The Impact of Various Anesthetic Techniques on Cerebral Oxygenation during Spinal Surgery Performed in a Prone Position with Controlled Hypotension
Background: While prone positioning during anesthesia is necessary for certain surgical procedures, it also increases the risk of postoperative neurological complications. This risk is exacerbated by controlled hypotension used to minimize blood loss during spinal surgeries. Monitoring regional cerebral oxygen saturation (rScO2) is essential for maintaining cerebral oxygenation and preventing adverse outcomes like cognitive dysfunction and organ failure. This study aimed to evaluate the effect of different anesthetic techniques on cerebral oxygenation in patients undergoing spinal surgery in the prone position with controlled hypotension. Methods: Fifty-four patients scheduled for spinal surgery in a prone position with controlled hypotension were randomly assigned into two equal groups, to receive sevoflurane or propofol anesthesia. Data were collected at various intervals: before and after anesthesia induction, post-induction in the prone position, during surgery, and before awakening in the supine position. Parameters recorded included rScO2, peripheral oxygen saturation (SpO2), heart rate (HR), patient state index (PSI), end-tidal carbon dioxide tension (ETCO2), and mean arterial pressure (MAP). Results: rScO2 levels decreased in both patient groups once positioned in the prone position. However, the rScO2 values were significantly lower in the propofol group compared to the other group (p = 0.025, 0.032 respectively). Conclusion: The study suggests that propofol as the anesthetic agent may have exacerbated the decline in cerebral oxygenation associated with the transition to prone positioning. Sevoflurane might thus be preferable for patients at risk of compromised cerebral oxygenation.
Abbreviations
HR: Heart Rate; PSI: Patient State Index; MAP: Mean Arterial Pressure; PP: Prone Position; NIRS: Near Infrared Spectroscopy; ASA: American Society of Anesthesiologists; MAP: Mean Arterial Pressure; CPP: Cerebral Perfusion Pressure; SVR: Systemic Vascular Resistance.
Introduction
The prone position (PP) is commonly utilized for surgical procedures involving the posterior aspect of the spine. The physiological effects of postural changes during anesthesia are complicated, influencing both systemic and cerebral circulation, potentially reducing cerebral blood flow (CBF) and oxygenation [1]. Complications such as cerebral ischemia, and spinal cord injury have been associated with the PP [2]. Furthermore, PP can increase intracranial pressure, adversely affecting cerebral perfusion and venous drainage [3]. Pressure from supporting pillows or the positioning of the patient’s neck can potentially distort or restrict blood vessels [4].
The main objective of such procedures is to ensure adequate cerebral perfusion and oxygenation while minimizing the risk of complications. Inducing controlled hypotension is commonly employed in spinal surgical procedures. Research and clinical practice recommend that the controlled hypotensive target indicated by MAP was maintained at 70–80% of the baseline which not only decreases intraoperative bleeding and improves the quality of the surgical field, but also is still within safe levels [5]. However, this strategy may also have the unintended consequence of decreasing cerebral perfusion and oxygenation [6]. Anesthetic medications can affect CBF, which is crucial during neurosurgical procedures. These medications can influence the delivery of oxygen and nutrients to neurons and alter the dynamics of cerebral blood vessels [7].
Inhalational agents commonly used in general anesthesia for spinal surgeries, can cause cerebral vasodilation, increasing CBF and oxygenation. The difference between CBF and oxidative metabolism is likely due to the effect of volatile anesthetics on cerebral vascular resistance [8]. However, managing the depth of anesthesia and the concentration of inhalational agents is crucial to avoid excessive vasodilation and hypotension, which can impair rScO2 [9]. Total Intravenous Anesthesia (TIVA), offers precise control over the depth of anesthesia and avoids the vasodilatory effects of inhalational agents. By preserving a more consistent cardiovascular profile, TIVA may be advantageous in helping to maintain adequate rScO2 and perfusion, throughout spinal surgeries [10].
Cerebral oximetry is a technique that continuously and noninvasively monitors rScO2 in the frontal cortex using near-infrared spectroscopy (NIRS) [11]. It provides real- time intraoperative insight into brain oxygenation, acting as a warning for cerebral deoxygenation that could affect outcomes. Additionally, cerebral oximetry positions the brain as a key indicator of the adequacy of tissue perfusion and oxygenation in other vital organs to prevent complications from undetected tissue hypoxia, which might not be identified with conventional invasive hemodynamic monitoring [12].
Materials and Methods
This prospective, randomized, double-blinded study was conducted between February and August 2024. The study was registered with the ClinicalTrials.gov registry (NCT06325462). After obtaining approval from the institutional ethics committee (IRB: HP-01-R079) and securing written informed consent from the participants, the researchers recruited 54 adult patients classified as American Society of Anesthesiologists (ASA) physical status I or II. These patients were between 18 and 65 years of age and were scheduled for elective spinal surgery to be performed in the prone position under general anesthesia with controlled hypotension. All patients who met the inclusion criteria agreed to participate in the study.
Patients were excluded if they had a history of uncontrolled hypertension, coronary artery disease, renal or hepatic insufficiency, neurodegenerative disorder, coagulopathy, intraoperative blood loss of ˃ 200 ml, or intraoperative hemodynamic instability. The researchers ensured that all participants had given their written informed consent before being enrolled in the research project in the preoperative area.
Procedure
In the preoperative area, all patients underwent the same preparatory procedures. They were then randomly divided into two equal groups: Group S and Group P. Patients in Group S received general anesthesia induced and maintained with the inhalational agent sevoflurane. Those in Group P were administered intravenous anesthesia with a propofol infusion. No premedication was given to the participants. Standard monitoring was employed, including electrocardiography, non-invasive blood pressure measurement, SpO2, ETCO2, and PSI using a sedation monitor (SedLine, Masimo Corp, Irvine, CA 92618). rScO2 was assessed with a Masimo O3 regional oximeter (Root® with O3® Regional Oximetry, Masimo Corp, Irvine, CA 92618). Before data collection, the skin on the patients’ foreheads was cleansed with alcohol to ensure good signal quality and minimize artifacts on both monitoring devices. During the surgical procedure, the degree of neuromuscular blockade was tracked using a Train of Four (TOF) Watch (Organon Teknika, Durhman, USA). Additionally, the inspired and expired oxygen fractions, the end-tidal concentration of sevoflurane, and the esophageal temperature were monitored using a Drager Perseus®
A500 workstation (Lubeck, Germany). The esophageal temperature was maintained between 36°C and 36.8°C using a Bair Hugger warming blanket (3M, MN55144, USA). After preoxygenation, all participants received an intravenous dose of fentanyl at 2 μg/kg. For patients in Group S, general anesthesia was induced by increasing the inspired concentration of sevoflurane to 7% until loss of consciousness, after which it was reduced to 2%. In Group P, anesthesia was induced with a propofol bolus of 2 mg/kg. All patients were administered cisatracurium at 0.2 mg/kg and orotracheal intubation was performed when TOF = 0 was achieved. The patients were mechanically ventilated using a Drager Perseus® A500 workstation (Lubeck, Germany). The mechanical ventilation parameters were adjusted to maintain a tidal volume of 7 ml/kg and an ETCO2 value between 30-35 mmHg.
Anesthesia was maintained with either propofol (4-8 mg/kg/h) for Group P or sevoflurane (1-2% end- tidal concentration, 40/60% O2/Air mix) for Group S, titrated to achieve a PSI of 25-50 [13]. Both groups also received remifentanil infusions at the anesthesiologist’s discretion, with doses ranging from 0.05-0.3 μg/kg/min. Neuromuscular blockade was maintained with cisatracurium boluses, keeping one or two responses in a TOF stimulation. Intraoperative controlled hypotension was achieved using dexmedetomidine infusion with a loading dose of 1 µg/ kg over 10 min after induction, followed by a maintenance infusion of 0.4–0.8 µg/kg/h before the surgical incision. The infusion rate was adjusted in both groups to maintain a MAP of 20–30% below baseline. A fluid bolus and 5 mg of intravenous ephedrine were administered when the MAP dropped ˃ 30% from the baseline value.
Simultaneously, the following parameters; SpO2, HR, invasively monitored MAP, ETCO2, PSI, and rScO2 were recorded at various pre-determined time points during the investigation. T1: Before induction, with the patient in the supine position. T2: Supine position, with the patient receiving oxygen administration. T3: After induction, with the patient still in the supine position. T4: Before the start of surgery, after the patient had been turned to the prone position.
T5: 10 minutes after the patient was placed in the prone position. T6: 2 hours after the patient was placed in the prone position. T7: At the end of the surgery, during skin suturing, with the patient in the prone position. T8: After the patient had been repositioned to the supine position. Cerebral oxygen desaturation was defined as a decline in rScO2 of more than 20% from the baseline value, lasting for longer than 15 seconds [14]. An investigator who was not involved in designing the protocol or assigning randomization numbers was responsible for recording all the data.
Statistical Analysis
The sample size for each group was set at 25 patients, which provided 80% power to detect a clinically meaningful decrease in rScO2. The expected mean difference was 10, with an estimated standard deviation of 5, and the significance level (alpha) was set at 0.05, using a two-sided two-sample t-test. Qualitative data were analyzed using Pearson’s Chi- square test and presented as number [%]. Quantitative data were analyzed using the unpaired t-student test for between-group comparisons and the paired t-test for within- group comparisons. The quantitative data were presented as mean ± standard deviation. A p-value of less than 0.05 was considered statistically significant. The statistical analysis was performed using the Statistical Package for Social Sciences SPSS software (version 26.0, Armonk, NY, USA).
Results
This prospective study included 54 patients between 18 and 65 years of age, who were scheduled for elective spinal surgery in the PP under general anesthesia with controlled hypotension. All patients agreed to participate, and no one declined. Two patients were excluded from the final analysis; one in the S group due to excessive bleeding (more than 300 ml), and another in the P group due to a malfunction of the cerebral oximetry probe.
The demographic and clinical characteristics were similar between the two groups, and no significant differences were observed (p > 0.05) (Table 1).
| Sevoflurane Group (n = 26) | Propofol Group (n = 26) | P-value | |
|---|---|---|---|
| Age (years) | 54.6 ± 9.5 | 56.3 ± 7.8 | 0.781 |
| Sex | |||
| Male | 14 (53.8%) | 13 (50%) | 0.604 |
| Female | 12 (46.2%) | 13 (50%) | 0.604 |
| Body Mass Index (Kg/m2) | 26.7 ± 4.56 | 27.5 ± 4.01 | 0.335 |
| ASA | |||
| I | 9 (34.6%) | 11 (42.3%) | 0.597 |
| II | 17 (65.4%) | 15 (57.7%) | 0.597 |
| Duration of Anesthesia (min) | 278.5 ± 22.71 | 289.2 ± 20.54 | 0.71 |
| Duration of Prone Position (min) | 233.2 ± 10.51 | 241.92 ± 17.22 | 0.854 |
| Type of surgery | |||
| Posterior instrumentation | 10 (38.4%) | 11 (42%) | 0.152 |
| Lumbar discectomy | 8 (30.8%) | 6 (23%) | 0.152 |
| Lumbar laminectomy | 8 (30.8%) | 9 (35%) | 0.152 |
Table 1: Demographic variables and intraoperative variables. Data are mean ± S.D. or numbers.
The study found that rScO2 declined in both experimental groups after the patients were placed in the PP. However, when comparing the two groups, rScO2 values were significantly lower in the P group compared to the S group at two specific time points - 10 minutes and 2 hours after the patients were placed in the prone position (p = 0.025 and 0.032, respectively) (Table 2).
| Sevoflurane Group | Propofol Group | P-value | |
|---|---|---|---|
| Supine without O2 | 63.38 ± 7.24 | 64.92 ± 9.11 | 0.2 |
| Supine with O2 | 66.15 ± 6.89 | 66.94 ± 5.92 | 0.1 |
| Intubation supine | 69.38 ± 7.04 | 68.9 ± 7.51 | 0.4 |
| Just after prone | 67.06 ± 5.71 | 65.91 ± 6.78 | 0.7 |
| 10 min after prone | 64.38 ± 7.11 | 61.37 ± 6.32 | 0.025* |
| 2 H after prone | 68.37 ± 6.32 | 62.92 ± 9.11 | 0.032* |
| End of surgery prone | 68.54 ± 6.78 | 68.95 ± 7.51 | 0.1 |
| End of Anesthesia supine | 70.92 ± 7.51 | 68.54 ± 6.78 | 0.3 |
Table 2: rScO2 for patients with the sevoflurane and propofol groups. Values are mean ± S.D. p-value ˂ 0.05 was considered statis
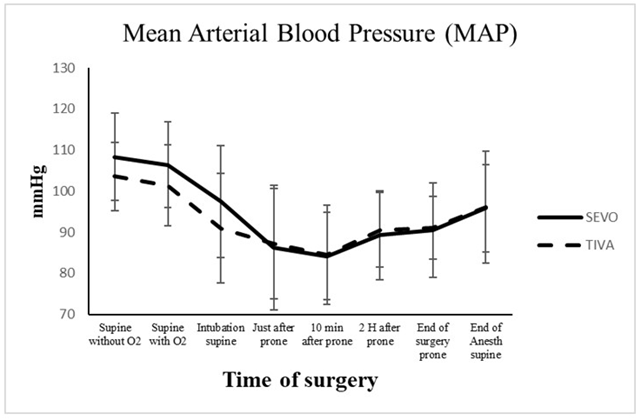
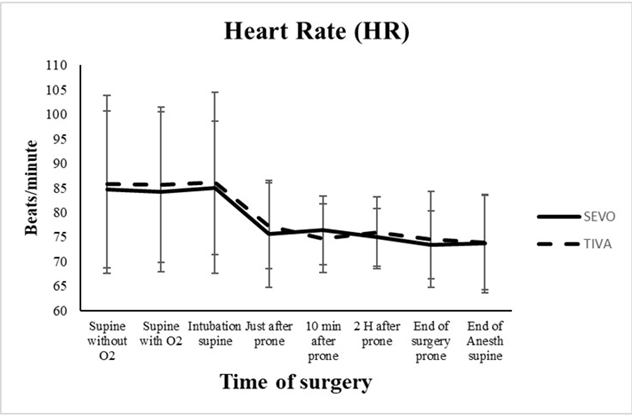
When comparing the two groups, the study found no significant differences in HR, MAP, SPO2, ETCO2, and PSI parameters at any of the measured time points (p > 0.05). However, there were statistically significant differences in MAP (p = 0.03, 0.0002, 0.0001 in the S group and p = 0.01, 0.004, 0.002 in the P group) and HR (p = 0.04, 0.03, 0.01 in the S group and p = 0.01, 0.04, 0.01 in the P group) compared to baseline values after the induction of anesthesia and at different time intervals (Figures 1 & 2).
There was a statistically significant increase in SpO2
levels at all measurement intervals in both groups (p = 0.003, 0.005, 0.001 in the S group and p = 0.002, 0.004, 0.004 in the P group). Concerning the PSI, there were significant decreases at different time intervals within each group compared to the pre-induction values (p = 0.02, 0.001, 0.001 in the S group and p = 0.04, 0.001, 0.001 in the P group). Regarding ETCO2, there were statistically significant differences between the pre-induction condition and the other measured conditions after the patients were placed in the prone position in both groups (p = 0.003, 0.001, 0.002 in the S group and p = 0.002, 0.001, 0.001 in the P group).
Discussion
The main focus of the present study was to evaluate rScO2. The researchers observed a gradual decline in rScO2 values over time in the S and P groups after the patients were turned to the PP. However, this reduction in rScO2 was significantly more pronounced in the P group compared to the other group. The study identified two critical time points for evaluating rScO2 values at T5 and T6. These time points coincided with the period patients were in the PP. The results indicated that MAP values decreased in both groups following the induction of anesthesia (T3), but rScO2 values did not show a similar decline. This may be due to the administration of 100% oxygen during the induction of anesthesia. However, the reduction in MAP from baseline did not exceed the range of cerebral auto regulation, typically between 60 and 150 mmHg. As a result, rScO2 values could return to baseline levels in less than 2 hours after the patients were placed in the PP in the S group. Conversely, the rScO2 values in the P group did not reach baseline levels within the same 2-hour timeframe while the patients were in the PP. This may be due to sevoflurane’s recognized ability to maintain cerebral perfusion more effectively during surgery, thereby enhancing oxygen delivery to the brain. Additionally, its sympatholytic effects can lead to reduced vasoconstriction and improved regulation of cerebral blood flow compared to propofol. Furthermore, sevoflurane may have a lesser effect on the cerebral metabolic rate for oxygen consumption, contributing to a more favourable balance between oxygen delivery and utilization.
This observation is consistent with findings from previous research in the field. For instance, a study conducted by Babakhani B, et al [15] demonstrated that after 30 and 60 minutes in the prone position, rScO2 significantly decreased compared to the values measured in the supine position [15]. Moreover, oxygen desaturation co-occurs with a significant decrease in blood pressure and pulse rate. However, at 90 minutes, the rScO2 values returned to baseline levels. This decrease in rScO2 has been attributed to the sympatholytic effects of general anesthetic agents [15]. Additionally, a study by Meng L, et al. [16] has reported similar observations [16].
The PP used in spinal surgery leads to physiological changes affecting CBF and rScO2. The primary cause is the compression of the inferior vena cava and its branches, which leads to blood deposition in the epidural venous plexus. This can favour intraoperative blood loss, reduce blood return to the systemic circulation, and ultimately impact cerebral blood flow [17].
The research team reported that both HR and MAP declined after the induction of anesthesia, and then again after the patient was placed in the prone position. It aligns with previous research highlighting the various factors influencing cerebral oximetry values. A study conducted by Fassoulaki A, et al. [18] has emphasized that several factors can modulate cerebral oximetry values, including depth of anesthesia, anesthetic technique, arterial carbon dioxide concentrations, inspired oxygen content, and mean arterial pressure (MAP) [18]. To address these factors, the authors of the current investigation, carefully standardized the anesthetic management in both groups. MAP was maintained between 20-30% below baseline, ETCO2 at 30–35 mmHg, and PSI readings (25-50) to represent a stable depth of anesthesia throughout the anesthesia course, with no significant differences between the groups.
Backofen et al. [19] reported that the change in posture from the supine to PP in anesthetized patients results in a reduction in MAP and cerebral perfusion pressure (CPP). In awake patients, this postural change triggers sympathetic nervous system activation, which increases systemic vascular resistance and HR to maintain MAP and cardiac output. However, in anesthetized patients, the sympathetic nervous system activation is attenuated by the vasodilating effect of anesthetic drugs. These hemodynamic changes may cause a reduction in CBF and rScO2 [19].
Badia JR, et al. [20] suggested that the effect of the prone position is a complex combination of various factors, such as increased abdominal pressure, thoracic compression and disrupted venous return, effects on cardiac output, respiratory dynamics, and intracranial circulation, as well as changes in MAP [20].
Conversely, other studies have indicated that the prone position positively affects a patient’s SpO2. They found that pulmonary atelectatic regions, which are concentrated in the posterior lung in the supine position, can dissolve in the prone position, leading to decreased intrapulmonary shunting and increased perfusion in the ventral regions, ultimately resulting in improved oxygenation [3]. Additionally, Bombardieri et al. evaluated CBF velocity using transcranial Doppler ultrasonography during PP for spine surgery. They demonstrated preservation of cerebral perfusion during stable systemic hemodynamic conditions [21]. Sniedze M, et al. [22] further emphasized the importance of monitoring rScO2 during these procedures, as they found no correlation between rScO2 and other intraoperatively monitored parameters, such as MAP, SpO2, and EtCO2. Therefore, without rScO2 monitoring, episodes of cerebral desaturation might have gone unnoticed [22].
Our analysis revealed a significant reduction in rScO2 values specifically in the P group following the transition to the PP. In contrast, comparatively smaller changes were observed in patients receiving sevoflurane anesthesia. Previous studies have reported that different anesthetic agents can affect rScO2 differently. Slupe AM [23] and Kim JY [24] found that desflurane causes dose-dependent decreases in cerebrovascular resistance and cerebral metabolic rate of oxygen consumption, while propofol is associated with a dose-dependent reduction of CBF and cerebral metabolic rate, leading to a decrease in intracranial pressure. Compared to volatile anesthetics administered at equivalent bispectral index (BIS) doses, propofol causes a significant reduction in CBF and a similar decrease in cerebral metabolic rate of oxygen consumption [23, 24]. Closhen D, et al. [25] studied the changes in rScO2 following prone positioning using 2 different monitors, an INVOS cerebral oximeter for continuous rSO2 measurement and a FORE-SIGHT cerebral oximeter for absolute cerebral tissue oxygenation (StO2) measurement, while also comparing awake and anesthetized patients [25]. Propofol 2 mg/kg was used for induction and sevoflurane 0.7-1.0 MAC to maintain anesthesia. They reported an initial decrease in rSO2 (from 75%±8% to 72%±8%) and StO2 (from 74%±5% to 72%±4%) in anesthetized patients after PP with a subsequent increase rate of 0.0324%/min. Awake volunteers did not exhibit significant changes in rScO2 after being placed in the PP [25].
Sudheer PS, et al. [26] reported a more significant decrease in cardiac index (CI) and an increase in systemic vascular resistance (SVR) when transitioning to the PP during TIVA (25.9% decrease in CI) compared to inhalation anesthesia (12.9% decrease in CI). They suggested that the reduction in CI in the prone position could be attributed to increased intrathoracic pressures, which can lead to decreased arterial filling and an increase in sympathetic activity via the baroceptor reflex. Their study demonstrated decreased stroke volume accompanied by increased sympathetic activity (increased heart rate, total peripheral vascular resistance, and plasma noradrenaline) in PP [26].
However, a potential contributor to these observations could be a change in propofol pharmacokinetics in the prone position. Measured propofol concentrations have been observed to increase during target-controlled infusions when patients are transferred from the supine to the PP, likely attributed to the decrease in cardiac output [27]. Similarly, Valencia et al. reported that rScO2, as measured by near- infrared spectroscopy (NIRS), may be better preserved with sevoflurane anesthesia compared to propofol. This finding was also supported by studies using jugular venous oxygen saturation (SjO2) as a measure of rScO2 [7].
In contrast, a study by Koraki E, et al. [28] found that both desflurane and propofol anesthesia were associated with a significant decrease in rScO2 when patients were in the prone position, with no notable differences between the two anesthetic agents [28]. Similarly, Deiner S, et al. [29] research suggested no significant differences between these anesthetic drugs throughout the prone positioning period [29].
Furthermore, a study by Nowak et al. evaluated patients undergoing functional endoscopic sinus surgery (FESS) with the Mini-Mental State Examination in 3 groups (mild hypotension [MAP >75%], intermediate hypotension [MAP 65-75%], severe hypotension [MAP 53-65%]) compared with preoperative blood pressure. The findings indicated that these varying degrees of controlled hypotension appeared to be equally safe for the patients, implying that the degree of induced hypotension may not be a critical factor in this surgical context, while simultaneously decreasing the complication rate, such as renal, lung, cardiovascular system damage, and postoperative cognitive decline [30].
Wang et al. demonstrated that a decrease in rScO2 can be used to predict delirium and that continuous monitoring of rScO2 can reduce the incidence of postoperative delirium [31]. Another study revealed that the duration of decline in rScO2 below 60% during lumbar spinal surgery was correlated with the development of postoperative cognitive dysfunction [32]. These findings suggest that monitoring rScO2 and timely intervention can help reduce the occurrence of postoperative neurological disorders.
The current study acknowledges a limitation in that it did not evaluate the potential impact of the observed changes in rScO2 on the patients’ cognitive functions. However, the authors did not observe any cerebral oxygen desaturation in group P compared to group S. Further research with larger sample sizes is needed to confirm these findings.
In conclusion, this appears to be the first study in the literature to evaluate the effect of different anesthetic techniques on rScO2 during spinal surgery with controlled hypotension in the prone position. The findings imply that sevoflurane may be a better anesthetic choice in clinical scenarios where there is a concern about maintaining adequate cerebral perfusion and oxygenation. Its cerebral hemodynamic properties may make it a more suitable option than other anesthetic agents when the patient’s oxygen delivery to the brain is threatened or impaired.
References
-
Melissa MK, Yik HH, Warren MR (2015) The Prone Position During Surgery and its Complications: A Systematic Review and Evidence-Based Guidelines. Int Surg 100(2): 292-303.
-
Chaix I, Manquat E, Liu N, Casadio MC, Ludes PO, et al. (2020) Impact of hypotension on cerebral perfusion during general anesthesia induction: a prospective observational study in adults. Acta Anaesthesiol Scand 64(5): 592‐601.
-
Reinprecht A, Greher M, Wolfsberger S, Dietrich W, Illievich UM, et al. (2003) Prone position in subarachnoid hemorrhage patients with acute respiratory distress syndrome: effects on cerebral tissue oxygenation and intracranial pressure. Crit Care Med 31(6): 1831-1838.
-
Hojlund J, Sandmand M, Sonne M, Mantoni T, Jorgensen HL, et al. (2012) Effect of head rotation on cerebral blood velocity in the prone position. Anesthesiol Res Pract 2012: 647258.
-
Zhao Y, Zang C, Ren S, Fu J, Liu N, et al. (2022) Effects of different levels of controlled hypotension on regional cerebral oxygen saturation and postoperative cognitive function in patients undergoing total knee arthroplasty. Front Med 9: 989341.
-
Hsieh JK, Dalton JE, Yang D, Farag ES, Sessler DI, et al. (2016) The association between mild intraoperative hypotension and stroke in general surgery patients. Anesth Analg 123(4): 933‐ 939.
-
Valencia L, Rodriguez PA, Kuhlmorgen B, Santana RY (2014) Does sevoflurane preserve regional cerebral oxygen saturation measured by near-infrared spectroscopy better than propofol? Ann Fr Anesth Reanim 33(4): e59-65.
-
Ishida K, Berger M, Nadler J, Warner DS (2014) Anesthetic neuroprotection: antecedents and an appraisal of preclinical and clinical data quality. Curr Pharm Des 20: 5751-5765.
-
Baburamani A, Joakim Ek, Walker D, Castillo MM (2012) Vulnerability of the developing brain to hypoxic-ischemic damage: contribution of the cerebral vasculature to injury and repair? Front Physiol 3: 424-445.
-
Fu KH, Cheng H, Teng W, Hsu PK, Hsu HS, et al. (2023) Total intravenous anesthesia decreases hospital stay but not incidence of postoperative pulmonary complications after lung resection surgery: a propensity score matching study. BMC Anesthesiol 23(1): 345-353.
-
Ali J, Cody J, Maldonado Y, Ramakrishna H (2022) Near-infrared spectroscopy (NIRS) for cerebral and tissue oximetry: Analysis of evolving applications. J Cardiothorac Vasc Anesth 36(8 Pt A): 2758- 2766.
-
Fedorow C, Grocott HP (2010) Cerebral monitoring to optimize outcomes after cardiac surgery. Curr Opin Anaesthesiol 23: 89-94.
-
Rick O (2024) PSI 25-50 Range for Optimal Hypnotic State for General Anesthesia. A Clinical Perspective pp: 1-4.
-
Chanon T, Panramon V, Pongkwan J (2021) What Is the Risk of Intraoperative Cerebral Oxygen Desaturation in Patients Undergoing Shoulder Surgery in the Beach Chair Position? Clin Orthop Relat Res 479(12): 2677-2687.
-
Babakhani B, Heroabadi A, Hosseinitabatabaei N, Schott M, Yekaninejad S, et al. (2017) Cerebral oxygenation under general anesthesia can be safely preserved in patients in prone position: A prospective observational study. J Neurosurg Anesthesiol 29(3): 291-297.
-
Meng L, Wang Y, Zhang L, McDonagh DL (2019) Heterogeneity and variability in pressure autoregulation of organ blood flow: lessons learned over 100+ years. Crit Care Med 47(3): 436-448.
-
Murniece S, Soehle M, Vanags I, Mamaja B (2019) Near Infrared Spectroscopy Based Clinical Algorithm Applicability During Spinal Neurosurgery and Postoperative Cognitive Disturbances. Medicina 55(5): 179-188.
-
Fassoulaki, A, Kaliontzi, H, Petropoulos G, Tsaroucha A (2006) The Effect of Desflurane and Sevoflurane on Cerebral Oximetry Under Steady-State Conditions. Anesth & Analg 102(6): 1830- 1835.
-
Backofen JE (1985) Hemodynamic changes with prone positioning during general anesthesia. Anesth Analg 64: 194-199.
-
Badia JR, Sala E, Rodriguez RR (1998) Positional changes and drug interventions in acute respiratory failure. Respirology 3(2): 103-106.
-
Bombardieri AM, Beckman J, Urban M, Gaudio AR, Girardi FP, et al. (2019) An observational study of cerebral blood flow velocity evaluation in the prone position during posterior lumbar surgery. Anesth Analg 129(2): 487- 492.
-
Murniece S, Soehle M, Vanags I, Mamaja B (2020) Regional Cerebral Oxygen Saturation Monitoring during Spinal Surgery in Order to Identify Patients at Risk for Cerebral Desaturation. Appl. Sci 10(6): 2069-2077.
-
Slupe AM, Kirsch JR (2018) Effects of anesthesia on cerebral blood flow, metabolism and neuroprotection. J Cereb Blood Flow Metab 38: 2192-2208.
-
Kim JY, Lee JS, Lee KC, Kim HS, Kim SH, et al. (2014) The effect of desflurane versus propofol on regional cerebral oxygenation in the sitting position for shoulder arthroscopy. J Clin Monit Comput 28(4): 371-376.
-
Closhen D, Engelhard K, Dette F, Werner C, Schramm P (2015) Changes in cerebral oxygen saturation following prone positioning for orthopaedic surgery under general anaesthesia: a prospective observational study. Eur J Anaesthesiol 32(6): 381-386.
-
Sudheer PS, Logan SW, Ateleanu B, Hall JE (2006) Haemodynamic effects of the prone position: a comparison of propofol total intravenous and inhalation anaesthesia. Anaesthesia 61(2): 138-141.
-
Takizawa D, Hiraoka H, Nakamura K, Yamamoto K, Horiuchi R (2004) Influence of the prone position on propofol pharmacokinetics. Anaesthesia 59: 1250-1251.
-
Koraki E, Stachtari C, Bagntasarian S, Gkiouliava A, Sifaki F, et al. (2021) Effects of Desflurane Versus Propofol Anesthesia on Regional Cerebral Oxygenation during Spinal Surgery in the Prone Position. Anesthes Clin Res 2(1): 2- 6.
-
Deiner S, Chu I, Mahanian M, Lin HM, Hecht AC, et al. (2014) Prone position is associated with mild cerebral oxygen desaturation in elderly surgical patients. PLoS 9(9): 1-6.
-
Nowak S, Oldak A, Kluzik A, Drobnik L (2016) Impact of controlled induced hypotension on cognitive functions of patients undergoing functional endoscopic sinus surgery. Med Sci Monitor 22: 898-907.
-
Wang X, Feng K, Liu H, Liu Y, Ye M, et al. (2019) Regional cerebral oxygen saturation and postoperative delirium in endovascular surgery: a prospective cohort study. Trials 20(1): 504 -512.
-
Kim J, Shim JK, Song JW, Kim EK, Kwak YL (2016) Postoperative cognitive dysfunction and the change of regional cerebral oxygen saturation in elderly patients undergoing spinal surgery. Anesth Analg 123(2): 436- 444.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index