Hematological and Histopathological Study Effect of Molybdate and Sulfate Alone and in Combination Overloaded Intake on Copper Outcome in Mature Male Rats
The object of this study were to evaluate the effect of molybdate and sulfate overload alone or in combination overload intake on copper outcome with regard toxicopathological changes in mature male rats. Twenty eight adult male rats were housed and arbitrarily divided into four equal groups (seven rat/group) and treated as follows for 60 days: control received distilled water, groups T1 received sodium molybdate 50 mg/kg B.W and T2: given orally 500 mg/kg B.W of sodium sulfate and T3 group were given sodium molybdate and sodium sulfate in combination at half dose in comparison with T1 and T2 doses. The blood tests results, which included Red Blood Cell count, hemoglobin concentration and Packed Cell Volume % that conducted a after one month and at the end of the experiment showed a significant reductions in general but were more in T1 group followed by T2 group, while T3 group showed less decline than that recorded in each of T1 and T2 groups. These functional changes were accompanied by structural changes in the hepatic and renal tissues. Histopathological changes following molybdate (50 mg/kg B.W) exposure were manifested by extensive areas of necrosis, hemorrhage, and hyperplasia of bile ductules. Besides focal area of necrosis and suppurative granuloma observed in livers of rats received 500 mg/kg B.W of sodium sulfate, mild infiltrate of mononuclear cell within the hepatic parenchyma, suppurative granuloma and proliferation of kupffer’s cells with hyperplasia of bile ductules seen in liver of rats received combination of them at half dose. While section of kidney from T1 group showed marked fibrous thickening of the capsule, severe cortical hemosiderosis with infiltrate of plasma cell and neutrophils, While in T2 group showed atrophy of glomerular tuft, focal interstitial mononuclear cells infiltration with deposition of hyaline cast. The histological changes revealed that renal damage was also observed in T3 group but at a little degree, depending on the result of this study it can be concluded that molybdate and sulfate alone and in combination succeeded to induce copper deficiency with severe changes in hematological and histopathological parameters in rats.
Introduction
Molybdenum (Mo) is an essential trace element for virtually normal life. Its role as a cofactor for a number of enzymes e.g. (sulfite oxidase, xanthin oxidase, aldehyde oxidase etc.) that catalyze important chemical transformations in the global carbon, nitrogen, and sulfur cycles [1]. Mo is the least abundant essential micronutrient found in most plant tissues and is often set as the base from which all other nutrients are compared and measured. Molybdenum is utilized by selected enzymes to carry out redox reactions. Enzymes that require molybdenum for activity include nitrate reductase, xanthine dehydrogenase, aldehyde oxidase and sulfite oxidase [2]. Molybdenosis (teart) is a form of molybdenum toxicity that produces a disease in ruminants similar to copper-deficiency. Little data are available on the human toxicity of molybdenum. A gout-like syndrome and pneumoconiosis have been associated with excessive concentrations of molybdenum, but the inadequate design of the studies prevents an adequate determination of the etiology of these effects [3]. It has been long known that the transition element Mo is an essential nutrient for plants, animals and microorganisms. Mo is very abundant in the oceans in the form of the MoO42-anion. And also in soils, the molybdate anion is the only form of Mo that is available for plants and bacteria [4]. Sulfur (S) is found in every cell in the body and is involved in a wide range about 15 function of biochemical functions e.g. Cellular energy production/ metabolism, maintaining blood glucose levels etc [5]. Copper (Cu) have a various roles in biological electron transport and oxygen transportation [6]. Also important in integrity of the C.N.S, elastin and collagen synthesis, melanin production and metabolism of iron [7]. High levels of Mo can interfere with the body’s uptake of Cu, creating copper deficiency by prevents plasma proteins from binding to Cu, and it also increases the amount of Cu that is excreted in urine, so the consumption of high amounts of molybdenum result in the development of symptoms including stunted growth, diarrhea, anemia and achromotrichia (loss of hair stain) [8]. The antagonism between Mo & Cu is affected by the S content of the diet. S reduces the retention of Mo by reducing its absorption from the GIT and increasing its elimination with the feces and the urine [9]. This study was arrangement for understanding Mo and S overload in outcome of Cu deficiency in rat, studying the hematological and histopathological effect of Mo and S alone and in combination overloaded in rats and understanding the mechanism of toxicity due to Mo – Cu – S interaction.
Materials and Methods
Twenty eight (28) adult Albino male rats at weight range of (316-350 g) and age of (4-5 months) were arbitrarily separated into four equal groups (7rat/group), they were kept in optimal condition of raising at the animal house/ college of veterinary medicine. Special pellet diet and water were provided ad libitum for the experiment groups were administered orally for 60 days by using special gavage needle as the following: group (T1) rats of this group were administrated 50 mg/kg B.W of sodium molybdate, group (T2) rats of this group were administrated 500 mg/kg B.W of sodium sulfate, group T3: rats of this group were administrated 25 mg/kg B.W of sodium molybdate + 250mg/ kg B.W of sodium sulfate and group (C) rats of this group were received ordinary distilled water and served as control.
Fasting blood (for 8-12 hrs.) samples were collected at different times 0, 30 and 60 days of the experiment. Blood was drawn by cardiac puncture technique from anesthetized rats [intramuscular injection of Ketamine (90mg/Kg B.W.) and xylazine (40mg/kg B.W.). 1st part of blood samples were collected in tube containing anticoagulant (EDTA), for hematological tests, while the 2nd part of blood were collected in plain tubes and used to separate serum which stored at (-20 Cº), then it used for measurement of biochemical parameters. The blood samples were subjected to assessment of the following parameter by using available commercial kits: RBC count, Hemoglobin concentration and PCV% by using the apparatus of hemolyzer. For histological studies, rats were anesthetized, sacrificed by withdrawal of blood from heart. Immediately, after scarification, the kidney and liver were excised blotted and tissue specimen and preserved in 10% neutral formalin buffer solution till the preparation of histological sections. Several tissue sections were prepared according to Luna G [10].
The Statistical Analysis System as used to effect of different factors (group and day) by using ANOVA-2Ways in study parameters. Least significant difference-LSD test was used to significant compare between means in this study [11].
Results
The result showed higher significant reduction (P > 0.05) in level of RBC count in the treated group T1 dosed with sodium molybdate (50 mg/kg B.W) more than group T2 that dosed with sodium sulfate (500 mg/kg B.W). The least significant reduced levels were recorded in T3 group that given combined half doses of sodium molybdate and sodium sulfate in comparison with control group. All treated groups showed more significant reduction (P > 0.05) at day 60 in comparison with that of day 30 but both showed significant reduction levels than that of pretreatment period (Table 1).
| Group | Day of experiment | LSD value | ||
|---|---|---|---|---|
| 0 | 30 | 60 | ||
| T1 | 8.04 ± 0.16 a A | 6.25 ± 0.20 b B | 4.62 ± 0.16 c C | 0.526 * |
| T2 | 8.41 ± 0.26 a A | 6.61 ± 0.20 b B | ±0.19 c C | 0.651 * |
| T3 | 8.38 ± 0.24 a A | 7.08 ± 0.23 b B | 6.89 ± 0.15 b B | 0.631 * |
| C | 8.50 ± 0.13 a A | 8.41 ± 0.12 a A | 8.61 ± 0.13 a A | 0.397 NS |
| LSD value | 0.603 NS | 0.568 * | 0.472 * | --- |
Table 1: Effect of oral intubation for two months with sodium molybdate, sodium sulfate and their combination on RBC count (×106/
Table 1: Effect of oral intubation for two months with sodium molybdate, sodium sulfate and their combination on RBC count (×106/mm3) of treated adult male rats. C: control group. T1: Animals received sodium molybdate 50 mg/kg/day orally. T2: Animals received sodium sulfate 500 mg/kg/day orally. T3: Animals received 25 mg/ kg B.W + 250mg/kg B.W. of sodium molybdate and sodium sulfate respectively. Different Capital letters denote differences between groups, (P<0.05). Different Small letters denote differences within group, (P< 0.05).
Hemoglobin (Hb) concentration result showed higher significant reduction (P > 0.05) in concentration of Hemoglobin (Hb) in the treated group T1 dosed with sodium molybdate (50 mg/kg B.W) more than group T2 that dosed with sodium sulfate (500 mg/kg B.W). The least significant reduction concentration were recorded in T3 group that had given combined half doses of sodium molybdate and sodium sulfate in comparison with control group.
All treated groups showed more significant reduction (P > 0.05) at day 60 in comparison with that of day 30 but both showed significant reduction levels than that of pretreatment period (Table 2).
| Group | Day of experiment | LSD value | ||
|---|---|---|---|---|
| 0 | 30 | 60 | ||
| T1 | 15.21 ± 0.23 a A | 11.77 ± 0.22 b B | 9.12 ± 0.16 c C | 0.626 * |
| T2 | 14.75 ± 0.22 a A | 11.58 ± 0.22 b B | 9.44 ± 0.23 c C | 0.677 * |
| T3 | 13.91 ± 0.08 a A | 12.67 ± 0.27 b B | 10.94 ± 0.17 c B | 0.578 * |
| C | 14.38 ± 0.25 a A | 14.88 ± 0.31 a A | 14.10 ± 0.17 a A | 0.746 * |
| LSD value | 0.614 * | 0.761 * | 0.552 * | --- |
Table 2: Effect of oral intubation for two months with sodium molybdate, sodium sulfate and their combination on hemoglobin conce
Table 2: Effect of oral intubation for two months with sodium molybdate, sodium sulfate and their combination on hemoglobin concentration (mg/dL) of treated adult male rats. C: control group. T1: Animals received sodium molybdate 50 mg/kg/day orally. T2: Animals received sodium sulfate 500 mg/kg/day orally. T3: Animals received 25 mg/ kg B.W + 250mg/kg B.W. of sodium molybdate and sodium sulfate respectively. Different Capital letters denote differences between groups, (P<0.05). Different Small letters denote differences within group, (P< 0.05).
The result showed higher significant reduction (P > 0.05) in Packed Cell Volume (PCV) % in the treated group T1 dosed with sodium molybdate (50 mg/kg B.W) more than group T2 that dosed with sodium sulfate (500 mg/kg B.W). The least significant reduced levels were recorded in T3 group that given combined half doses of sodium molybdate and sodium sulfate in comparison with control group.
All treated groups showed more significant reduction (P > 0.05) at day 60 in comparison with that of day 30 but both showed significant reduction levels than that of pretreatment period (Table 3).
| Group | Day of experiment | LSD value | ||
|---|---|---|---|---|
| 0 | 30 | 60 | ||
| T1 | 44.25 ± 0.36 a A | 40.22 ± 0.22 b C | 34.81 ± 0.25 c C | 0.856 * |
| T2 | 44.85 ± 0.31 a A | 39.60 ± 0.16 b C | 36.74 ± 0.51 c C | 1.074 * |
| T3 | 43.85 ± 0.31 a A | 42.44 ± 0.17 a B | 40.14 ± 0.34 b B | 0.866 * |
| C | 44.74 ± 0.55 a A | 44.82 ± 0.50 a A | 45.20 ± 0.16 a A | 1.311 NS |
| LSD value | 1.66 NS | 0.877 * | 1.010 * | --- |
Table 3: Effect of oral intubation for two months with sodium molybdate, sodium sulfate and their combination on packed cell volu
Table 3: Effect of oral intubation for two months with sodium molybdate, sodium sulfate and their combination on packed cell volume % of treated adult male rats. C: control group. T1: Animals received sodium molybdate 50 mg/kg/day orally. T2: Animals received sodium sulfate 500 mg/kg/day orally. T3: Animals received 25 mg/ kg B.W + 250mg/kg B.W. of sodium molybdate and sodium sulfate respectively. Different Capital letters denote differences between groups, (P<0.05). Different Small letters denote differences within group, (P< 0.05).
Histopathology
Control Group: There were no significant microscopic findings in the control untreated group used in the experiment. Treated Groups: After two month of treatment:
- Treated Group (1): Liver: Severe dilatation and congestion of hepatic arteries and central veins contain inflammatory cells and serum protein in their lumina. Many sections exhibited extensive areas of necrosis and hemorrhage, the portal areas showed infiltration of mononuclear cells with hyperplasia of bile ductules and moderate hemosiderosis (Figures 1A & 1B).
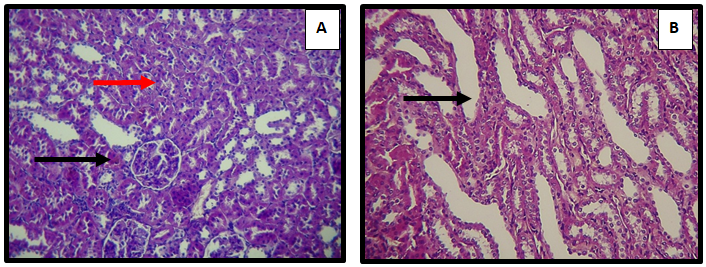
- Kidney: Showed severe congestion of interstitial renal arteries. In addition to marked fibrous thickening of the organ capsule. The fibrous connective tissue was infiltrated with plasma cells and neutrophils, the interstitial tissue showed infiltration of mononuclear cells with mild fibrosis, fibrous thickening of the Bowman’s capsule with cystic dilatation of renal tubules, severe cortical hemosiderosis were also noticed (Figures 2A & 2B).
- Treated Group (2): Liver: The hepatocytes contain large nuclei with more than nucleolus in addition to proliferation of Kupffer cells. Many sections showed focal areas of necrosis, in addition to the formation of suppurative granuloma with the infiltration of inflammatory cells within the portal areas (Figures 3A & 3B).
- Kidney: Histopathological findings were characterized by atrophy of glomerular tufts. In addition to focal interstitial mononuclear cells infiltration with vacuolization of epithelial cells lining the renal tubules. The cortical renal tubules showed cystic dilatation with deposition of hyaline cast (Figure 4A & 4B).
- Treated Group (3): Liver: Tissue section showed mild infiltration of mononuclear cells within the hepatic parenchyma and proliferation of kupffer’s cells. In addition to infiltration of mononuclear cells in the portal area with hyperplasia of bile ductules and severe dilatation of hepatic artery contain inflammatory cells and serum protein in the lumen (Figure 5A & 5B).
- Kidney: The main histopatological changes were acute cellular swelling of proximal and distal convoluted tubules. Other tissue sections showed vacuolar degeneration of epithelial lining the cortical renal tubules with focal areas of regenerated epithelial cells containing large hyperchromatic nuclei with cystic dilatation of medullary renal tubules (Figure 6A & 6B).
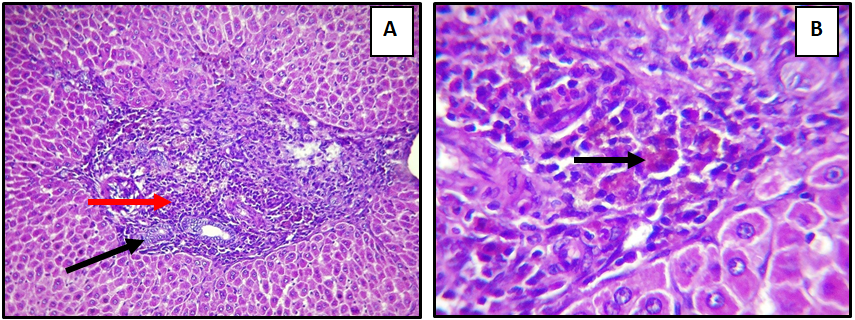
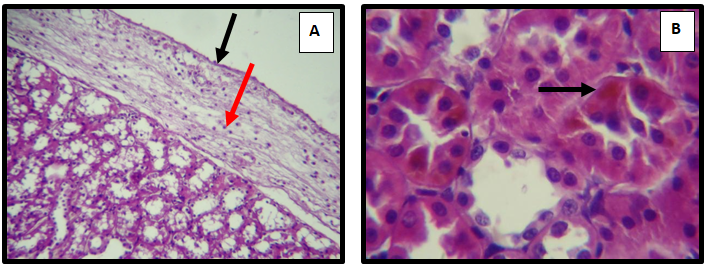
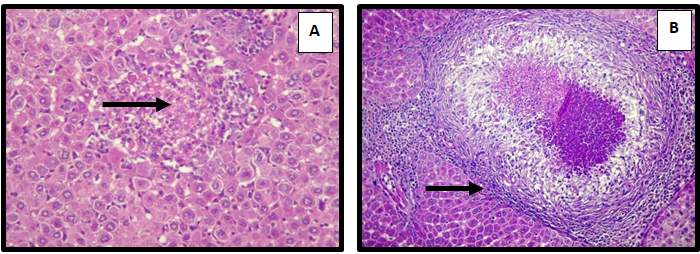
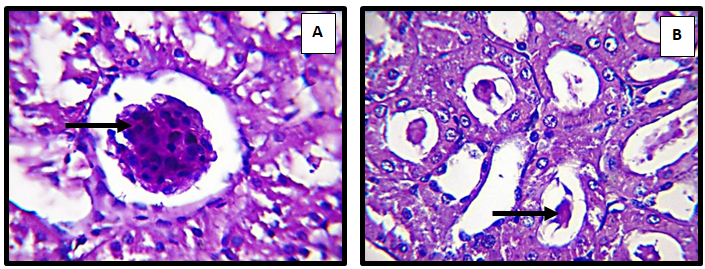
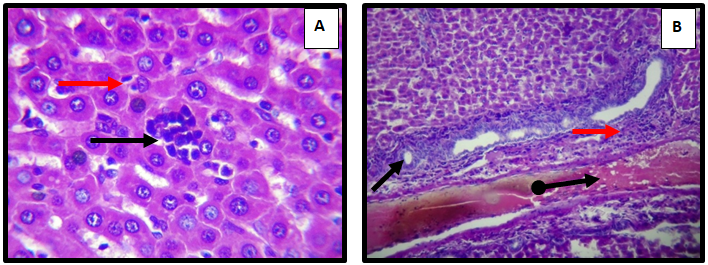
Figure 5: Liver of adult male rat treated with sodium molybdate 50 mg/Kg/B.W and Sodium sulfate500 mg/Kg/B.W (combination) for 60 day, showing (A) mild infiltrate of mononuclear cell within the hepatic paranchyma ( ) and prolifration of kupffer’s cells ( ) in the portal area with hyperplasia of bile ductules ( ) and severe diltation of hepatic artery contain inflammatory cell and serum protien in lumen (
Discussion
The hematologic findings that have been reported in copper deficiency include anemia with neutropenia. The characteristic hematological (blood) effects of copper deficiency are anemia (which may be microcytic, normocytic or macrocytic) and neutropenia [12]. Copper deficiency interferes with iron transport and utilization and, therefore, with heme synthesis. Specifically, ceruloplasmin (which incorporates copper) is a ferroxidase that converts ferrous (+2) to ferric (+3) iron allowing it to bind transferrin and be transported. The copper dependent enzyme cytochrome-c oxidase also is required for the reduction of ferric iron to incorporate it into the heme molecule. In addition to interference with heme synthesis, there is approximately 85% reduction of superoxide dismutase in the RBC membrane in copper deficiency [13]. Copper also acts as a ligand to ferroxidase II, which oxidizes iron, allowing it to be mobilized and transported from hepatic stores to the bone marrow for use in erythropoiesis. Thus, copper deficiency results in excessive iron in the liver but insufficient iron in the marrow for effective erythropoiesis. Patients with copper deficiency can also develop profound hematopoietic deficits resulting in anemia and leukopenia, although not all patients with copper deficiency develop these manifestations. Sideroblastic changes and nuclear maturation defects causing anemia and neutropenia have been observed in erythroid precursors of patients with copper deficiency [14].
Copper-deficient animals lacking adequate levels of cytochrome oxidase are impaired in their ability to synthesize heme from ferric iron [12]. Molybdenum over intake depresses copper availability and produces copper deficiency; the symptoms of molybdenosis are similar to those of hypocuprosis [15].
Our result indicative of different low serum copper levels due to molybdenum, sulphate and their half combined dose, so it is not strong to have a results on the hematological pictures proportional in effect to their copper level in serum and hematopoietic organs, since copper play important role in the synthesis of RBC so its deficiency in different group causing significant reduction in hemoglobin and PCV levels leading to anemia.
Copper deficiency have been reported in many studies due to molybdenum and sulfate overload in rat and ruminant can lead to many hematological manifestations, such as myelodysplasia, anemia, leukopenia (low white blood cell count) and neutropenia (low count of neutrophils, a type of white blood cell that is often called “the first line of defense” for the immune system [16].
Our results showed a decrease in whole hematological activity system including (RBC count, Hb and PCV) which have a major effect on parenchymal and vital tissue and organs such as liver and kidney, RBC count, Hb and PCV decreased in all treated group T1, T2 and T3 but at different extence of change.
Hepatic damage e.g. necrosis and hyperplasia are frequently associated with hematological abnormalities, the degree of damage depending on the severity of an hematological changes, liver damage usually seen and recorded in anemic patients [17]. It has been reported that molybdenum caused hepatocellular necrosis together with severe periportal to bridging fibrosis and biliary hyperplasia. In addition to necrosis, most centrilobular regions have severe hemorrhage, also fibrosis and biliary hyperplasia that bridges portal areas [18].
In rat suchronic exposure to high doses of molybdenum resulted in a delay in body weight gain associated with renal failure marked by a decrease in glomerular filtration. An increase in diuresis and urinary kallikrein excretion associated with unchanged glycosuria and proximal tubular enzymuria (alanine aminopeptidase and gamma-glutamyl transpeptidase) evoked a preferential mild effect at the distal tubules [19]. It has reported that when the levels of serum sulfate increased, they become a common feature of kidney failure, also the levels of serum sulfate may be elevated 7 to 24 times the normal level in an individual with acute renal failure [20]. The hypersulfathemia of chronic renal failure may directly affect the trans-sulfuration pathway and contribute to the severity of homocysteinemia typically seen in this condition [21]. Intratubular hyaline casts were observed in the kidney in addition to the hepatic changes. The acute hepatocellular necrosis, taken with the kidney lesions, suggests acute hemolytic crisis precipitated by molybdenum intoxication [22].
High intake of molybdenum and sulfur in the diet of ruminant causesd a decrease in bioavailability of Cu. Tetrathiomolybdate was identified to complex copper gastro intestinally and in the tissues. A redistribution of Copper from the liver to other tissues occurs. The redistribution to the kidney results in increased urinary Copper execration [23]. Since Cu is involved in normalized function of many enzymes, such as cytochrome c oxidase, which is complex IV in mitochondrial electron transport chain, cerulopasmin, Cu/Zn superoxide dismutase, and in amine oxidases. These enzyme catalyze reactions for oxidative phosphorylation, iron transportation, antioxidant and free radical scavenging and neutralization, and neurotransmitter synthesis, respectively Jaiser SR, et al. [24]. Also, cupper acts as a redox metal (Fenton reactant), so it plays a chief role in inducing ROS and RNS synthesis creating oxidative change especially in parenchymal cells like liver, kidney and spleen. These oxidative changes usually opposed by glutathione interaction to overcome their oxidative changes, those leading to their depletion [25].
So, naturally it can be concluded that damage reported in kidneys and livers of treated groups was proportional with their serum and tissue levels of copper and the oxidative changes induced by them in these organ which more occurred in T1 than T2 while the combination showed less effect probably due to less doses of molybdate and sulphate which causes less copper deficiency and less oxidative changes, or due to similarity of charge (all anion) that effect absorption of Cu depending on the rate of Mo/S in the diet.
References
-
Wuebbens MM, Liu MT, Rajagopalan K, Schindelin H (2000) Insights into molybdenum cofactor deficiency provided by the crystal structure of the molybdenum cofactor biosynthesis protein MoaC. Structure Fold Des 8(7): 709-718.
-
Kaiser BN, Gridley KL, Ngaire Brady J, Phillips T, Tyerman SD (2005) The role of molybdenum in agricultural plant production. Annals of botany 96(5): 745-754.
-
Barceloux DG, Barceloux D (1999) Molybdenum. Journal of Toxicology: Clinical Toxicology 37(2): 231-237.
-
Mendel RR, Bittner F (2006) Cell biology of molybdenum. Biochimica et Biophysica Acta (BBA)-Molecular Cell Research 1763(7): 621-635.
-
Hoffer JL, Hamadeh MJ, Robitaille L, Norwich KH (2005) Human sulfate kinetics. American Journal of Physiology- Regulatory, Integrative and Comparative Physiology 289(5): R1372-R1380.
-
Vest KE, Hashemi HF, Cobine PA (2013) The Copper Metallome in Eukaryotic Cells. Metal Ions in Life Sciences 12: 451-478.
-
Harrison MD, Jones CE, Solioz M, Dameron CT (2000) Intracellular Copper routing: The role of Copper Chaperones. Trend Biochemical Science 25(1): 29-32.
-
NTP (1997) Toxicology and carcinogenesis studies of molybdenum trioxide in F344/N rats and B6C3F1 mice (inhalation studies). Natl Toxicol Program Tech Rep Ser NIH Publication, 462: 1-269.
-
Kodama H, Fujisawa C (2009) Copper metabolism and inherited copper transport disorders: molecular mechanisms, screening, and treatment. Metallomics 1(1): 42-52.
-
Luna LG (1968) Manual of histological staining methods of Armed Forces institutes of pathology. In: 3rd (Edn.), McGraw-Hill, New York, USA.
-
SAS (2012) Statistical Analysis System, User’s Guide. Statistical. In: 9th (Edn.), SAS Inst Inc Cary NC, USA.
-
Gregg XT, Reddy V, Prchal JT (2002) Copper deficiency masquerading as myelodysplastic syndrome. Blood 100(4): 1493-1495.
-
Brewer GJ, Askari F, Dick RB, Sitterly J, Fink JK, et al. (2009) Treatment of Wilson’s disease with Tetrathiomolybdate: V. Control of free copper by Tetrathiomolybdate and a comparison with trientine. Translational Research 154(2): 70-77.
-
Klevay LM (2006) Myelodysplasia, myeloneuropathy, and copper deficiency. Mayo Clinic Proceedings 81(1): 132.
-
Culotta VC, Gitlin JD (2001) Disorders of copper metabolism. In: Scriver CR, Beaudett AI, et al. (Eds), 8th (Edn.), Metabolic and molecular bases of inherited disorders McGraw–Hill, New York, USA, pp: 3105-3126.
-
Turnlund JR, Keyes WR (2006) Dietary molybdenum: effect on copper absorption, excretion, and status in young men. Trace Elements in Man and Animals. Kluwer Academic Press, New York, USA, pp: 951-953.
-
Halfdanarson TR, Kumar N, Li CY, Phyliky RL, Hogan WJ (2008) Hematological manifestations of copper deficiency: a retrospective review. European Journal of Hematology 80(6): 523-531.
-
McHutchison JG, Manns MP, Longo DL (2006) Definition and management of anemia in patients infected with hepatitis C virus. Liver Int 26(4): 389-398.
-
Pandey G, Jain GC, Mathur N (2012) The effect of sub chronic exposure to ammonium molybdate on hematological and hepatic parameters in albino rats. Asian J Phar Biol Res 2(2): 136-142.
-
Murray J, Sullican F, Tiwary A, Carey S (2013) 90-Day subchronic toxicity study of sodium molybdate dihydrate in rats. Regul Toxicol Pharmacology 70(3): 579-588.
-
Culotta VC, Gitlin JD (2000) Disorders of copper transport. The Metabolic and Molecular Bases of Inherited Disease, OMMBID, McGraw Hill, New York, USA, pp: 3105-3126.
-
Nakanishi T, Otaki Y, Hasuike Y, Nanami M, Itahana R, et al. (2002) Association of hyperhomocysteinemia with plasma sulfate and urine sulfate excretion in patients with progressive renal disease. Am J Kidney Dis 40(5): 909-915.
-
Hansen SL, Schlegel P, Legleiter LR, KLloyd KE, Spears JW (2008) Bioavailability of copper from copper glycinate in steers fed high dietary sulfur and molybdenum. J Anim Science 86(1): 173-179.
-
Jaiser SR, Winston GP (2010) Copper deficiency myelopathy. Journal of Neurology 257(6): 869-881.
-
Fang YZ, Sheng Y, Guoyao Wu (2002) Free radicals, antioxidants, and nutrition. Nutrition 18(10): 872-879.