Delirium in the Oncology Patient: Case Report
Delirium is an alteration of attention or consciousness accompanied by a change in basic cognition, which manifests as a decreased ability to direct, focus, maintain and shift attention. In the postoperative period it can be a factor that reduces the quality of life and perioperative outcome in cancer patients. It has been associated with increased in-hospital stay and morbidity and mortality. The following is the case of a 61-year-old patient who underwent an exploratory laparotomy and presented with hypoactive delirium with transition to hyperactive delirium in the first postoperative hours. Postoperative delirium occurs in 10-60% of patients, and its incidence is higher in older patients. It may present as a hyperactive, hypoactive state or with a mixed component, a key feature of this etiology being its fluctuating behavior between these states. Primary prevention of postoperative delirium requires a multimodal approach, the first-line measures being non-pharmacological interventions.
Introduction
Preoperative anxiety and postoperative delirium are factors that reduce quality of life and worsen surgical outcomes in cancer patients [1]. Geriatric syndromes are the most frequently identified clinical conditions in frail older adults [2]. Postoperative delirium is a challenge for sustainability, mainly in societies with a larger group of elderly people, since it causes an increase in economic and social costs [1]. Previous studies have shown that older adult patients with oncologic pathologies present a higher prevalence of geriatric syndromes [2]. In patients with risk factors for postoperative delirium who undergo highly complex surgery, the incidence reaches 50%; however, up to 40% of the cases can be prevented. It is estimated that more than half of the patients who undergo oncological surgery can be classified as frail [3]. Evidence suggests that cancer treatments may cause cognitive impairment, which is reported subjectively or can be measured objectively by neuropsychological tests [4].
Delirium is considered an alteration of attention or consciousness accompanied by a change in basic cognition, which manifests as a decreased ability to direct, focus, maintain and shift attention, due to the individual being easily distracted by irrelevant stimuli [5, 6]. The development of such events is associated with significantly worse clinical outcomes [3]. Delirium in intensive care units (ICU) has an incidence ranging from 5% to 92%. In oncology patients, the incidence of delirium is also high; reaching up to 80% in the most advanced stages of the disease, and it has also been related to worse analgesic control and decreased survival [5]. Patients and families should be warned that despite the low risk of delirium associated with chemotherapy, it can have significant clinical repercussions [6]. Delirium can persist for hours or days, and present in a fluctuating manner during the course of the day. Postoperative delirium occurs in 10-60% of patients, and its incidence is higher in older patients [7].
Pathophysiology
There are several theories regarding the pathophysiology of postoperative delirium, based on findings from animal models; however, evidence from human studies is currently limited [8].
Neuroinflammation
One of the possible pathophysiological mechanisms of postoperative delirium is neuroinflammation. Systemic proinflammatory mediators are significantly elevated following a surgical event and remain elevated during the postoperative period. Postoperative elevation of peripheral C-reactive protein (CRP) and interleukin-6 (IL- 6) concentrations have been reported to be risk factors associated with the presence of postoperative delirium [8].
Neurotransmitters
Another possible pathophysiological mechanism of postoperative delirium is the alteration of neurotransmitters. Acetylcholine is thought to be involved in neuroplasticity, and is present in several neuronal pathways responsible for attention and memory processes [8]. A recent observational study, performed in patients undergoing cardiac surgery concluded that patients who presented postoperative delirium had lower acetylcholinesterase levels, both before the operation and up to 2 days after the operation, and that this same reduced activity is an independent risk factor for the development of postoperative delirium, as well as drugs with anticholinergic action at the central level (such as amitriptyline) [9].
Subclinical Cerebral Vascular Events
Diseases that increase the risk of cerebral vascular events, such as hypertension, atrial fibrillation, and previous stroke, have been reported to be risk factors for the development of postoperative delirium. Although the risk of postoperative stroke with overt clinical repercussions is rare, radiological evidence of cerebral ischemia can be documented in 7-10% of elderly surgical patients, and this has been associated with more than doubling the risk of postoperative delirium [8].
Cognitive Complications
Clinically significant neurocognitive complications affecting older patients include postoperative delirium (POD) and postoperative cognitive dysfunction (POCD). Delirium, defined as an acute change in attention and cognition, is the most common postoperative complication in older patients, affecting up to half of them after surgery [3]. The American Cancer Society defines chemotherapy-related cognitive impairment (CRCI) as increased forgetfulness, difficulty concentrating and remembering details, difficulty multitasking and finding words, and taking longer to complete tasks. To date, most research on CRCI has been conducted in women with breast cancer, who represent approximately 23% (3.6 million) of the 15.5 million cancer survivors in the United States alone [10]. The development of delirium in older patients is likely to be multifactorial in origin, with predisposing risk factors. Predisposing factors include advanced age, frailty, disability, alcohol or drug abuse, multiple comorbidities, living in a geriatric care facility, and severity of illness, and several biological mechanisms have been suggested to play a role in the development of CRCI, including blood-brain barrier damage, release of neurotoxic cytokines, changes in hormone levels, DNA damage, oxidative stress, reduced neuroplasticity, the presence of altered levels of growth factors, and altered hippocampal neurogenesis [3, 10]. Postoperative delirium is a frequent clinical condition in elderly patients undergoing surgery, varying from 28 to 50% [11].
The most widely used diagnostic tool to identify delirium in older adults is the Confusion Assessment Method (CAM), which has a sensitivity of 94% and a specificity of 89% in high quality studies including more than 1000 patients, The CAM-ICU (CAM modified for intensive care patients) is a modification of the CAM to facilitate its application by medical and nursing staff in elderly patients admitted to the Intensive Care Unit, which assesses the presence of four criteria: (I) Acute fluctuating mental status, (II) Inattention, (III) Disorganized thinking, and (IV) Altered level of consciousness. The presence of a positive CAM-ICU necessarily requires the presence of criteria I and II, together with criteria III or IV, thus making it possible to establish the diagnosis of delirium [3].
Predisposing factors can be classified by organs and systems: • Neuropsychological factors: cognitive impairment, dementia, previous stroke, depression, history of delirium, and limited cognitive reserve.
- Cardiovascular factors: hypertension, heart failure and ischemic heart disease.
- Respiratory factors: chronic obstructive pulmonary disease, obstructive sleep apnea and active smoking.
- Gastrointestinal factors: diabetes mellitus, malnutrition, hypoalbuminemia and overweight or obesity [3].
Cancer and Frailty
Frailty is defined as a clinical state characterized by multisystemic deterioration, which is associated with the loss of physiological reserves [3]. Traditionally, clinical trials in oncology have focused on validating specific clinical criteria related to oncologic pathology, from diagnostic tools, overall survival rates, disease-free survival time, as well as treatment response rates; cognitive function is often not considered as an endpoint in interventional trials evaluating response to chemotherapy in most cancer subtypes, despite the fact that patients value cognition as an important outcome [4]. When frail individuals are exposed to a stressor such as chemotherapy treatment or undergoing cancer surgery, they are at increased risk of disability or even increased mortality. In the general population, frailty affects approximately 10% of people over 65 years of age and 25-50% of those over 85 years of age [3]. Since the 1980s, the presence of cognitive impairment associated with chemotherapy has been reported in patients with oncologic pathology of the peripheral nervous system, a phenomenon commonly known as “chemo brain” or “chemotherapy fog”, a phenomenon little known and, until relatively recently, ignored [10, 11, 12, 13]. It is likely that its etiology is multifactorial in origin through interactive mechanisms that induce direct or indirect effects on the central nervous system (CNS), affecting the cognitive capacity of patients. Genetic predisposition seems to play an important role in determining and possibly predicting long- term cognitive impairment in cancer patients. Historically, it has been reported that cancer survivors with a positive mutation in the e4 allele of apolipoprotein E (APOEe4) have a significantly increased risk of developing a cognitive deficit compared to those with other APOE allele mutations [12]. Patients with oncologic pathology other than that of the central nervous system (CNS) often present with cognitive symptoms, also called “cancer-related cognitive impairment” (CRCI), which occur mainly after the first cycle of chemotherapy, either as impaired short-term and working memory, impaired attention, impaired executive functions and/or decreased processing speed. Fifty percent of breast cancer patients have cognitive impairment following chemotherapy; however, only 15-25% have objective cognitive impairment [14].
The pathophysiology linking cancer and frailty is likely to be multifactorial in origin, including metabolic and immune dysfunction, polypharmacy related to cancer treatment and direct inflammatory effect caused by the tumor, as well as functional changes. Patients with frailty have a higher risk of presenting intolerance to chemotherapy, postoperative complications and higher mortality [3, 7].
Recently it has been described that colon and rectal surgery is associated with a higher incidence of postoperative delirium, and with worse clinical outcomes (increased length of in-hospital stay and higher mortality rates). In particular, it has been found that procedures performed with laparoscopic techniques have a significantly lower incidence of postoperative delirium [11].
Types of Delirium
Depending on the level of activity, delirium may present with a hyperactive, hypoactive or mixed component, a fundamental characteristic of this etiology being its fluctuating behavior between these states. Hyperactive delirium is characterized by the presence of agitation and increased alertness, while hypoactive delirium is characterized by lethargy and decreased motor activity. Hypoactive delirium is more common than hyperactive delirium, but is often overlooked. Previous studies reported that hypoactive delirium was associated with higher mortality than hyperactive delirium, but nurses who cared for patients with hyperactive delirium experienced greater subjective burden compared with those who cared for patients with hypoactive delirium. Although antipsychotics are widely used for the treatment of delirium, current evidence does not support their routine use because of adverse effects, such as oversedation, somnolence, and extrapyramidal symptoms [15]. Postoperative delirium in the elderly is an acute disorder of attention and cognition that is common, fatal, costly, and underrecognized. Consequently, delirium is now included in the safety agendas of older patients and is increasingly used as an indicator of the quality of medical care for the elderly [16]. Postoperative delirium is defined as an acute, fluctuating disorder of consciousness and inattention after surgery [17].
Clinical Case
This case is about a 61-year-old female patient who underwent an exploratory laparotomy, resulting in cytoreduction and an ileostomy with a diagnosis of endometrial adenocarcinoma, dysphagia to solids for 6 months, with a history of routine endometrial surgery, chemotherapy (20 sessions), total abdominal hysterectomy plus adhesiolysis, lymph node resection, port catheter placement, and diagnostic laparoscopy plus cytoreduction. On physical examination we observed a patient of apparent age older than chronological age located in space and time. Under mixed interrogation, she has family support, requires support for activities of daily living. We observed infantilism during the interview. Height: 1.47mts weight: 65kg, short neck, short chin, and partial edentulism, normal vesicular breath sounds RR: 17rpm, SpO2:90%, rhythmic heart sounds of good intensity and tone HR: 56 bpm, BP: 130/70mmhg.The abdomen had a thick adipose panniculus. An abdominal CT scan showed reactive lymph nodes with preserved shape and fatty hilum, located in the mediastinum, mesentery, and right external iliac chain. As additional findings, a hiatal hernia, a right renal cyst, colonic diverticulosis, and degenerative osteoarthropathy were also noted. Laboratory tests showed: hemoglobin 11. 1mg/dl, hematocrit 31.6, leukocytes 7.7, platelets 154, glucose 224, creatinine 0.76, proteins 5.6, albumin 3.
It was decided to perform balanced general anesthesia, under noninvasive monitoring. Upon admission to the operating room her vitals were: HR: 45 bpm, RR: 16 rpm, BP: 120/60 mmhg, SpO2: 90%. She received preoxygenation with tidal volume technique for 5 minutes. A fractional dose of butylhioscine 20mg was administered without increasing the HR. We proceded to administer an intravenous induction with fentanyl 150mcg, propofol 100mg, lidocaine 40mg, rocuronium 40mg. A #7 endotracheal tube was placed at the first attempt, as the first surgical time, high endoscopy was performed with distal esophageal dilatation without incident. Prior to the exploratory laparotomy, she presented sinus bradycardia 35 bpm with BP 90/50 mmhg. Atropine 1mg was administered without response. A second dose of atropine 1mg was administered, achieving a heart rate of 68 bpm BP:110/70 mmhg. Anesthetic maintenance under volume controlled mechanical ventilation TV: 380ml, RR:12 rpm, ETCO2: 28-34 mmhg, sevoflurane: 1-1.5 vol% BIS 40- 60% with predominance of alpha and beta waves. During the trans anesthetic period, she was hemodynamically stable with no need for vasopressor support. Fluid balance was: input: 1200ml (packed RBC: 300ml: fresh frozen plasma: 200ml); output: 1500ml (uresis: 1.5 ml/kg/hr, bleeding: 400ml); total balance: -300ml. Postoperative analgesic management was performed with abdominal TAP block as well as rectus abdominis fascia. Emergence was performed by pharmacological lysis with suggamadex, under safe parameters with airway protective reflexes present, and spontaneous ventilation. Glasgow 14, Aldrete: 9/10, Ramsay: 2. During her stay in postanesthesia care she presented Glasgow:12, Ramsay: 5. It was decided to administer naloxone 0.4mg IV with adequate response. The optic nerve sheath was traced by ultrasound. A diameter of 0.4mm was measured on 3 occasions, ruling out an increase in intracranial pressure. She was referred to the neurology team where a diagnosis of hypoactive delirium was made in the first postoperative hours, improving her reactivity with the passage of time. Later she presented psychomotor agitation. Haloperidol 2mg and olanzapine 25 mg were administered without response.
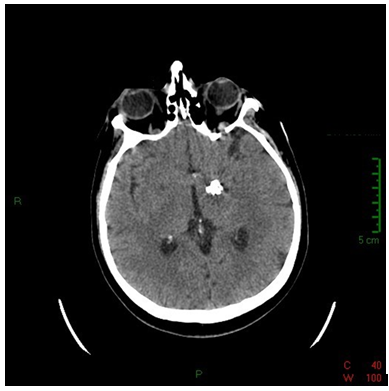
Dexmedetomidine infusion was started at 20mcg/hr without improvement. At the time of evaluation by Neurology, the neurological examination reported: pupils 6mm, dilated, non-reactive, mobilization of extremities to painful stimulus. A cranial computed tomography was performed where data of ischemia or acute hemorrhage were ruled out. A granulomatous lesion with calcium density in the region of the posterior arm of the internal capsule and 2 calcified lesions attached to the middle cerebral artery, suggestive of a chronic process, were reported (Figure 1).
She was admitted to the intensive care unit for close monitoring. During the transfer she presented a sinus bradycardia event of 25 bpm associated with arterial hypotension. She responded to the administration of 1 mg of Atropine. During her stay in the ICU she continued to be drowsy, unresponsive to verbal stimuli, withdrawing limbs to painful stimuli, with mydriatic, hyporeflectic pupils. A transthoracic echocardiogram was performed and reported: LVEF 60%, E/e’ ratio of 9, E/A ratio of 0.9, left atrial indexed volume of 27ml/m2, right ventricle with fractional area change of 41%, TAPSE 30mm and estimated PASP of 32 mmhg. During her stay in ICU, drugs were gradually withdrawn, showing improvement after 2 days. She was discharged neurologically intact, with resolution of delirium. She continued management as an outpatient.
Discussion
In view of what has been presented, we must understand that there are different ways to avoid the presence of delirium in our patients by having timely interventions for the comprehensive care of the oncologic patient, the interventions that most of medical doctors brings are divide in preoperative, intraoperative and postoperative.
Preoperative Interventions
Strategies used for the prevention of postoperative delirium include avoiding perioperative polypharmacy, avoiding prolonged fluid fasting (> 6 h) although 2 h of fluid fasting is recommended to allow voiding, patients often fast for much longer in practice [18, 19]. Comprehensive geriatric assessment (CGA) is a useful multidisciplinary approach to systematically assess and address the often complex care needs of older patients [8]. Several observational studies have found that poor preoperative analgesic control is associated with a 1.5- to 3-fold increased risk of postoperative delirium [15].
Intraoperative Interventions
Several studies have shown that the degree of anesthetic depth, especially prolonged periods of suppression rate, is an independent risk factor for postoperative delirium, further increasing its incidence when associated with previous risk factors of the patient, or factors inherent to the medical procedures [20].
Use of Opioid-Sparing Multimodal Analgesia
The most frequent complication following a surgical procedure is the presence of pain. A directly proportional relationship has been found in several observational studies between a higher postoperative pain score and the incidence of delirium [8]. NSAIDs and acetaminophen are commonly used as part of multimodal analgesia after surgery; in addition, it has been suggested that these drugs may prevent postoperative delirium by directly alleviating neuroinflammation [21]. It is known that surgical trauma can result in both an acute stress response and systemic inflammation [17].
Dexmedetomidine
Dexmedetomidine is a highly selective α2-adrenergic receptor agonist; initially licensed for sedation management in intensive care units, recent studies have demonstrated its neuroprotective utility by decreasing the incidence of delirium. In animal models, administration of dexmedetomidine reduced the expression of inflammatory mediators, microglial activation and neuroapoptosis [22].
Intraoperative Care
There is great controversy regarding the behavior of inhalational anesthetics compared to total intravenous anesthesia in relation to the incidence of delirium, because they induce hypnosis through different molecular targets, suggesting that inhalational anesthesia may exacerbate neuroinflammation, however, this being CAM-dependent [8]. Heat loss in patients undergoing general anesthesia is a common phenomenon that should be monitored and anticipated in any surgical procedure, as it is associated with coagulation factor dysfunction, as well as deleterious cardiovascular and immunologic changes [8]. Subclinical cerebral vascular events have been implicated in the development of postoperative delirium; any intraoperative hemodynamic fluctuation may result in transient cerebral hypoperfusion, especially in watershed areas [23]. Recently, a retrospective multicenter cohort study demonstrated the association of prolonged arterial hypotension during the transanesthetic period (defined by a MAP <55 mmHg) with a higher probability of developing postoperative delirium in patients undergoing noncardiac surgery [24]. Fluid management in the perioperative period guided by objective hemodynamic parameter goals to optimize circulating volume and maintain an adequate preload, helps to reduce fluid overload and thus reduce the risk of perioperative complications, being useful to reduce the risk of delirium in geriatric patients [24].
Postoperative Interventions
Non-Pharmacological Prevention of Delirium
Primary prevention of postoperative delirium requires a multimodal approach, with the first-line measures being nonpharmacologic interventions. Reorientation is a strategy to help patients become familiar with the environment and people [8]. Melatonin is a hormone involved in sleep regulation, and has shown utility as a pharmacological measure to regulate the circadian cycle. It was recently reported in a meta-analysis that perioperative administration of melatonin is associated with a reduction of up to 40% in the risk of developing postoperative delirium [25].
Dexamethasone
Dexamethasone is a synthetic corticosteroid frequently used (and included in guidelines) for the prevention of postoperative nausea and vomiting. Another use of corticosteroids is in the treatment of neuroinflammatory diseases [26].
Antipsychotics
These are drugs with dopamine antagonist action, which have varying degrees of affinity for muscarinic, serotonergic and adrenergic receptors [8]. It has been reported in the literature an association of antipsychotic drugs with an increased risk of anesthetic oversedation being this dose dependent, as well as with the development of extrapyramidal symptoms and long QT syndrome when used for the management of postoperative delirium, which in turn can lead to increased mortality in geriatric patients and in patients with dementia [1].
Conclusion
The oncology patients frequently associate a greater presence of comorbidities and usually present a greater degree of deterioration of the baseline physiological state, coming to present a high incidence of frailty syndrome during the different stages of their disease. Additionally, the presence of polypharmacy (and especially chemotherapy) generates a high risk for the presence of delirium in oncological patients, which is exponentially multiplied when they are subjected to a surgical procedure due to all that a hospital stay entails. Therefore, it is of utmost importance to carry out a multidisciplinary approach and a preventive strategy that includes the adequate choice of the type of surgery, reduction of surgical times, adequate perioperative fluid management, implementation of blood saving techniques, adequate transanesthetic thermal control, implementation of multimodal analgesia, systematic use of neuromonitoring to monitor the anesthetic depth and the use of anti-inflammatory drugs, among other factors, resulting in a lower incidence of postoperative delirium. In addition to preventive measures, having a high index of suspicion will help early detection in order to implement an adequate and timely management, thus reducing morbidity and mortality derived from this entity.
References
-
Wada S, Sadahiro R, Matsuoka YJ, Uchitomi Y, Yamaguchi T, et al. (2021) Yokukansan for Treatment of Preoperative Anxiety and Prevention of Postoperative Delirium in Cancer Patients Undergoing Highly Invasive Surgery. J-SUPPORT 1605 (ProD Study): A Randomized, Double- Blind, Placebo Controlled Trial. Journal of Pain and Symptom Management 61(1): 71-80.
-
Magnuson A, Sattar S, Nightingale G, Saracino R, Skonecki E, et al. (2019) A Practical Guide to Geriatric Syndromes in Older Adults With Cancer: A Focus on Falls, Cognition, Polypharmacy, and Depression. American Society of Clinical Oncology 39: 96-109.
-
Daksla N, Nguyen V, Jin Z, Bergese SD (2022) Brain Prehabilitation for Oncologic Surgery. Current Oncology Reports 24(11): 1513-1520.
-
Loh KP, Janelsins MC, Mohile SG, Holmes HM, Hsu T, et al. (2016) Chemotherapy-related cognitive impairment in older patients with cancer. Journal of geriatric oncology 7(4): 270-280.
-
Gouveia BR, Jomar RT, Valente TCO (2019) Delirium in cancer patients admitted to the intensive care unit: a retrospective study. Rev Bras Ter Intensiva 31(4): 536- 540.
-
Jung P, Puts M, Frankel N, Syed AT, Alam Z, et al. (2021) Delirium incidence, risk factors, and treatments in older adults receiving chemotherapy: A systematic review and meta-analysis. Journal of Geriatric Oncology 12(3): 352- 360.
-
Cicerchia M, Ceci M, Locatelli C, Gianni W, Repetto L, et al. (2010) Geriatric syndromes in peri-operative elderly cancer patients. Surgical Oncology 19(3): 131-139.
-
Jin Z, Hu J, Ma D (2020) Postoperative delirium: perioperative assessment, risk reduction, and management. British Journal of Anaesthesia 125(4): 492-504.
-
Adam EH, Haas V, Lindau S, Zacharowski K, Scheller B, et al. (2020) Cholinesterase alterations in delirium after cardiosurgery: a German monocentric prospective study.. BMJ Open 10(1): e031212.
-
Vega JN, Dumas J, Newhouse PA (2017) Cognitive Effects of Chemotherapy and Cancer-Related Treatments in Older Adults. Am J Geriatr Psychiatry 25(12): 1415- 1426.
-
Monacelli F, Signori A, Prefumo M, Giannotti C, Nencioni A, et al. (2018) Delirium, Frailty, and Fast-Track Surgery in Oncogeriatrics: Is There a Link. Dement Geriatr Cogn Disord 8(1): 33-41.
-
Argyriou AA, Assimakopoulos K, Iconomou G, Giannakopoulou F, Kalofonos HP, et al. (2011) Either Called ‘‘Chemobrain’’ or ‘‘Chemofog’’ the Long-Term Chemotherapy-Induced Cognitive Decline in Cancer Survivors is Real. Journal of pain and symptom management 41(1): 126-139.
-
Dias-Carvalho A, Ferreira M, Ferreira R, Bastos ML, Sá SI, et al. (2022) Four decades of chemotherapy induced cognitive dysfunction: comprehensive review of clinical, animal and in vitro studies, and insights of key initiating events. Archives of Toxicology 96(1): 11-78.
-
Lange M, Joly F, Vardy J, Ahles T, Dubois M, et al. (2019) Cancer-related cognitive impairment: an update on state of the art, detection, and management strategies in cancer survivors. Annals of Oncology 30(12): 1925- 1940.
-
Abe H, Sumitani M, Matsui H, Inoue R, Konishi M, et al. (2022) Gabapentinoid Use Is Associated With Reduced Occurrence of Hyperactive Delirium in Older Cancer Patients Undergoing Chemotherapy: A Nationwide Retrospective Cohort Study in Japan. Anesthesia- Analgesia 135(2): 362-369.
-
Huyan T, Hu X, Peng H, Zhu Z, Li Q, et al. (2019) Perioperative dexmedetomidine reduces delirium in elderly patients after lung cancer surgery. Psychiatria Danubina 31(1): 95-101.
-
Ishibashi H, Wakejima R, Asakawa A, Sugita Y, Ishikawa Y, et al. (2022) Postoperative Delirium in Lung Cancer Anatomical Resection-Analysis of Risk Factors and Prognosis. World J Surg 46(5): 1196-1206.
-
Ahmed S, Leurent B, Sampson EL (2014) Risk factors for incident delirium among older people in acute hospital medical units: sistematic review and meta-analysis. Age Ageing 43(3): 326-333.
-
Radtke FM, Franck M, MacGuill M, Seeling M, Lütz A, et al. (2010) Duration of fluid fasting and choice of analgesic are modifiable factors for early postoperative delirium. Eur J Anaesthesiol 27(5): 411-416.
-
Soehle M, Dittmann A, Ellerkmann RK, Baumgarten G, Putensen C, et al. (2015) Intraoperative burst suppression is associated with postoperative delirium following cardiac surgery: a prospective, observational study. BMC Anesthesiol 15: 61.
-
Carty ML, Wixey JA, Reinebrant HE, Gobe G, Colditz PB, et al. (2011) Ibuprofen inhibits neuroinflammation and attenuates white matter damage following hypoxia– ischemia in the immature rodent brain. Brain Res 1402: 9-19.
-
He H, Zhou Y, Zhou Y, Zhuang J, He X, et al. (2018) Dexmedetomidine mitigates microglia-mediated neuro inflammation through upregulation of programmed cell death protein 1 in a rat spinal cord injury model. J Neurotrauma 35(21): 2591-2603.
-
Maheshwari K, Ahuja S, Khanna AK, Mao G, Perez-Protto S, et al. (2020) Association between perioperative hypotension and delirium in postoperative critically ill patients: a retrospective cohort analysis. Anesth Analg 130(3): 636-643.
-
Langer T, Santini A, Zadek F, Chiodi M, Pugni P, et al. (2019) Intraoperative hypotension is not associated with postoperative cognitive dysfunction in elderly patients undergoing general anesthesia for surgery: results of a randomized controlled pilot trial. J Clin Anesth 52: 111- 118.
-
Campbell AM, Axon DR, Martin JR, Slack MK, Mollon L, et al. (2019) Melatonin for the prevention of postoperative delirium in older adults: a systematic review and metaanalysis. BMC Geriatr 19: 272.
-
Meneses G, Gevorkian G, Florentino A, Bautista MA, Espinosa A, et al. (2017) Intranasal delivery of dexamethasone efficiently controls LPS-induced murine neuroinflammation. Clin Exp Immunol 190(3): 304-314.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index