A Case of Penetrating Thoracic Injury- A Diagnostic Dilemma and Subsequent Management
Trauma is the leading cause of death worldwide. Mortality from thoracic trauma is second highest after head injury. Penetrating thoracic injury poses a challenge in predicting the extent of injury, structures involved and severity of intraoperative adverse events. Diagnostic imaging plays an important part in the evaluation of these patients. We will be doing the detailed discussion on above aspects in this article.
Introduction
A retained thoracic knife, in the form of either the knife blade and handle or the knife blade alone, following an assault is a relatively uncommon injury [1]. In 75% of these patients, penetrating pulmonary injuries are managed with tube thoracostomy alone. Of those who require operative intervention, 24% have been shown to require repair of pulmonary hilar or major parenchymal injuries. Pulmonary resections in this setting have been shown to carry a mortality rate of 30-60% [2].
Diagnostic imaging plays a key role in the management of patients after chest trauma and in decision making. The information generated by diagnostic imaging not only serves to tailor therapy to the individual needs of patients, but also contributes to determine prognosis and outcome [3].
We present a challenging case of penetrating thoracic knife injury, where there was dilemma in predicting the extent of injury due to in-conclusive imaging findings.
24 years old male patient was scheduled for a foreign body removal from right thorax. Patient was working in the field, when the blade of grinder, used for cutting of crops, suddenly broke and pierced his right thorax. Patient presented to emergency unit with tachypnoea and difficulty in breathing.
On examination, there was a stab entry wound in the right thorax, at anterior axillary line, measuring around two inches horizontally at 5th intercostal space. There was tenderness around the site on palpation with decrease air entry in right thorax. Tachycardia and tachypnoea were present and room air saturation was 92%. Oxygen supplementation with face mask was started immediately.
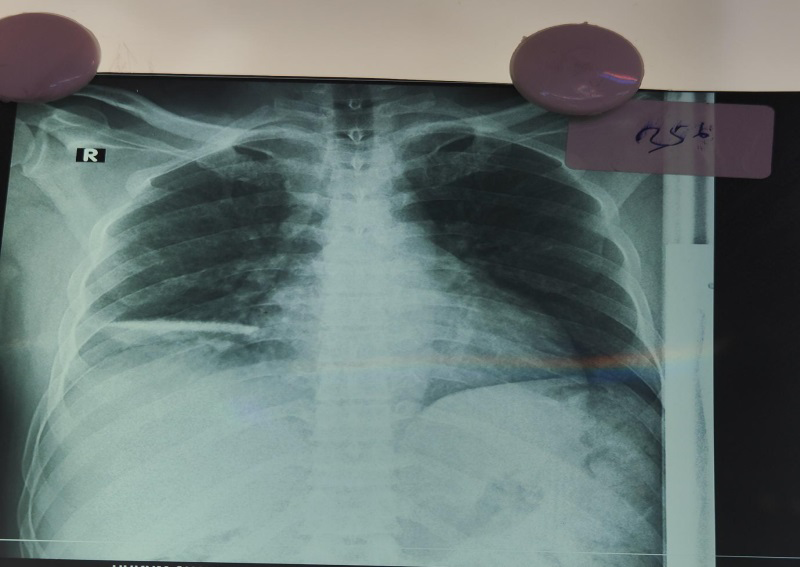
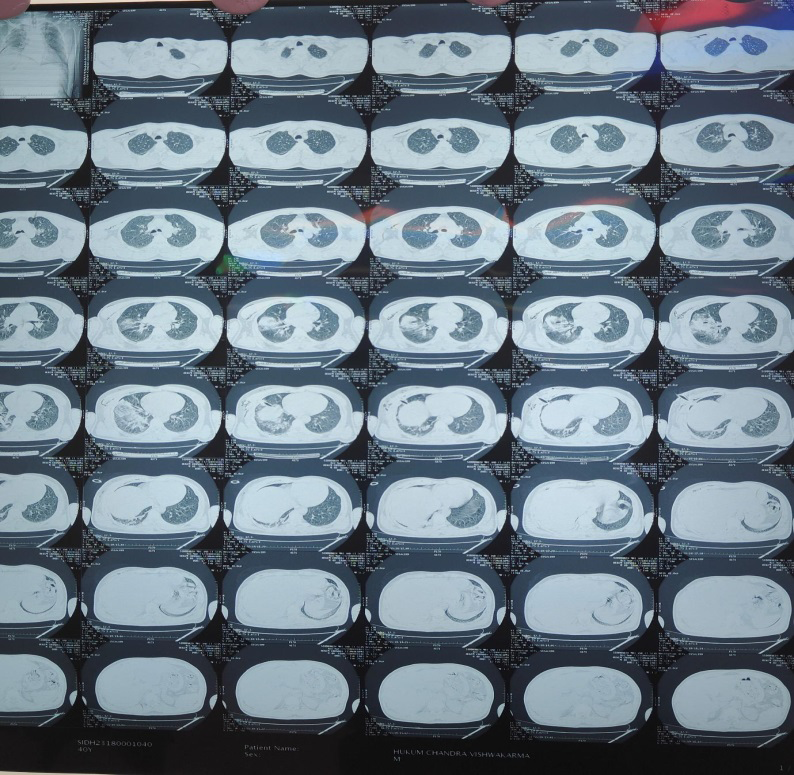
X-Ray chest showed the blade impacted in his right middle lobe (Figure 1). However, his Computed tomography (CT) image, except for the soft tissue opacity around the suspected area, did not show any blade in the thorax (Figure 2). Echo cardiography done in casualty revealed no tamponade. Routine blood investigations were normal.
Surgery for blade removal under general anaesthesia was scheduled. Patient was premedicated with injection pethidine and injection phenargan in the preoperative area one hour prior to the surgery. With premedication, initial tachypnoea of 28 breaths per minute got settled to 20 breaths per minute prior shifting the patient to Operation theatre. Oxygen supplementation using 6 lt/minute with a venturi mask was maintained until induction agents were initiated. A rapid sequence induction was planned to avoid further damage from positive pressure ventilation. Injection propofol, injection fentanyl, injection rocuronium were used for induction and airway was secured with a 37 Fr Right sided double lumen tube. Position of the tube was confirmed both with Auscultation and AMBUSCOPE. Ventilation was allowed only to the Left lung to avoid further damage to right lung. Pressure controlled ventilation was used restricting the peak pressure to 25mm Hg and Respiratory Rate was adjusted to maintain adequate minute ventilation. Patient was placed in the left lateral position for easy surgical access. Surgery proceeded smoothly, except in the final extraction of the foreign body, a massive bleed started as one the intercostal vessels, which was earlier tamponaded by the blade, started bleeding on the blade removal. The patient lost approximately 2 l of blood, before the vessel rent could be ligated securely. Blood pressure slumped to values less than 70mmHg and 500ml colloids (Voluven) was given and a decision to initiate Vasopressors was made. Infusion Dopamine was started at 3mcg/kg/hr which helped us in maintaining stable vitals till the end of surgery. ABG was sent showed reduced Hemoglobin (7.2 gm/dl) for which two PRBCs were transfused gradually. An Intercostal drain was inserted on the right side in the end. As the spontaneous efforts of patient were adequate, trail for extubation was done. Patient was observed for 30 minutes inside OT and shifted to post-operative ICU for further observation. In the ICU patient was monitored for two days and ICD was removed after discussing with the surgeon on POD2.
Discussion
Trauma is the leading cause of death worldwide [4, 5]. In majority (70%) of cases, this devastating injury to the chest is associated with multisystem injuries [5, 6]. Mortality is second highest after head injury. The German Trauma Registry, which included 873 chest trauma patients between 1993 and 2008, showed that 60% had an AIS (Abbreviated Injury Scale) score ≥3 (serious), expressing once again the potential severity of chest trauma [4]. Gunshot injuries and stab injuries constitute majority of penetrating chest injuries with incidence of 10% and 9.5%. Although severity and outcome changes accordingly with the extent of damage, involvement of heart, lungs and major thoracic vessels is often associated with high risk for mortality.
Radiological diagnosis is a central part of the initial clinical management phase and so has been incorporated in the procedural algorithms. A CT angiography (CTA) of the thorax should also be done if a vascular lesion is suspected, in particular in deceleration injuries, e.g., high-speed car crashes, or suspected aortic injury. The introduction of multislice CT (MSCT) is a major development [7]. Magnetic resonance imaging (MRI) has a limited role in the initial evaluation of the trauma patient, but may be of use for the evaluation of the spine and diaphragm [8].
However, in our case, the CT findings were inconclusive. X-ray chest was the only imaging tool available to predict the extent of injury, with its limitations.
Penetrating thoracic injury can be the most lethal of injuries. Penetrating abdominal injuries are not immediately life-threatening unless a major blood vessel is damaged [5].
Prediction of bleeding by mere position of knife is difficult, just as it was in our case. Bleeding from the wound is usually from the intercostal blood vessels, since they are part of systemic circulation, comparing to blood vessels from lungs which are the part of pulmonary circulation with lower pressure. Air embolism occurs in the setting of a fistulous connection between a bronchus and a pulmonary vein. With spontaneous respiration, the pressure differential favours a gradient from the vein to the bronchus resulting in hemoptysis in 22% of these patients. With positive pressure ventilation or with Valsalva-type respiration, the gradient is reversed and results in systemic air embolism [2].
Penetrating lung injuries may extend to cardiac injury, pulmonary lacerations and other vascular injuries. Although penetrating thoracic trauma is relatively common, retained knife in this setting is rare [1]. Other associated injuries include spinal cord injury, splenic and hepatic injury, brachial plexus injury (associated with fractures of ribs 1–3), injury of the subclavian artery and the development of Horner’s syndrome (interruption of sympathetic nerve supply to the eye) [5].
The choice of incision is determined by the clinical and imaging findings. Cardiac arrest secondary to cardiac tamponade can potentially occur in this specific setting of retained knife. Knife itself is often contaminated and can contain embedded clothing and other materials. Aggressive and early wound management is appropriate [1].
Those at increased risk of developing complications following major thoracic trauma have three or more rib fractures, are 65 years or older, used anticoagulant therapy pre-injury, have previously diagnosed chronic respiratory disease or cardiovascular disease, and/or have arterial oxygen saturation of less than 90% on admission. The body’s response to traumatic injury, blood loss and surgery is activation of a major acute inflammatory response. This contributes to muscle protein breakdown and wasting. Blood oxygen levels are low because of reduced erythropoietin production and phlebotomy procedures in the ICU setting, which further increase pro-inflammatory cell activity and insulin resistance. The systemic inflammatory response syndrome leads to the development of sepsis and multiple organ dysfunctions. These patients develop severe muscle wasting early and rapidly during their ICU stay.[5]
Physiotherapists play an important.
Conclusion
Thoracic injuries account for 20-25% of deaths due to trauma and contribute to 25-50% of remaining deaths [2].
Due to proximity with major vascular and neural structures, imaging plays a crucial role in the management of these cases. But not all images are helpful in evaluation of damage. Clinical assessment becomes important in these type of cases, which was reflected in our case.
References
-
Kong V, Cheung C, Buitendag J, Rajaretnam N, Varghese C, et al. (2022) Management of penetrating thoracic trauma with retained knife blade: 15-year experience from a major trauma centre in South Africa. Ann R Coll Surg Engl 104(4): 308-313.
-
Kuhajda I, Zarogoulidis K, Kougioutzi I, Huang H, Li Q, et al. (2014) Penetrating trauma. J Thorac Dis 6(4): 461- 465.
-
Lomoschitz FM, Eisenhuber E, Linnau KF, Peloschek P, Schoder M, et al. (2003) Imaging of chest trauma: radiological patterns of injury and diagnostic algorithms. Eur J Radiol 48(1): 61-70.
-
Ludwig C, Koryllos A (2017) Management of chest trauma. J Thorac Dis 9(3): 172-177.
-
Aswegen HV (2020) Physiotherapy management of patients with trunk trauma: A state-of-the-art review. S Afr J Physiother 76(1): 1406.
-
Goyal S, Panday BC (2020) Anesthetic Management of Thoracic Trauma. In: Sood J, et al. (Eds.), Clinical Thoracic Anesthesia. Springer, Singapore, pp: 275-282.
-
Lisenmeier U, Krotz M, Hauser H (2002) Whole body computed tomography in polytrauma. Eur Radiol 12(7): 1728-1740.
-
Zinck SE, Primack SL (2000) Radiographic and CT Findings in Blunt Chest Trauma. Journal of Thoracic Imaging 15(2): 87-96.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index