Use of Proseal Laryngeal Mask Airway in Contrast to Endotracheal Tube for Routine Laparoscopic Cholecystectomy under General Anaesthesia-A Randomized Comparative Study
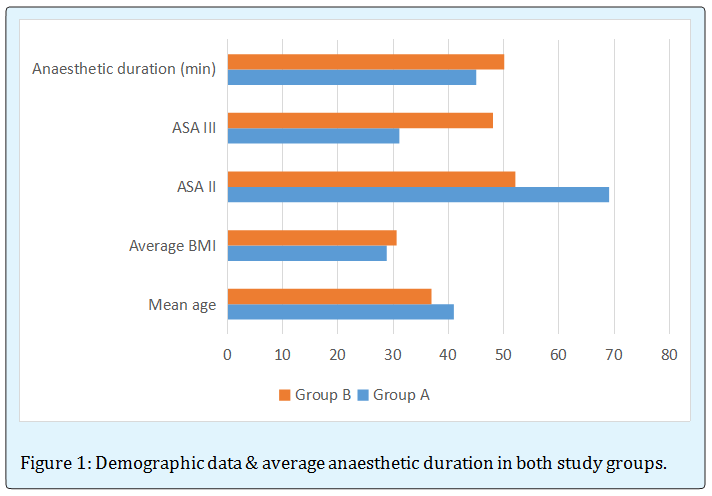
Evidence based data in the very recent years suggest that in spite of tremendous advances in contemporary anaesthetic practice, advances, airway management continue to be of paramount importance to anesthesiologists. In this RCT (Randomized Control Clinical Trial), the ultimate aim was to depict the anaesthetic safely of the patients of routine laparoscopic cholecystectomy (ASA II & III) in terms of haemodynamic and laryngeal adverse outcomes in BIRDEM General Hospital, Bangladesh. A total number of 200 patients (100 patients with endotracheal tube & 100 patients with LMA) were selected on the basis of simple random sampling. In each patient, after preoxygenation, anaesthesia was introduced with propofol, fentanyl and vecuronium. Anaesthesia was maintained with N2O, O2, Halothane and vecuronium. Ventrilation was set at 8 ml/kg and respiratory rate was 12/min. The ultimate result of this study suggest that in Group A (ETT group), mean±SD of age was 41±1.1 and in Group B (LMA group), it was 37±1.7. Demographic status suggests that the average BMI in both groups were 28.9 and 30.6 respectively. In ETT group, majority of patients (69%) had ASA grade II, in contrast, in LMA group, it was 52%. Average anaesthetic duration in both group were 45 & 50 minutes respectively. There found no significant difference in haemodynamic parameter between both groups at different phases of peroperative period. Laryngeal complications, like tube leakage and gastric insufflation were found in 2 & 3 patients respectively with the use of LMA. Regarding laryngeal morbidity following tube removal, coughing and trauma to lip, teeth, and tongue were slightly higher in with ETT than LMA tube. The incidence of sore throat was slightly higher with the use of LMA (07%) in contrast to ETT (05%), but complications like dysphagia, dysphonia, and dysarthia were found to be same in both groups. P-values suggest less significant result here.
Faruquzzaman
MS Part 3 (Thesis) Course Student BIRDEM Hospital, Bangladesh
were found to be same in both groups. P-values suggest less significant result here.
Keywords: Laryngeal mask airway; Endotracheal tube; Laparoscopic cholecystectomy
Introduction
Laryngeal mask airway (LMA) was introduced by Dr. Brain in 1980s and caused a revolution in airway management [1]. Today, this device has a special position in anesthesiology procedures and among many of anesthesiologists [2, 3]. LMA provides a proper way for ventilating the patient while protecting his or her airway [4]. Nowadays, LMA is used as a proper device for protecting the patient’s airway during many of the operations [5, 6]. However, American society of anesthesiologists [3, 7, 8] Australian and European council of resuscitation, and American heart Association [9, 10, 11] approve the usage of LMA only in emergency situations and in cardio-pulmonary resuscitation. The reason for this issue seems to be the inadequate evidence on the efficacy and safety of LMA. Many studies were conducted on usage of LMA for protecting the patients’ airway during surgery and showed that this device has many benefits including easier insertion, no need for laryngoscope [12], fewer homodynamic complications [13], and less harmful complication for the larynx and vocal cords[14]. Furthermore, LMA is better tolerated by patients [15] and learning of its usage is easy for physicians and other health care providers [16, 17, 18, 19, 20]. Also, LMA is a cost beneficent device [21]. It needs to be mentioned that some complications have also been reported for LMA. The most important of these complications are related to digestive system including vomiting and aspiration [12, 22] and to larynx including sore throat, coughing, vocal cord paralysis [23, 24], and acute epiglottis [25]. Complications such as nausea and vomiting and laryngeal complications such as coughing and sore throat are most common complications after general anesthesia. Nausea and vomiting usually happen in one third of patients after the general anesthesia [26] and can be followed by serious complications such as aspiration, pneumonia and even rupture of esophagus [27]. The sore throat and other laryngeal complications also happen in 60% of patients in the post general anesthesia period [28]. It should be mentioned that such complications can result in delay of patients' discharge, increased health care costs, and decreased patients’ satisfaction [29, 30, 31, 32, 33, 34, 35, 36, 37, 38]. Therefore, any effort taken to decrease such complications would be important. Several studies have been conducted related to comparison the cardio- respiratory, digestive and laryngeal perioperative Faruquzzaman. Use of Proseal Laryngeal Mask Airway in Contrast to Endotracheal Tube for Routine Laparoscopic Cholecystectomy under General Anaesthesia- A Randomized Comparative Study. Anaesth Critic Care Med J 2016, 1(3): 000115.
complications by using ETT and LMA. In a group of studies no difference has been observed in perioperative complications. For example, in a study conducted by Splinter and Small man, no difference was indicated between ETT and LMA regarding the sore throat and coughing in the perioperative period [39]. Other studies have indicated that the risk of complication after use of LMA were further than ETT [40, 41]. Finally, some other studies have reported that a risk of nausea, vomiting [42], sore throat [43, 44, 45, 46, 47, 48], and coughing [49, 50] after use of LMA were less than ETT. As it turned out, in spite of the increase in the application of LMA, there is still controversy about the efficacy of LMA in comparison to ETT. This problem restricts the wide application of LMA. Therefore, the aim of present study was to compare the perioperative cardi-respiratory, digestive (nausea and vomiting) and laryngeal (sore throat and coughing) complications by using ETT and LMA in perioperative period of selective laparoscopic cholecystectomy under general anaesthesia.
Materials and Methods
This randomized controlled clinical trial was designed to be conducted among the 200 patients (100 patients with endotracheal tube & 100 patients with LMA) of routine laparoscopic cholecystectomy in BIRDEM General Hospital, Bangladesh from a period of 15.11.2014 to 15.07.2016 with a view to depict the of safety of Laryngeal Mask Airway in contrast to Endotracheal Tube in terms of peroperative and immediate postoperative complications. Respective patients of 20 to 60 years age group with ASA II or III included as study population. Different pathology (for which operation was done), BMI, co-morbidity were confounding variable here. Patients with congenital anomaly and morbid obesity were excluded from study population. Simple random sampling was used as the sampling technique. In each patient, after preoxygenation, anaesthesia was introduced with propofol, fentanyl and vecuronium. Anaesthesia was maintained with N2O, O2, Halothane and vecuronium. Ventrilation was set at 8 ml/kg and respiratory rate was 12/min. Patients with endotracheal tube (ETT) were included in Group a (Control group) & patients with LMA were in Group B (Experimental group). Data were processed, presented in tabulated form and discussed with compare & comparison on the basis of statistical analysis.
Copyright© Faruquzzaman
Results
Age and sex distribution of both group of patients is depicted in Table 1 which suggests that majority (47%) of the patients of Group A were in 40 to 50 years age group whereas, in a case of Group B, most of the patients (35%) were in group B.
| Group A (n=100) | Group B (n=100) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age in years | No. of patients | % | Mean±SD | No. of patients | % | Mean±SD | ||||||
| 20-30 | 13 | 13 | 41±1.1 | 17 | 17 | 37±1.7 | ||||||
| 30-40 | 24 | 24 | 19 | 19 | ||||||||
| 40-50 | 47 | 47 | 35 | 35 | ||||||||
| 50-60 | 16 | 16 | 29 | 29 | ||||||||
| Total | 100 | 100 | 100 | 100 |
Table 1: Laryngeal morbidity in Group A & B.
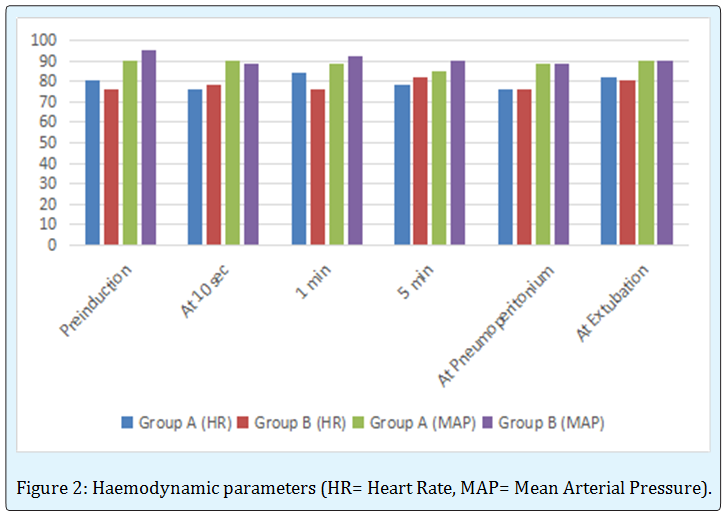
Haemodynamic status in different time of peroperative period is represented in Figure 2 in terms of heart rate (HR) and mean arterial pressure (MAP).
Faruquzzaman. Use of Proseal Laryngeal Mask Airway in Contrast to Endotracheal Tube for Routine Laparoscopic Cholecystectomy under General Anaesthesia- A Randomized Comparative Study. Anaesth Critic Care Med J 2016, 1(3): 000115.
Copyright© Faruquzzaman
Laryngeal morbidity at different phases is represented in Table 2 which suggests no significant difference between the findings in ETT and LMA groups. P-values are statistically less significant here.
| Group | Group | P- | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | value | |||||||||
| Intraoperative | |||||||||||
| Leak | --- | 02 | 0.5 | ||||||||
| Gastric insufflation | --- | 03 | |||||||||
| Aspiration, regurgitation | --- | 00 | |||||||||
| At removal | |||||||||||
| Coughing | 07 | 04 | 0.4 | ||||||||
| Blood stain device | 05 | 05 | |||||||||
| Trauma to lip, teeth, tongue | 04 | 01 | |||||||||
| Postoperative | |||||||||||
| Vomiting | 01 | 01 | 0.5 | ||||||||
| Sore throat | 05 | 07 | |||||||||
| Dysphagia, dysphonia, dysarthia | 00 | 00 |
Table 2: Laryngeal morbidity in Group A & B.
Faruquzzaman. Use of Proseal Laryngeal Mask Airway in Contrast to Endotracheal Tube for Routine Laparoscopic Cholecystectomy under General Anaesthesia- A Randomized Comparative Study. Anaesth Critic Care Med J 2016, 1(3): 000115.
Discussion
In Group A (control group), majority of the patients (47 out of total 100 patients) were in 40 to 50 years of age group followed by 24 patients (out of total 100 patients) were in 30 to 40 years age group. Mean±SD of age in this group was 41±1.1, in contrast, in experimental group, most of the patients were in (35 out of total 100 patients) were in 40 to 50 years of age group followed by 29 patients (out of total 100 patients) were in 50 to 60 years age group. Mean±SD of age in this group was 37±1.7. Demographic data (Figure 2) suggests that the average BMI in both group were 28.9 and 30.6 respectively. In ETT group, most of the patients (69%) had ASA grade II, whereas in LMA group 52% patients had ASA grade II. Average anaesthetic duration in both group were 45 & 50 minutes respectively. Haemodynamic status in both groups in terms of heart rate and mean arterial pressure was depicted in figure 2 which suggest no significant difference in between both groups at different phases of peroperative period. In question of laryngeal complications, table 2 suggests that tube leakage and gastric insufflation were found in 2 & 3 patients respectively with the use of LMA. No case of regurgitation and aspiration was recorded. Regarding the issue of Copyright© Faruquzzaman
laryngeal morbidity immediately following removal of tube, it was reflected that coughing and trauma to lip, teeth, tongue were slightly higher in Group A an contrast to Group B. But the prevalence of blood stain on device found same (05%) in both groups. The incidence of sore throat was slightly higher with the use of LMA (07%) in comparison to ETT (05%), but postoperative complications like dysphagia, dysphonia, and dysarthia were recorded to be same in both groups. P-values suggest less significant result here. In a study of Namita S et al. [51]. It was found that in case of haemodynamic status, there was no significant comparative result between ETT and LMA groups also. In issue of Intraoperative laryngeal morbidity, the prevalence of tube leakage and gastric insufflation were 1 case and 3 cases respectively in LMA group, whereas, regarding postoperative sore throat, it was recorded to be slight higher in LMA group (07%). But following removal of tube, the difference of laryngeal complications in between both groups suggests less significant result.
Conclusion
In summary, the result of this study is highly suggestive of the effectiveness and safety of LMA tube in terms of per and postoperative haemodynamic and laryngeal complications in comparison to endotracheal tube.
References
-
Wemyss-Holden SA, Porter KJ, Baxter P, Rudkin GE, Maddern GJ (1999) The laryngeal mask airway in experimental pig anesthesia. Laboratory Animals 33(1): 30-34.
-
Asai T, Morris S (1994) the laryngeal mask airway: its features, effects and role. Can J Anaesth 41 (10): 930- 960.
-
Shung J, Avidan MS, Lng R, Klien DC, Pott L (1998) awake intubation of the difficult airway with the intubating laryngeal mask airway. Anaesthesia 53(7): 645-649.
-
Frascone RJ, Heegaard W, Pippert G, Dries D, Molinari P, et al. (2008)Use of the Intubating Laryngeal Mask Airway in HEMS. Air Medical Journal 27 (4): 1852- 1854.
-
Golshevsky J, Cormack J (2009) Laryngeal mask airway device during coiling of unruptured cerebral Faruquzzaman. Use of Proseal Laryngeal Mask Airway in Contrast to Endotracheal Tube for Routine Laparoscopic Cholecystectomy under General Anaesthesia- A Randomized Comparative Study. Anaesth Critic Care Med J 2016, 1(3): 000115. aneurysms. Journal of Clinical Neuroscience 16(1): 104-105.
-
Komatsu R, Nagata O, Kamata K, Yamagata K, Sessler I, et al. (2005) Comparison of the intubating laryngeal mask airway and laryngeal tube placement during manual inline stabilisation of the neck. Anaesthesia 60(2): 113-117.
-
Raphael J, Rosenthal-Ganon T, Gozal Y (2004) Emergency Airway Management with a Laryngeal Mask Airway in a Patient Placed in the Prone Position. Journal of Clinical Anesthesia 16(7): 560-561.
-
Zoremb M, Aust H, Eberhart L, Braunecker S, Wulf H (2009) Comparison between intubation and the laryngeal mask airway in moderately obese adults. Acta Anaesthesiol Scand 53(4): 436-442.
-
Wilson GD, Sittig SE, Schears GJ (2008) The laryngeal mask airway at altitude. The Journal of Emergency Medicine 34(2): 171-174.
-
Gibbons AJ, Evans MJ, Fenner SG, Grew NR (2005) the use of the laryngeal mask in surgical tracheotomy. British Journal of Oral and Maxillofacial Surgery 43(1): 87-88.
-
Heina C, Owen H, Plummer J (2008) a 12- month audit of laryngeal mask airway (LMA) use in a South Australian ambulance service. Resuscitation 79(2): 219-224.
-
Yong S, Soo-Kyung P, Young-Pyo C, Yoo- Sun C, Jin- Young A, et al. (2002) Effect of Laryngeal Mask Airway on Esophageal Motility During General Anesthesia. Journal of Clinical Anesthesia 14(7): 518- 523.
-
Shah EF, Allen JG, Greatorex RA (2001) Use of the laryngeal mask airway in thyroid and parathyroid surgery as an aid to the identification and preservation of the recurrent laryngeal nerves. Ann R Coll Surg Engl 83(5): 315-318.
-
Trevisanuto D, Micaglio M, Pitton M, Magarotto M, Piva D, et al. (2006) Laryngeal mask airway: Is the management of neonate’s requiring positive pressure ventilation at birth changing? Resuscitation 62(2): 151-157. Copyright© Faruquzzaman
-
Gandini D, Brimacombe J (2004) Manikin training for neonatal resuscitation with the laryngeal mask airway. Paediatr Anaesth 14 (6): 493-494.
-
Brimacombe J (1995) the advantages of the LMA over the tracheal tube or facemask: a meta-analysis. Can J Anaesth 42 (11): 1017-1023.
-
Reinhart DJ, Simmons G (1994) Comparison of placement of the laryngeal mask airway with endotracheal tube by paramedics and respiratory therapists. Ann Emerg Med 24 (2): 260–263.
-
Weksler N, Tarnopolski A, Klein M, Shily M, Rozentsveig V, et al. (2005) Insertion of the endotracheal tube, laryngeal masks airway, and oesophageal-tracheal Combitube: a 6-month comparative prospective study of acquisition and retention skills by medical students. Eur J Anaesthesiol 22(5): 337-340.
-
Burgoyne L, Cyna A (2001) Laryngeal mask vs. intubating laryngeal mask: insertion and ventilation by inexperienced resuscitators. Anaesth Intensive Care 29(6): 604-608.
-
Dries D, Frascone R, Molinari P, Heegaard W, Pippert G, et al. (2001) Does the ILMA make sense in HEMS? Air Med J 20(5): 35-37.
-
Goodman EJ, Christenson E, Douglas AM, Ziegler EJ, Lewis BR (2008) Reusable Laryngeal Mask Airways can be used more than 40 times. Journal of Clinical Anesthesia 20: 109-115.
-
Nanji GM, Maltby JR (1992) Vomiting and aspiration pneumonitis with the laryngeal mask airway. Can J Anaesth 39 (1): 69-70.
-
Mclure HA (1996) Vocal cord paralysis and a laryngeal mask airway. Anai srhesia 51: 1079.
-
Endo K, Okabe Y, Maruyama Yumiko, Tsukatani T, Furukawa M (2007) Bilateral vocal cord paralysis caused by laryngeal mask airway. American Journal of Otolaryngology–Head and Neck Medicine and Surgery 28(2): 126-129.
-
Seid Hejazie M (2007) Severe Epiglottis edema after laryngeal mask airway ventilation. Rawal Med J 32(2): 199-200. Faruquzzaman. Use of Proseal Laryngeal Mask Airway in Contrast to Endotracheal Tube for Routine Laparoscopic Cholecystectomy under General Anaesthesia- A Randomized Comparative Study. Anaesth Critic Care Med J 2016, 1(3): 000115.
-
Gan TJ (2002) Postoperative nausea and vomiting- and it be eliminated? JAMA 287(10): 1233-1236.
-
Apfel CC, Korttila K, Abdalla M, Kerger H, Turan A, et al. (2004) A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med 350(24): 2441-2451.
-
Mande H, Nikolajsen L, Lintrup U, Jepsen D, Mfilgaard J (1992) Sore throat after endotra cheal intubation. Anesth Analg 74(6): 897-900.
-
Baric A (2000) Oesophageal rupture in a patient with postoperative nausea and vomiting. Anaesth Intens Care 28(3): 325-327.
-
Hirsch J (1994) Impact of postoperative nausea and vomiting in the surgical setting. Anaesthesia 49: 30– 33.
-
Dexter D, Tinker JH (1995) Analysis of strategies to decrease postanesthesia care unit costs. Anesthesiology 82(1): 94-101.
-
Andrews PLR (1992) Physiology of nausea and vomiting. Br J Anaesth 69(1): 2S-19S.
-
Metter SE, Kitz D, Young M et al. (1987) Nausea and vomiting after outpatient laparoscopy: incidence, impact on recovery stay and cost. Anesth Analg 66: 116S.
-
Patel RI, Hannallah R (1988) Anesthetic complications following pediatric ambulatory surgery: a 3-year study. Anesthesiology 69(6): 1009- 1012.
-
Meeks GR, Waller GA, Meydrech EF (1992) Unscheduled hospital admission following ambulatory gynecologic surgery. Obstet Gynecol 80(3): 446-450.
-
Camu F, Lauwers M, Verbessen D (1992) Incidence and aetiology of postoperative nausea and vomiting. Eur J Anaesth 9: 25-32.
-
Fisher DM (1997) The “Big Little Problem” of Postoperative Nausea and Vomiting. Anesthesiology 87: 1271-1273.
-
Myles P, Williams DL, Hendrata M (2000) Patient satisfaction after anaesthesia and surgery: results of a Copyright© Faruquzzaman prospective survey of 10,811 patients. Br J Anaesth 84(1): 6-10.
-
Splinter WM, Smallman B, Rhine EJ, Komocar L (1994) Postoperative sore throat in children and the laryngeal mask airway. Can J Anaesth 41 (11): 1081- 1083.
-
Swann DG, Spens H, Edwards SA, Chestnut RJ (1993) Anaesthesia for gynaecological laparoscopy-a comparison between the laryngeal mask airway and tracheal intubation. Anaesthesia 48(5): 431-434.
-
Kumagai A, Iwasaki H, Kawana S, Namiki A (1996) Laryngeal mask airway does not reduce the incidence of post-operative nausea and vomiting after gynaecological surgery. Anesth Analg 81: S255.
-
Klockgether-Radke A, Gerhardt D, Muhlendyck H, Braun U (1996) The effect of the laryngeal mask airway on the postoperative incidence of vomiting and sore throat in children. Anesthetist 45(11): 1085- 1088.
-
Zimmert M, Zwirner E, Braun KU (2007) Effects on vocal function and incidence of laryngeal disorder when using a laryngeal mask airway in comparison with an endotracheal tube. European Journal of Anaesthesiology 16 (8): 511-515.
-
Smith I, White PF (1992) Use of the laryngeal mask airway as an alternative to a face mask during outpatient arthroscopy. Anesthesiology 77(5): 850- 855. Faruquzzaman. Use of Proseal Laryngeal Mask Airway in Contrast to Endotracheal Tube for Routine Laparoscopic Cholecystectomy under General Anaesthesia- A Randomized Comparative Study. Anaesth Critic Care Med J 2016, 1(3): 000115.
-
Akhtar TM, McMurray P, Ken WJ, Kenny GNC (1992) A comparison of laryngeal mask airway with tracheal tube for intra-ocular ophthalmic surgery. Anaesthesia 47(8): 668-671.
-
Alexander CA, Leach AB (1989) Incidence of sore throats with the laryngeal mask (Letter). Anaesthesia 44(9): 791.
-
Swann DG, Spens H, Edwards SA, Chestnut RJ (1993) Anaesthesia for gynaecological laparoscopy - a comparison between the laryngeal mask airway and tracheal intubation. Anaesthesia 48: 431-434.
-
Brain AIJ, McGhee TD, McAteer EJ, Thomas A, Abu- Saad MAW, et al. (1985) the laryngeal mask airway. Development and prelimimary trials of a new type of airway. Anaesthesia 40(4): 356-361.
-
Sarma VJ (1990) The use of a laryngeal mask airway in spontaneously breathing patients. Acta Anaesthesiol Scand 34(8): 669-672.
-
McCrirrick A, Ramage DT, Pracilio JA, Hickman JA (1991) Experience with the laryngeal mask airway in two hundred patients. Anaesth Intensive Care 19(2): 256-260.
-
Namita S, Aditya K, Abhijeet M, Amrita gupta, Gyan saurabh, et al. (2011) The comparison of proseal laryngeal mask airway and endotracheal tube in patients undergoing laparocopic surgeries under general anaesthesia. Indian Journal of Anaesthesia, 55(2): 156-159. Copyright© Faruquzzaman
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index