Should we Systematically Measure Plasma Magnesium Levels in the Treatment of Severe Preeclampsia/Eclampsia?
Aim: To show that measuring magnesium levels optimizes magnesium sulfate treatment in severe preeclampsia/eclampsia. Subjects and methods: A retrospective study was conducted with severe preeclampsia/eclampsia patients who have been treated with magnesium sulfate and have received magnesium in biological monitoring. Results: Ten patients were treated for severe pre-eclampsia/eclampsia during the study period. Of these, six patients with, an average age of 27.5 years had their plasma magnesium measured through treatment monitoring. The average rate of ionized magnesium was 1.4 (1-13.6 mEq/l). Plasma levels were supratherapeutic (> 4 mmol/l) for two patients. The other four patients had subtherapeutic plasma levels. Clinical signs of overdose were seen in one case, where plasma magnesium levels were 1,8mEq/l. At admission, the average systolic blood pressure was 137.5mmHg (120-147mmHg), and the average diastolic blood pressure was 80.5 mmHg (69-106mmHg). Complications included hemodynamic pulmonary edema (2 cases) and nosocomial bacterial pneumonia (1 case). The average length of stay was 4 days (1-8 days), and there was no hospital mortality. Conclusion: The results suggest a need for systematic measurement of plasma magnesium levels in severe preeclampsia/eclampsia treated with magnesium sulfate. A larger study is needed to build consensus regarding this practice.
Introduction
Magnesium sulfate administration is essential in the treatment of severe preeclampsia/eclampsia [1, 2, 3]. The treatment monitoring is essentially clinical, except in cases of renal failure [4, 5]. However, acute renal failure may be included in the clinical picture of severe preeclampsia/eclampsia. This purely clinical approach seems to underestimate actual frequency of magnesium overdose in the treatment of severe preeclampsia/eclampsia. Thus, through this reports of clinical series, we want to check the relevance of clinical examination in detecting magnesium overdose signs in severe preeclampsia/eclampsia with measuring magnesium plasma levels.
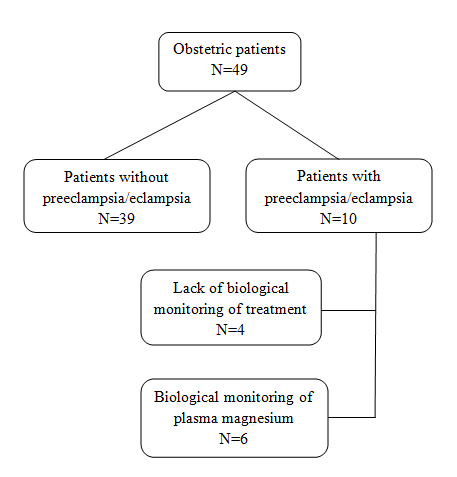
| Figure 1: Inclusion scheme of the patients in the | ||
| study. | ||
Patients and Methods
This is a retrospective study of all patients that were hospitalized in surgical intensive care from 2008 to 2013 for severe preeclampsia/eclampsia and received magnesium sulfate treatment with a biological monitoring of magnesium levels. The approval of the ethics committee was required. For the inclusion of patients, we conducted a study of clinical records of obstetric patients. From this set, severe preeclamptic/eclamptic patients were identified. We then turned our attention to patients whose magnesium had been measured through treatment monitoring (Figure 1). The definitions of severe preeclampsia/eclampsia are those given by scholarly associations [4]. The magnesium sulfate was administered according to the protocol of the French Society of Anesthesia and Intensive Care [6]. The recommended therapeutic concentrations are between 2 and 4 mmol/l (4 and 8 mEq/l) [4]. The data is expressed in averages (first quartile-third quartile).
Results
Ten patients were admitted for severe preeclampsia/eclampsia. Six of them had received biological monitoring of magnesium sulfate treatment (Figure 1).
From these measurements, we point out that magnesium was above therapeutic concentrations in two patients, while it was below the therapeutic range for the other four patients (Table 1). Paradoxically, signs of overdose were present in only one patient, with magnesium levels at 1.8 mEq/l. additionally; the duration of treatment was practically identical in five of the patients that were treated for severe preeclampsia/eclampsia. For the sixth, the treatment duration was very brief (one hour) and the magnesium levels were low. In this patient, hereditary hypofibrinogenemia was ultimately diagnosed. Systolic blood pressure at admission was moderate (≥ 90 mmHg and < 110 mmHg) for three patients. Diastolic blood pressure was severe (> 110 mmHg) for one patient and moderate (≥ 90 mmHg < 110 mmHg) for another. Caesarean section performed under general anesthesia was the most frequent mode of delivery (5 cases). A history of fetal death and preeclampsia were present in two and three cases, respectively. The average lactate was 0.8mmol/l (0.7-2.0 mmol/l). Two patients were intubated and ventilated upon admission. Liver failure was present in three patients. The average rate of AST enzymes was 49 (21-763 IU/l) and the ALT, 21 (10-438 IU/l).
- Age (Years)
- Parity
- Comorbidities
- Renal
- Failure
- General
- Anesthesia
- Definitive
- Diagnosis
- Magnesemia (Meq/L)
- 1
- 28
- 1
- Yes
- Yes
- No
- Hypofibrinogenemia
- 0.9
- 1
- No
- 9
- 2
- 26
- 6
- Yes
- Yes
- Yes
- Eclampsia
- 1.0
- 48
- No
- 3
- 3
- 31
- 2
- Yes
- Yes
- Yes
- Severe preeclampsia
- 1.0
- 39
- No
- 4
- 4
- 36
- 1
- Yes
- Yes
- Yes
- Severe preeclampsia
- 1.8
- 51
- Yes
- 8
- 5
- 32
- 4
- Yes
- Yes
- Yes
- Severe preeclampsia
- 13.6
- 48
- No
- 3
- 6
- 23
- 2
- No
- Yes
- Yes
- Severe preeclampsia
- 15.0
- 53
- No
- 3
Table 2: Demographic and magnesium treatment characteristics (*): Length of stay.
Creatinine was high for all patients, with an average of 145 (76-183 µmol/l) (Table 2). The average prothrombinemia rate was 76%, and thrombocytopenia was present in five patients, including one severe case. Despite these organ failures, no deaths were recorded. The median length of stay in the ICU was 4 days (1-8 days). The complications that arose during these stays were hemodynamic pulmonary edema (2 cases) and nosocomial bacterial pneumonia (1 case).
| Median (First Quartile- | |||||
|---|---|---|---|---|---|
| Variables | |||||
| Third Quartile) | |||||
| Median age, years | 27.5 (26-32) | ||||
| Systolic blood pressure, mmHg | 137.5 (120-147) | ||||
| Diastolic blood pressure, mmHg | 80.5 (69-106) | ||||
| Mean blood pressure, mmHg | 97.5 (86-120) | ||||
| Pulse oximetry, % | 98.5 (98-100) | ||||
| Heart rate, bpm | 92 (88-116) | ||||
| Serum sodium concentration, mmol/l | 134 (133-135) | ||||
| Serum potassium, mmol/l | 4.4 (3.8-5.0) | ||||
| Calcium, mmol/l | 1.9 (1.0-2.0) | ||||
| Creatinine, µmol/l | 145 (95-183) | ||||
| Urea, g/l | 9 (6-11) | ||||
| ALT, IU/l | 21 (17-42) | ||||
| AST, IU/l | 49 (25-98) | ||||
| Total bilirubin, mg/l | 16.5 (8-21) | ||||
| Gamma glutamyl- transferase, IU/l | 18 (12-23) | ||||
| Lipase, IU/l | 29 (21-31) | ||||
| Amylase, IU/l | 96 (84-108) | ||||
| Lactate, mmol/l | 0.8 (0.7-1.5) | ||||
| Alkaline phosphatase IU/l | 221 (70-372) | ||||
| pH | 7.40 (7.37-7.46) | ||||
| PaO , mmHg 2 | 132.5 (97-161) | ||||
| PaCO , mmHg 2 | 30.5 (29-33) | ||||
| Bicarbonates, mEq/l | 20 (19-22) | ||||
| TP, % | 76 (70-94) | ||||
| Platelets count, 1012 /l | 95 (43-143) |
Table 3: Clinical and biological characteristics.
Discussion
The improvement of obstetric care has undoubtedly contributed to the reduced frequency of female admissions to the ICU. However, this study had the risk of being a small sample size. Over an observation period of six years, only six patients met the inclusion criteria set out in our work. Despite this, the information drawn from this study cannot be seen as any less important. First, therapeutic concentrations can be surpassed quickly with the administration protocol developed by scholarly associations [6, 7]. The role of initial renal failure can then be discussed. Dose reduction is suggested by urinary magnesium excretion reduction [8]. In addition, four patients had subtherapeutic plasma concentrations, and eclampsia was diagnosed in one of these patients. Underdosing may have played a role. Second, the absence of severe clinical presentations related to magnesium sulfate overdose as reported in numerous scientific works, and where the monitoring of treatment was limited to clinical examination alone, should under no circumstances discourage the biological examination. Indeed, there is no parallel between the clinical signs and the plasma concentration of magnesium.
The choice between the measurement of ionized or non-ionized magnesium remains under debate. For some authors, the ionized magnesium measurement seems essential because of pathophysiological changes induced by the disease; for others, however, the biological determination in one form or another was sufficient because of the correlation that exists between the two [4, 9, 10]. Third, early treatment of severe preeclampsia/eclampsia based on clinical presumption can turn out to be unjustified. Indeed, symptoms and clinical signs of the disease can be included in the clinical picture of many other conditions [8]. One of our patients had early treatment with magnesium sulfate based on the clinical presumption of severe preeclampsia. This fact highlights the need for a rigorous management approach, which must take into account different diagnoses. The observed complications, nosocomial bacterial pneumonia and hemodynamic pulmonary edema, would be the consequences of severe preeclampsia/eclampsia. Additionally, it may be accompanied by neurological issues of varying degrees, exposing the patient to the risk of pulmonary aspiration and secondary pneumonia. Moreover, increased systemic vascular resistance, an essential component of high blood pressure in preeclampsia/eclampsia, exposes the left ventricular to dysfunction. This is compounded by the reduction of edema and vascular filling often in hypovolemic patients [11, 12, 13, 14, 15, 16, 17]. If persistent hypertension (10.4%), generalized edema (7.1%) and severe thrombocytopenia (6.2%) were the major complications in the Kuwaiti study, in other studies they were represented by pulmonary edema, acute renal failure, aspiration pneumonia and cardiac arrest [11, 12, 18, 19]. Moreover, the demographic characteristics of our patients do not differ from those of other authors [16, 18]. Conclusion In light of the above, monitoring magnesium plasma concentration in the treatment of severe preeclampsia/eclampsia seems necessary as underdosing and overdosing remain possible. However, the weakness of our numbers prevents us from making a recommendation in this regard. Conducting a larger study will undoubtedly create a consensus concerning this aspect of therapeutic care. References
1. Do women with pre-eclampsia and their babies, benefit from magnesium sulphate? The Magpie trial (2002) a randomized placebo-controlled trial. The Magpie trial collaborative group. Lancet 2002; 359:1877-1890. 2. Duley L, Gülmezoglu AM, Henderson-Smart DJ, Chou D (2010) Magnesium sulphate and other anticonvulsants for women with pre-eclampsia. Cochrane Database Syst Rev10 (11):CD000025. 3. Duley L. (2005) Evidence and practice: the magnesium sulphate story. Best Pract Res Clin Obstet Gynaecol 19(1): 57-74. 4. Girard B, Beucher G, Muris C, Simonet T, Dreyfus M. J.
(2005) Magnesium sulphate and severe preeclampsia : its use in current practice Gynecol Obstet Biol Reprod 34(1pt1):17 – 22. 5. Lowe S, Bowyer L, Lust K, McMahon L, Morton M, North R, et al. (2014) The SOMANZ guideline for the management of hypertensive disorders of pregnancy. Society of Obstetric Medicine of Australia and New Zealand 55(1): 11-16 . http://somanz.org (available 18/02/2016). 6. Diemunsch P, Langer B, Noll E. (2010) Intrahospital management of women with preeclampsia. Ann Fr Anesth Reanim 29(4): 51-58. 7. The Eclampsia Trial Collaborative Group. Which anticonvulsant for women with eclampsia? Evidence from the Collaborative Eclampsia Trial. Lancet 1995 345:1455–63. 8. Sibai BM. (2005) Diagnosis, prevention, and management of eclampsia. Obstet Gynecol 105(2):402-410. 9. Taber EB, Tan L, Chao CR, Beall MH, Ross MG. (2002) Pharmacokinetics of ionized versus total magnesium in subjects with preterm labor and preeclampsia. Am J Obstet Gynecol 1869(5):1017-1021. 10. Yoshida M, Matsuda Y, Akizawa Y, Ono E, Ohta H.
(2006) Serum ionized magnesium during magnesium sulfate administration for preterm labor and preeclampsia. Eur J Obstet Gynecol Reprod Biol 128(1-2):125-128. 11. Mattar F, Sibai BM. (2000) Eclampsia VIII: risk factors for maternal morbidity. Am J Obstet Gynecol 182(2):307-312. 12. Douglas KA, Redman CW. (1994) Eclampsia in United Kingdom. BMJ 309(6966):1395-1400. 13. Visser W, Wallengurg HC. (1991) Central hemodynamic observations in untreated preeclamptic patients. Hypertension 17(6 Pt 2): 1072-1077. 14. Lambert G, Brichant JF, Hartstein G, Bonhomme V, Dewandre PY. (2014) Preeclampsia: an update. Acta Anaesthesiol Belg 65(40): 137-149. 15. Melchiorre K, Thilaganathan B. (2011) Maternal cardiac function in preeclampsia. Curr Opin Obstet Gynecol; 23(6): 440-447. 16. Melchiorre K, Sutherland GR, Baltabaeva A, Liberati M, Thilaganathan B. (2011) Maternal cardiac dysfunction and remodeling in women with preeclampsia at term. Hypertension 57(1): 85-93. 17. Omu AE, Al-Harmi J, Vedi HL, Mlechkova L, Sayed AF.
(2008) Magnesium sulphate therapy in women with pre-eclampsia and eclampsia in Kuwait. Med Princ Pract 17(3): 227-232. 18. Lopez-Llera M. (1992) Main clinical types and subtypes of eclampsia. Am J Obstet Gynecol 166(1pt1): 4-9.
19. Rozenberg P. (2006) Magnesium sulphate for the management of preeclampsia. Gynecol Obstet Fertil 34(1): 54-59.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index