A Comparison of Sterofundin and Ringer’s Lactate on Intraoperative Acid Base and Electrolytes Status in Children: A Randomized Controlled Trial
Background: Perioperative fluid management of pediatric patients is very challenging, as children are unable to cope with inappropriate water and electrolyte administration. Suboptimal fluid management leads to deleterious effects on cardiovascular stability and altered tissue perfusion. We evaluate the Intraoperative use of SterofundinÒas the main crystalloid in moderate to major pediatric surgery in comparison to Ringer’s lactate. The primary outcome was the changes of plasma pH from the start of surgery to the end of surgery. The secondary outcomes included changes of Intraoperative plasma electrolyte and Intraoperative hyper/hypoglycemia. Methodology: A total of 30 children aged between 1-13 years old, were enrolled and randomized into two arms, to receive Sterofundin or Ringer’s Lactate intraoperatively. Children with renal, cardiac or liver dysfunction, hypervolemia states, electrolyte imbalance and metabolic acidosis were excluded. Acid-base status, electrolyte balance and hemodynamic variables were recorded at baseline and repeated every hour until one hour postoperatively. Results: In Ringer’s Lactate group, the mean difference in pH between the baseline and end of surgery was 0.07±0.06 (p=0.001, 95% CI 0.03-0.09) and in Sterofundin group the mean difference in pH was 0.05±0.06 (p=0.010, 95% CI 0.01- 0.08). For base excess (BE), the mean difference in BE between the baseline and end of surgery was1.664±2.694(p=0.035) in Ringer’s Lactate group while in Sterofundin group the mean difference in BE is -1.331±3.327(p=0.175). Conclusion: The use of Sterofundin is better to Ringer’s Lactate in the management of Intraoperative acid base, electrolyte and hemodynamic parameters in pediatric patient undergoing major surgery.
Introduction
Perioperative fluid management in pediatrics is particularly challenging since children are less able to cope with inappropriate water and electrolyte administration compared to adults due to the immaturity of their organ systems. Major pediatric surgical procedures involving body cavities are associated with large fluid shifts between body compartments. Hence, anesthetists have to consider carefully the type and amount of intravenous fluid administered intraoperatively. Most of the fluids given Perioperative are used for replacing deficits and third space losses, which consist mainly of extracellular fluid [1]. Therefore, the hydrating solution should ideally have a composition of electrolytes as similar to plasma as possible. The safe prescription of Intraoperative fluids in pediatric surgical patients ensures optimal function of the cardiovascular system and sustains cellular physiology during a period of enormous stress. Undesirable and dangerous effects associated with moderate to severe derangement in electrolytes and pH balance, that may occur during surgery are related to the choice of intra operative fluids [2, 3]. Normal saline or colloids that are saline-based have issues with Hyperchloremic acidosis [4, 5]. The development of intravenous fluids has seen the progression to newer balanced fluids to better serve Perioperative fluid strategy. The compositions of Ringer’s Lactate (RL), Sterofundin(S) and 0.9% Sodium Chloride are shown in (Table 1). RL is a balanced solution with a similar composition to plasma with a potential base excess of 3 mmol/L [6]. Lactate was added to RL to reduce the chloride load and to act as a bicarbonate precursor, therefore reducing the likelihood of Hyperchloremic acidosis seen after larger infusions of normal saline. However, the metabolism of lactate is dependent on the kidney and liver. Hence when the functions of those organs are compromised, there will be lactate accumulation as well as reduction in the production of bicarbonate that may result in lactic acidosis. ISO, B.Braun, Melsungen, Germany is a balanced isotonic solution for• Sterofundin intravenous infusion with electrolyte composition very similar to plasma with a potential base excess of zero [7]. It contains acetate and maleate, which is widely metabolized in all organs and muscles. In adult patients Sterofundin has been shown to be associated with a better preservation of electrolyte and acid-base pattern compared to RL [6]. However, data on Sterofundin use in the pediatric population remains limited. It is shown to protect young children who underwent major surgery against the risk of increasing plasma chlorides and the subsequent metabolic acidosis in comparison to normal saline [8].
| Electrolyte | Plasma | 0.9% Nacl | Ringer’s Lactate | Sterofundin® | ||||||||||
| Sodium | 140 | 154 | 131 | 140 | ||||||||||
| Potassium | 5 | 0 | 5 | 4 | ||||||||||
| Chloride | 100 | 154 | 111 | 127 | ||||||||||
| Calcium | 2.2 | 0 | 2 | 2.5 | ||||||||||
| Magnesium | 1 | 0 | 1 | 1 | ||||||||||
| Bicarbonate | 24 | 0 | 0 | 0 | ||||||||||
| Lactate | 1 | 0 | 29 | 0 | ||||||||||
| Acetate | 0 | 0 | 0 | 24 | ||||||||||
| Maleate | 0 | 0 | 0 | 5 |
Table 1: Electrolyte composition (mmmol/L) of commonly available crystalloids. (Adapted from Guidet, et al. 2010 [7]. In this stu
Table 1: Electrolyte composition (mmmol/L) of commonly available crystalloids. (Adapted from Guidet, et al. 2010 [7]. In this study, our primary objective is to determine any significant differences in acid base balance in pediatric patients administered with these two different types of fluids. The secondary objectives are to determine any significant differences in electrolyte balance, incidence of hyper/hypoglycemia and hemodynamic stability between the two groups.
Methodology
The study was approved by our institutional review board (approval no. 823.9) and registered to trial registration on the Australian New Zealand Clinical Trials Registry [ACTRN12612000107820]. All parents of the patients gave their written consent. We enrolled 30
children of American Society Anesthesiologists physical status I- III, aged between 1-13 years who underwent moderate to major elective surgery in our pediatric surgical centre. This included laparotomies, gynecological and urological surgery, orthopedic, plastic and spine surgery that lasted for more than 2 hours. The surgeries were elective and patients were optimized according to standards of care in their individual wards. Major fluid shift was expected during surgery and where appropriate, blood was grouped and saved. We excluded patients with renal failure or impairment, cardiac or liver failure, anomalies of the heart, hypervolemia states, severe generalized oedema, electrolyte imbalance, and metabolic acidosis. Patients were randomized into two groups, Group RL vs Sterofundin, using a computer generated random number table, in blocks of ten. After recruitment, the enrolling investigators opened sealed opaque envelopes that concealed group allocation. Participants, trial investigators, attending anesthetists providing general anesthesia for the cases, and outcome assessors were blinded to group allocation. All patients were fasted for six hours and clear fluids were allowed to 2 hours prior to surgery. Based on the randomization, all patients received 10ml/kg bolus of Sterofundin or RL after induction of anaesthesia. For maintenance, the patients received the study fluids according to Holliday and Segar formula of 4-2-1 rule. (4 ml/kg/hr for the first 10 kg, 2 ml/kg/hr for 11 to 20 kg and 1 ml/kg.) For surgical replacement, the patients received fluids according to the severity of surgical trauma, that is, 2 to 4 ml/kg/hr for moderate trauma and 5 to 8 ml/kg/hr for severe trauma. Colloids (5 % human albumin) were used if blood loss was estimated to be more than 10% blood volume but less than 20% blood volume. Blood loss of more than 20% blood volume was replaced with packed red blood cells in a one to one ratio. The patients were monitored using standard monitoring devices, such as non-invasive blood pressure cuff, capnography and Electrocardiogram. Anaesthesia was induced with fentanyl (1-2 mcg/kg) and propofol (2mg/kg). Atracurium (0.5 mg/kg) or rocuronium (0.5- 0.6 mg/kg) was given for muscle relaxation and tracheal intubation. Anaesthesia was maintained with Sevoflurane in oxygen: air mixture (keeping MAC within 1.0-.1.2). An arterial line was inserted after induction in all patients for invasive monitoring of blood pressure and for blood sampling. Volume status was closely evaluated to maintain euvolaemia by clinical status i.e. Capillary return < 2 seconds, urine output of at least 1 ml/kg/hr, blood pressure and heart rate. Ventilation was adjusted to keep PaCO2 of 35- 45 mmHg. Every child received a forced-air warming device and core temperature was maintained at 36.0 to 37.0 °C. Hemoglobin was maintained between 9 to 10g/dl. We provided multimodal analgesia that included central neuroaxial blockade or regional techniques where possible, suppositories paracetamol or NSAIDs and intravenous opioid. Patients’ clinical data (age, gender, weight and surgical details) were recorded at enrollment. Blood pressure was recorded at 10-minute intervals for the first two hours and then every 30 minutes thereafter. Urine output, core temperature and capillary refill times were recorded hourly. Arterial blood gases were taken at the start (baseline) then hourly during surgery followed by the last measurement taken 1-hour postoperatively. The pH, pCO2, pO2, bicarbonate, base excess, sodium, chloride, glucose and hemoglobin levels were recorded from the arterial blood gas results.
Statistical Analysis
Sample size calculation: Our primary outcome measure was the change in plasma pH from the start of surgery to the end of surgery. It is shown that the normal physiological pH of mammalian arterial blood is strictly maintained at 7.40, and hence a decrease of more than 0.05 units from the normal pH results in acidosis [9]. To detect a difference in of 0.05 units in plasma pH from baseline to the end of surgery, power analysis at 80% and the 0.05 level of significance showed that a sample of 13 patients in each arm would be required. Therefore, we recruited 15 patients per group to account for dropouts and protocol breaches. Statistical analyses were performed using IBM SPSS Version 20 (SPSS Inc., Chicago, IL, USA). Continuous variables were tested for normality using the Shapiro- Wilk test. Differences at baseline characteristics were tested using independent t-tests for continuous variables and chisquare tests for categorical variables. The paired t- tests were used to compare the changes in measured variables from the baseline to end of surgery. A p value of<0.05 was deemed statistically significant.
Results
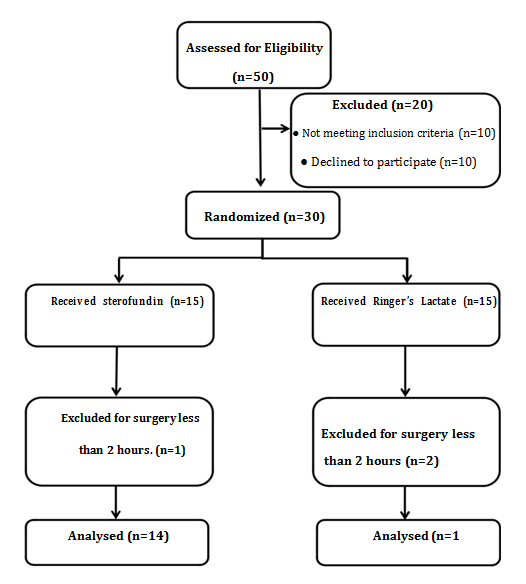
Fifty children were assessed for eligibility and approached for consent (Figure1). Thirty patients were then enrolled into the study and randomized into two arms. There were 15 patients in the RL group and 15 patients in the Sterofundin group. However, 3 patients were used, 14 in the RL group and 13 in the Sterofundin group. Their baseline characteristics are summarized in (Table 2).
| Variable | Ringer’s Lactate (n=14 | ) | Sterofundin (n=13) | P Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | |||||||||||
| Male/Female 7 /6 0.85 | 7/7 | 7/6 | 0.85 | ||||||||
| Age (in years) | 4.7±2.0 | 6.7±3.9 | 0.1 | ||||||||
| Weight (in kg) | 15.5±4.1 | 20.3±9.5 | 0.09 | ||||||||
| Duration of surgery (in hours) | 4.3±1.0 | 4.4±1.7 | 0.91 | ||||||||
| Amount of fluids administered (ml/kg/hr) | 36.9±17.5 | 37.1±20.5 | 0.97 | ||||||||
| Total volume blood transfused (ml/kg) | 48.6±77.6 | 34.6±85.1 | 0.66 |
Table 2: Baseline characteristics.
Our study showed that the reduction in plasma pH from the start of surgery to end of surgery in RL group is greater than the Sterofundin group (0.07±0.06, p=0.001, 95% CI 0.03, 0.09) 0.06 (p=0.010, 95% CI 0.01, 0.08). However, there is no significant acidosis (pH±vs. 0.05 < 7.25) detected in both group. There is also a significant decrease in BE (-1.66±2.69, p=0.035) observed in Ringer’s Lactate group from start of surgery to the end of surgery but not in Sterofundin group, BE (-1.33±3.33, p=0.175). In addition, there is a greater increase from baseline to the end of surgery, in RL group for Na (1.71±2.13, p=0.01) and Cl (2.36±2.84, p=0.008) as compared to Sterofundin group (Table 3).
| Ringer's Lactate (n=14) | Sterofundin (n=13) | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Start of | End of | Start of | End of | ||||||||||||||||||
| Variable | surgery | surgery | Change | P value | d | surgery | surgery | Change | P value | d | |||||||||||
| pH | 7.38 | 7.32 | 0.07±0.06 | 0.001 | 1.15 | 7.39 | 7.39 | 0.05±0.06 | 0.010 | 0.85 | |||||||||||
| BE | -4.00 | -5.66 | -1.66±2.69 | 0.035 | 0.62 | -3.20 | 4.53 | -1.33±3.33 | 0.175 | 0.40 | |||||||||||
| Lactate | 1.29 | 1.69 | 0.39±0.87 | 0.114 | 0.45 | 1.17 | 1.65 | 0.48±0.09 | 0.076 | 0.54 | |||||||||||
| Cl | 105.21 | 107.57 | 2.36±2.84 | 0.008 | 0.83 | 106.31 | 107.77 | 1.46±3.73 | 0.183 | 0.39 | |||||||||||
| Na | 136.36 | 138.07 | 1.71±2.13 | 0.010 | 0.81 | 137.85 | 138.54 | 0.69±3.25 | 0.457 | 0.21 | |||||||||||
| Glucose | 5.34 | 6.59 | 1.25±1.96 | 0.033 | 0.59 | 5.45 | 6.78 | 1.32±1.36 | 0.040 | 0.97 |
Table 3: Changes in pH, Base Excess (BE), lactate, Chloride (Cl), Sodium (Na) and glucose from start of surgery to end of surgery
Table 3: Changes in pH, Base Excess (BE), lactate, Chloride (Cl), Sodium (Na) and glucose from start of surgery to end of surgery. d=effect size: less than 0.2 small, 0.5 moderate, more than 0.8 large Both groups were equivalent for the amount of crystalloids and blood transfused during surgery. The total volume per weight per (ml/kg/hr) administered in RL and Sterofundin was (36.9±17.5 vs 37.1±20.5, p=0.974) and the amount blood transfused per weight (ml/kg) in RL and Sterofundin groups was (48.6±77.6 vs 34.6±85.1, P=0.66). Cardiovascular stability was maintained in both groups. None of the children experienced hypoglycemia (10mmol/l) in this study (Figure 2).

Discussion
At a glance, the alterations in blood variables are in favour of Sterofundin administration that resulted in lesser changes in pH, BE (less negative), Cl and Na at the end of surgery. It is also notable that BE, Cl and Na did not reach statistical significance in Sterofundin whereas the three parameters were significantly altered in Ringer’s Lactate. Lactate was not significantly altered in either group. In our study, we found that Ringer’s Lactate had a mean difference in pH of 0.07 compared to 0.05 in Sterofundin from the start of surgery to the end of surgery, both of which were statistically significant. The physiological pH of a normal human arterial blood is strictly maintained at 7.40. Hence, a slight reduction of more than 0.05 units from the normal pH will results in acidosis [9]. A research on hypochloraemic acidosis has revealed that even small changes in pH can have a negative impact on organ systems [10]. In addition, fluid requirements during other forms of major surgery may far exceed the amount administered in this current study. Thus, small but significant differences concerning acid base stability of applied crystalloids may gain importance eventually if increasing amounts of fluid are administered or if duration of surgery lasts longer. Ringer’s Lactate showed a significant change in BE from beginning to end of surgery. The mean change in BE in the Ringer’s Lactate group was 1.66 compared to 1.33 in the Sterofundin group. The changes are small, but are statistically relevant. Therefore, it is some concern that at the end of long duration of surgery (more than 4 hours), the base excess in Ringer’s lactate may became more negative. As a result, children who are administered Ringer’s Lactate for long surgeries are at risk to develop some degree of metabolic derangement intraoperative. Hence, these children will require closer monitoring of their acid-base balance intraoperatively. From the result of our study, it may be postulated that Sterofundin even if administered in large volumes may preserve optimum acid-base characteristics. In this study, we did not compare Sterofundin with infusion of normal saline, as it was shown by several studies that large volumes of normal saline will increase Cl and decrease BE in a dose- dependent manner leading to acidosis [8, 10]. RL group demonstrated a small but statistically significant change in serum Na and Cl levels in contrast to the Sterofundin group. However the changes were within the physiological range and direct adverse clinical impact was unlikely to arise. There is an inverse linear relationship between Cl level and BE. A study had noted that Hyperchloremic acidosis was associated with the amount of Cl received during intravenous fluid resuscitation with the base excess changing, on average, by -0.4 mmol/L of BE for each mmol/kg of Cl administered [11]. In our study, the change in Cl is small. However in a large study comparing normal saline and Sterofundin, it was shown that regardless of the type crystalloid infused in large amount (> 46 ml/kg) in patient less than 10 months, the relative risk of developing Hyperchloremic is significantly high [8]. A concern regarding balanced solutions such as Ringer’s Lactate and Sterofundin that contain bicarbonate precursors (lactate or acetate), is that there is a possibility for these solutions to produce metabolic alkalosis after larger volumes are administered [12]. Metabolic alkalosis has been associated with worse outcomes in the critically ill [13]. In our study, both sets of analysis showed that neither groups had metabolic alkalosis. The hemodynamics profile remained stable throughout and was comparable in both groups. Although acetate- containing solutions have been reported to cause severe hemodynamic instability due to increased nitric oxide synthesis and enhanced arrhythmias, this was only noted in patients who were undergoing haemodialysis [14]. In our study, we did not infuse any glucose solution intravenously. However, both groups of patient did not experience any hypoglycemia (10mmol/l). In contrast, It was shown by other studies that infusion of 1% dextrose with Sterofundin to be beneficial in preventing hypoglycemia and ketoacidosis in neonates and children less than 4 years old [15, 16]. This probably because the children in our study were older children and the anesthesia and surgical stress had led to reduced intraoperative glucose requirements. There are a few limitations in this study. Firstly, data was only collected intraoperative and one hour postoperatively and patients were not followed up until the end of their hospital stay. Therefore if there is any change in the electrolyte and acid base status at postoperative day one due to the different type of study fluid administered, it will be missed. This study also excluded patients with renal and liver disease who would benefit from Sterofundin as the acetate and maleate in Sterofundin can be metabolized in multiple sites in the body and not just the liver, as is the case with lactate in Ringer’s Lactate. The sample size of this study is only powered for changes in plasma pH. Therefore, larger sample size will be needed for other secondary observations.
Conclusion
Our study shows the intraoperative use of Sterofundin is comparable or even better than Ringer’s Lactate in terms of preservation of acid-base and electrolyte balance, avoidance of hypo/hyperglycaemia and cardiovascular stability in ASA I-III children undergoing moderate to major pediatric surgery. However, given the small number of patients enrolled, larger studies are required to clarify the better acid-base status of patients administered with Sterofundin. While a waiting for future directions from evidence-based studies, Sterofundin may be preferential and beneficial to Ringer’s Lactate as a crystalloid in Perioperative fluid management under most circumstances.
Competing Interests
No external funding or conflicts of interest exist. The study was supported by Institutional Grant: RG312/11HTM.
Author’s Contributions
IIS is the corresponding author, contributor to conception and design, acquisition of data, analysis and interpretation of data; contributed in drafting the article and revising it. PPA contributed to conception and design, and acquisition of data; contributed in drafting the article and revising it. AC contributed to conception and design, and acquisition of data; contributed in drafting the article and revising it. KC contributed to conception and design, data acquisition, analysis and interpretation of data; contributed in drafting the article and revising it. LC contributed to conception and design, and acquisition of data; contributed in drafting the article and revising it. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to thank our anaesthetic colleagues at the Department of Anaesthesia, University of Malaya Medical Centre and nursing staff for their help in the trial.
References
-
Murat I, Dubois MC (2008) Perioperative fluid therapy in pediatrics. Pediatric anesthesia 18(5): 363- 370.
-
Moritz ML, Ayus JC (2005) Preventing neurological complications from dysnatremias in children. Pediatric Nephrology 20(12): 1687-1700.
-
Waters JH, Gottlieb A, Schoenwald P, Popovich MJ, Sprung J, et al. (2001) Normal saline versus lactated Ringer’s solution for Intraoperative fluid management in patients undergoing abdominal aortic aneurysm repair: An outcome study. Anesthesia & Analgesia 93(4): 817-822.
-
Burdett E, Roche AM, Mythen MG (2003) Hyperchloremic acidosis: pathophysiology and clinical impact. Transfusion alternatives in transfusion medicine 5(4): 424-430.
-
Prough DS, Bidani A (1999) Hyperchloremic metabolic acidosis is a predictable consequence of Intraoperative infusion of 0.9% saline. Anesthesiology 90(5): 1247-1249.
-
Galas F, Hajjar L, Simoes C, Vieira S, Kalil Filho R, et al. (2009) Effects of Ringer's lactate or Ringerfundin resuscitation on the acid–base status and serum electrolytes in septic oncologic patients. Critical Care 13(Suppl 1): P447.
-
Guidet B, Soni N, Della Rocca G, Kozek S, Vallet B, et al. (2010) A balanced view of balanced solutions. Crit Care 14(5): 325.
-
Disma N, Mameli L, Pistorio A, Davidson A, Barabino P, et al. (2014) A novel balanced isotonic sodium solution vs normal saline during major surgery in children up to 36 months: a multicenter RCT. Pediatric Anesthesia 24(9): 980-986.
-
Aoi W, Marunaka Y (2014) Importance of pH homeostasis in metabolic health and diseases: Crucial role of membrane proton transport. BioMed research international 0-8.
-
Lira A, Pinsky MR (2014) Choices in fluid type and volume during resuscitation: impact on patient outcomes. Annals of Intensive Care 4: 38.
-
O'Dell E, Tibby SM, Durward A, Murdoch IA (2007) Hyperchloremia is the dominant cause of metabolic acidosis in the post resuscitation phase of pediatric meningococcal sepsis. Crit Care Med 35(10): 2390- 2394.
-
Morris C, Boyd A, Reynolds N (2009) Should we really be more ‘balanced’ in our fluid prescribing? Anaesthesia 64(7): 703-775.
-
Tripathy S (2009) Extreme metabolic alkalosis in intensive care. Indian journal of critical care medicine: peer-reviewed, official publication of Indian Society of Critical Care Medicine 13(4): 217- 220.
-
Hofmann-Kiefer KF, Chappell D, Kammerer T, Jacob M, Paptistella M, et al. (2012) Influence of an acetate- and a lactate-based balanced infusion solution on acid base physiology and hemodynamics: an observational pilot study. European journal of medical research 17(1): 1- 8.
-
Sumpelmann R, Mader T, Eich C, Witt L, Osthaus WA (2010) A novel isotonic-balanced electrolyte solution with 1% glucose for intraoperative fluid therapy in children: results of a prospective multicentre observational post-authorization safety study (PASS). Pediatric Anesth 20(11): 977–981.
-
Sumpelmann R, Mader T, Dennhardt N, Witt L, Eich C, et al. (2011) A novel isotonic balanced electrolyte solution with 1% glucose for intraoperative fluid therapy in neonates: results of a prospective multicentre observational postauthorisation safety study (PASS). Paediatr Anaesth. 21(11): 1114-1118.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index