Role of Vena Cava Inferior Ultrasound in Volume Assesment
Regulation of body fluid volume is a key concern for physicians in intensive care units. In intensive care, it is most important to determine the intracellular fluid status because it directly affects the volume status of the patient. Ultrasonography appears to be a useful tool for the assessment of body fluid status. The gold standard for measuring central venous pressure (CVP) is a central venous catheter. Vena cava inferior ultrasound (US-VCI) has been proposed as the non-invasive technique of choice for CVP assessment due to its wide availability, low costs, and ease of use. While a depleted IVC is often observed in hypovolemic patients, typically the IVC is dilated in a hypervolemic condition with a less pronounced or null respiratory collapse in the appropriate clinical context. respiratory variability in VCI diameteris known as the caval index (collapsibility index=VCImax- VCImin /VCImax) and is considered to reflect the intravascular volume state. According to the current updated American and European guidelines, an IVC diameter ≤2.1 cm and collapsibility >50% during inspiration suggest a RAP between 0–5 mm Hg while a diameter >2.1 cm with <50% inspiratory collapse indicates a high RAP of 10–20 mmHg. Primarily because of complicated pathophysiological mechanisms, ultrasound measurement of VCI should not be used as the only parameter in the assessment of volemic status.
Introduction
Regulation of body fluid volume is a key concern for physicians in intensive care units. In intensive care, it is most important to determine the intracellular fluid status because it directly affects the volume status of the patient [1]. Fluid responsiveness is challenging in the management of critically ill patients [2]. Ultrasonography appears to be a useful tool for the assessment of body fluid status. There is a significant range of modalities available to assess intracellular water volume. Point-of-care ultrasonography (POCUS) is widely recognized its usefulness in complementing the physical examination and serving as a safe interventional guidance at the bedside [3]. This method enables a non-invasive assessment of the degree of hydration in real time, and due to its reproducibility, it is also suitable for monitoring. The results of ultrasound assessment of the degree of hydration correlate with those obtained by other reference methods [1].
Right atrial pressure (RAP) is most important for evaluation of the intravascular volume status. The gold standard for measuring central venous pressure (CVP) is a central venous catheter. Vena cava inferior ultrasound (US- VCI) has been proposed as the non-invasive technique of choice for CVP assessment due to its wide availability, low costs, and ease of use [4].
Ultrasound measurement of the diameter of the inferior vena cava (US-VCI) and the degree of respirophasic collapse was initially used by nephrologists and later by cardiologists. It has recently been integrated into several critical care/ emergency ultrasound protocols as a non-invasive assessment of central venous pressure (CVP). In order to achieve a more accurate repeated measurement, especially in intensive care units, it is necessary that the measurement is always performed by the same doctor - either a radiologist or a practicing anesthesiologist.
The role of this review is to point out the importance of measuring the inferior vena cava in order to determine the volemic status, to show the measurement technique, to explain different ultrasound presentation of the inferior vena cava, but also to show the limits of the ultrasound assessment of the volemic status.
Technique
For a good examination of the VCI, low-frequency convex probe (2–5.5 MHz) with high penetration of ultrasound waves is used for a good assessment of the diameter of the VCI, including the veno–atrial junction and the right atrium. The probe is usually placed in a transverse scan in the epigastrium at the level of the right hemiabdomen below the level of the xiphoid process and intrahepatic segment of VCI must be examined with the inner walls clearly imaged (Figure 1). In a certain percentage of cases, a larger amount of gas in transversal colon or stomach disable good visualization of the VCI, so we can place the probe transversely at the level of the anterior axillary line on the right side. Visualization of the aorta is also important for determining the volemic status, so it would be useful to directly visualize both the aorta and the VCI at the same time during the examination.
Imaging Spectrum of VCI
Initially, during the examination after visualization of the VCI, we measure its baseline diameter. The threshold value of VCI baseline diameter it is considered that the CVP is higher than 10 mmHg is 2cm. While a depleted IVC is often observed in hypovolemic patients, typically the IVC is dilated in a hypervolemic condition with a less pronounced or null respiratory collapse in the appropriate clinical context [5].
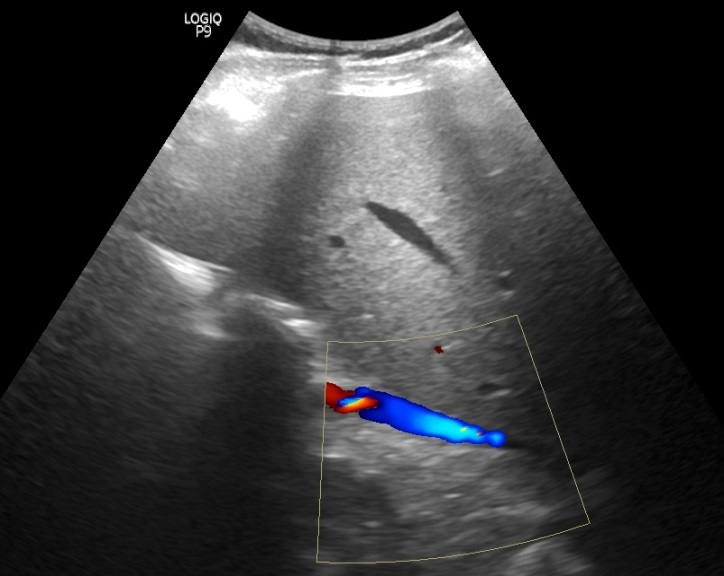
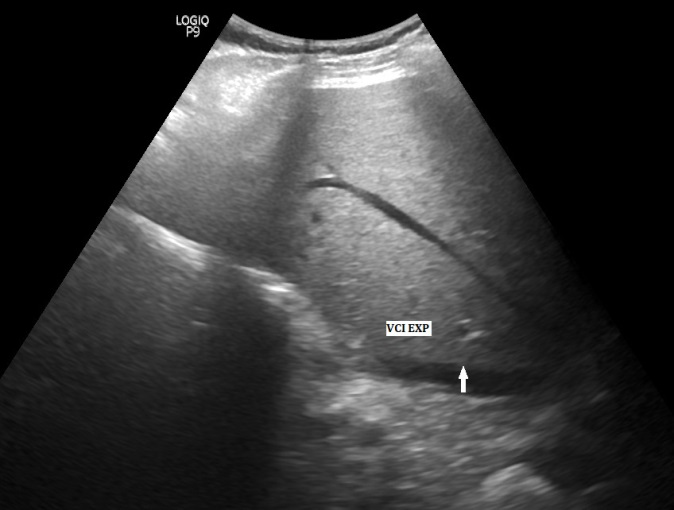
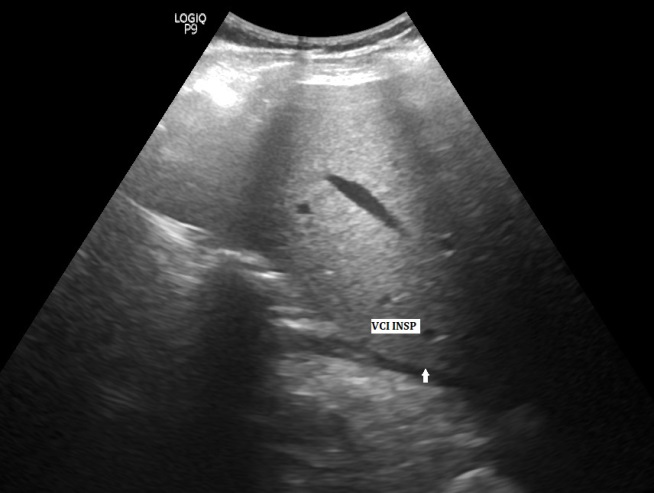
The maximum VCI diameter must be obtained during the inspiratory and expiratory phase of the respiratory cycle (Figures 2 & 3). In people with spontaneous breathing, intrathoracic pressure decreases during inspiration, the pressure difference between the right atrium and vena cava inferior (VCI) increases, bloodflow accelerates and causes VCI-diameter collapse. During expiration, the intrathoracic pressure rises again and the pressure difference between the right atrium and vena cava inferior decreases, leading to an increase in the diameter of the vena cava inferior. This respiratory variability in VCI diameteris known as the caval index (collapsibility index=VCImax-VCImin /VCImax) and is considered to reflect the intravascular volume state [6].
According to the current updated American and European guidelines (Table 1), an IVC diameter ≤2.1 cm and collapsibility >50% during inspiration suggest a RAP between 0–5 mm Hg while a diameter >2.1 cm with <50% inspiratory collapse indicates a high RAP of 10–20 mmHg; a mean pressure value of 8 mmHg is used if the clinical picture does not follow the proposed pattern [7]. The IVC/Ao ratio – both the value before giving fluid and the percentage change in value – can be statistically significant and help to predict fluid responsiveness with the optimal cutoff at 0.675 has sensitivity and specificity of 70.3% and 61.9%, respectively [8]. The IVC/Ao index has been found to be useful for the evaluation of preoperative and intraoperative volume status, especially in a major surgery with marked fluid shift or blood loss [1]. Overall, a statistically significant non-linear correlation was described between the sonographic dimensional parameters of IVC and CVP [9]. In outpatients undergoing haemodialysis, standardization of IVC diameter to body surface area (BSA) was recommended (i.e., IVC diameter 2.1 cm if BSA > 1.61 m2, IVC diameter 1.7 cm when BSA < 1.61 m2) [10]. The presence of continuous flow from the IVC to the RA corresponds to a low to normal CVP; on the contrary, an interrupted waveform indicates a high RAP only if it is associated with other ultrasound indices such as the IVC size and cIVC [11]. Regarding the non-invasive estimation of CVP, current evidence does not support the use of the IVC diameter in mechanically ventilated patients. In a recent meta-analysis that included 16 studies, the correlation between CVP and IVC diameter was not statistically significant in 8 studies and was weak to moderate in the others [12].
| Caval Index | Right Atrial Pressure (mmHg) | |
|---|---|---|
| < 21mm | > 50% | 0-5mmHg |
| > 21mm | > 50% | 5-10mmHg |
| > 21mm | < 50% | 10-20mmHg |
Table 1: The American Society of Echocardiography reccomendations.
Limitations
Certain clinical conditions affect the state of intravascular pressure and thus may render the ultrasound assessment of volemic status inaccurate. Pericardial tamponade, acute massive pulmonary embolism, intraabdominal hypertension including pregnancy, asthma/COPD exacerbations and mechanically ventilated patients with positive pressures represent conditions where the IVC measurement may fail in indicating reliably the volume status [13]. Of course, if the examination technique is not performed correctly, there may also be measurement errors and incorrect estimation of volemic status. A correct interpretation of the volume status through the IVC assessment should always combine the respiratory variation of the IVC with its absolute size.
Conclusion
For all these reasons, and primarily because of complicated pathophysiological mechanisms, ultrasound measurement of VCI should not be used as the only parameter in the assessment of volemic status.
Recently, the combination of VCI measurement with other blood vessels measurement is often used in order to avoid wrong conclusions. The splanchnic system is considered autonomous from the systemic circulation and ultrasound measurement cannot be used for these purposes. In conclusion, VCI diameter cannot be used as a separate parameter, but can be used in combination with other parameter to improve the monitoring volemic status and prognosis of severe patients.
The research data associated with a paper is available and the data can be accessed. There are no funders to report for this submission.
The authors whose names are listed immediately above certify that they have NO affiliations with or involvement in any organization or entity with any financial interest or non- financial interest in the subject matter or materials discussed in this manuscript.
References
-
Piotrkowski J, Buda N, Januszko-Giergielewicz B, Kosiak W (2019) Use of bedside ultrasound to assess fluid status: a literature review. Pol Arch Intern Med 129(10): 692-699.
-
Sulovic LJ, Sulovic N (2016) The role of echocardiography measurement index collapsing VCI in evaluation of dyalisis and determing the state of hydration. Praxis Med 45(2): 49-54.
-
Blanco P, Volpicelli G (2016) Common pitfalls in point- of-care ultrasound: a practical guide for emergency and critical care physicians. Crit Ultrasound J 8: 15.
-
Nicolò DP, Tavazzi G, Nannoni L, Corradi F (2023) Inferior Vena Cava Ultrasonography for Volume Status Evaluation: An Intriguing Promise Never Fulfilled. J Clin Med 12(6): 2217.
-
Perera P, Mailhot T, Riley D, Mandavia D (2010) The RUSH exam: rapid ultrasound in SHock in the evaluation of the critically lll. Emerg Med Clin North Am 28(1): 29-56.
-
Kicher BJ, Himelman RB, Schiller NB (1990) Noninvasive estimation of right atrialpressure from the inspiratory collapse of the inferior vena cava. Am JCardiol 66: 493- 496.
-
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, et al. (2015) Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 28(1): 1-39.
-
Permata KN, Abdul L, Hocky PA (2021) Inferior Vena Cava/Abdominal Aorta Ratio as a Guide for Fluid Resuscitation. J Emerg Trauma Shock 14(4): 211-215.
-
Beigel R, Cercek B, Luo H, Siegel RJ (2013) Noninvasive Evaluation of Right Atrial Pressure. J Am Soc Echocardiogr 26(9): 1033-1042.
-
Taniguchi T, Ohtani T, Nakatani S, Hayashi K, Yamaguchi O, et al. (2015) Impact of Body Size on Inferior Vena Cava Parameters for Estimating Right Atrial Pressure: A Need for Standardization. J Am Soc Echocardiogr 28(12): 1420-1427.
-
Ranjan R, Toroghi MH, Pressman GS, Schiller NB (2019) Doppler Recognition of Low or Normal Central Venous Pressure from Continuous Flow from Inferior Vena Cava into Right Atrium. Am J Cardiol 124(3): 448-452.
-
Ciozda W, Kedan I, Kehl DW, Zimmer R, Khandwalla R, et al. (2016) The Efficacy of Sonographic Measurement of Inferior Vena Cava Diameter as an Estimate of Central Venous Pressure. Cardiovasc Ultrasound 14(1): 33.
-
Juhl-Olsen P, Frederiksen CA, Sloth E (2012) Ultrasound Assessment of Inferior Vena Cava Collapsibility Is Not a Valid Measure of Preload Changes during Triggered Positive Pressure Ventilation: A Controlled Cross-over Study. Ultraschall Med 33(2): 152-159.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index