Central Nervous System Infiltration by Multiple Myeloma: Two Case Reports of a Rare Clinical Presentation
Introduction: We present two case reports of rare and aggressive presentation of multiple myeloma, one of the most common hematological malignancies. To our knowledge, there are very few case reports of meningeal invasion by multiple myeloma, denoting the importance of describing the clinical features and the complementary investigation necessary to develop a better approach to these patients. Cases presentation: In case 1, we present a 64 years old patient with vague symptoms of headache associated with exacerbated tendinous reflexes and previous diagnosis of multiple myeloma. In case 2, a 58 years old presents with auricular plenitude, headache and encephalopathy, and a medical antecedent of multiple myeloma. Both were diagnosed with different sites of multiple myeloma central nervous system invasion, case 1 with predominant meningeal infiltration and case 2 with intraparenchymal infiltration. Conclusion: Analyzing these cases, we conclude that besides the rarity of the meningeal accometiment in myeloma patients compared to other hematological disorders, the identification of clinical signals and symptoms suggestive of this invasion is necessary to provide better health care to these patients.
Introduction
Multiple myeloma is one of the most common hematological malignancy worldwide. It is formed by abnormal plasma cells usually producing monoclonal antibodies of different subtypes that accumulate on bone marrow and multiple parts of the body, causing many different clinical abnormalities [1].
Multiple myeloma may affect the central and peripheral nervous system, causing different neurological symptoms. These complaints may be secondary to different mechanisms like compression, monoclonal antibodies, or collateral effects of the therapy, for example [1, 2].
Leptomeningeal myeloma is a rare entity and correlationates with aggressive disease and poor prognosis, affecting a minority of the patients with multiple myeloma [2]. A high clinical suspicion of this rare entity is required to offer a better quality of life to the patients, because it usually presents with a wide constellation of nonspecific clinical symptoms.
In our case report, we present two cases of multiple myeloma infiltration of the central nervous system presenting with vague clinical symptoms, illustrating the need of minucius investigation of these patients.
Case Report
Case 1
A 64 years old patient presented to the emergency department complaining of holocranial headache, unsteady gait, drowsiness and subtle cognitive impairment. She had a diagnosis of multiple myeloma and four years before, she had already been submitted to an autologous stem cell transplantation, with good therapeutic response and no signal of active disease until the date. At the neurological examination she had lost of proximal muscle strength associated with exacerbation of all tendinous reflexes.
An MRI of the brain and spine was requested, which showed leptomeningeal and ependymal, supra and infratentorial lesions with involvement of cranial nerves (subclinical at the moment) and parenchymal micronodular lesions (Figure 1). There were also lesions in the cranial portion of the spinal cord, at the cervical level, associated with diffuse leptomeningeal impregnation, affecting the cervical, thoracic and lumbar regions and the cauda equina roots. The lumbar puncture after the radiological evaluation showed monoclonal plasmocytes with 123 proteins/dL.
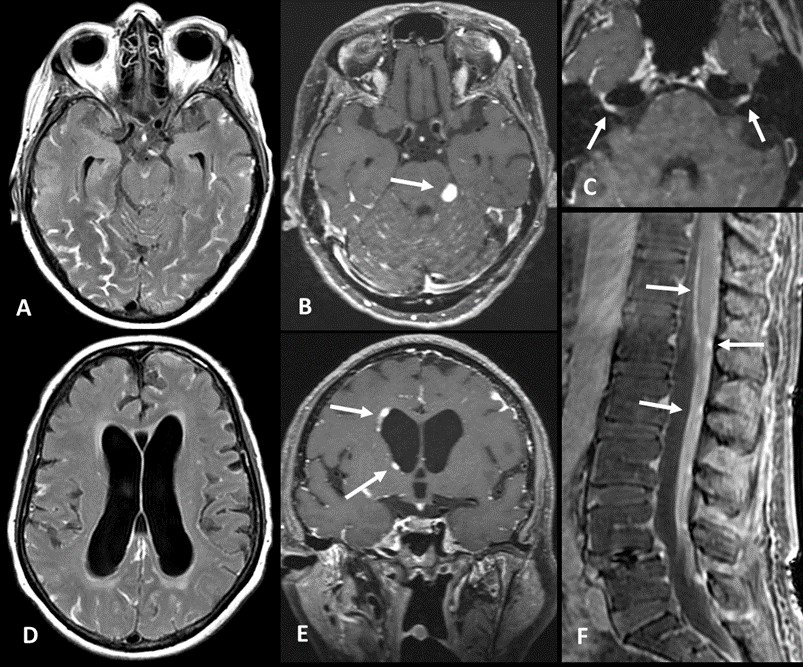
Figure 1: (A) Axial gadolinium-enhanced FLAIR sequence and (B) Axial gadolinium-enhanced T1-SPACE sequence showing diffuse leptomeningeal enhancement in interpeduncular cistern, temporal and occipital lobes, superior aspect of both cerebellar hemispheres. Nodular leptomeningeal enhancement in left ambiens cistern (arrow). (C) Axial gadolinium-enhanced T1-SPACE sequence demonstrates enhancement of complex of seventh and eighth cranial nerves within the internal auditory canals. (D) Axial FLAIR – moderate hydrocephalus with transependymal edema. (E) Coronal gadolinium-enhanced T1-SPACE sequence showing subependymal nodular enhancement (arrow). (F) Sagittal gadolinium-enhanced fat-suppressed T1 sequence of lumbar spine – linear pial and nodular leptomeningeal enhancement in pial surface of conus medullaris and cauda equina roots (arrow).
Rescue chemotherapy was attempted, with no good therapeutic response. After that, she was submitted to palliative care, with great improvement of life quality and pain. She died 5 months after the recurrence.
Case 2
A 58-year-old female patient presented to neurological evaluation compaimpling of progressive vertigo, tinnitus, ear plenitude and episodic holocranial headache that worsened in a week. She also developed an episodic holocranial headache. Her previous medical history included the diagnosis of multiple myeloma (subtype IgA - DS IIIA/ ISS 2) 4 years before with previous autologous bone marrow transplant with great therapeutic response, showing criteria of remission on the transplant follow up until one year before the neurological symptoms, when she developed continuous and diffuse bone pain. On her neurological examination, she had partial desorientation on time and space, without any other alterations on motor and sensibility. To elucidate the cognitive and headache symptoms, we choose magnetic resonance imaging.
Brain magnetic resonance imaging had lytic lesions on parietal bones with intense gadolinium uptake associated with invasion and thickening of the falx cerebri. There was significant leptomeningeal thickening and enhancement of the cortical gyri and the left sylvian fissure in the temporal lobe, with associated vasogenic edema (Figure 2). The lesion spectroscopy showed an important choline peak (inferring greater cell turnover) and a reduction in the N-Acetyl Aspartate peak (neuronal density and viability marker), inferring invasion of the central nervous system by the underlying disease. A lumbar puncture was made and the initial cerebrospinal fluid analysis had 27 cells, 100% with neoplasic features.
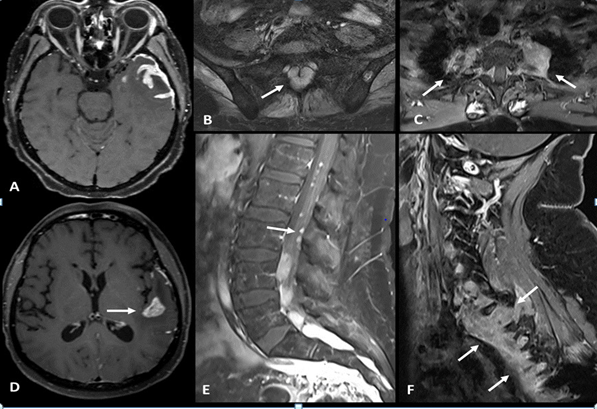
Figure 2: (A, D) Axial gadolinium enhanced T1-SPACE sequence showing leptomeningeal and brain parenchymal enhancement in left temporal lobe. (B) Axial gadolinium-enhanced fat-suppressed T1 sequence of sacrum showing extradural mass lesion within sacral foramina (arrow). (E) Sagittal gadolinium-enhanced fat-suppressed T1 sequence demonstrates nodular enhancement of cauda equina roots (arrow). Axial (C) and Sagittal (F) gadolinium-enhanced fat-suppressed T1 sequence of cervical spine showing paravertebral mass lesion in superior thoracic spine and inferior cervical spine with foraminal and extradural space involvement.
Rescue chemotherapy was performed with therapeutic failure and the patient died 5 months after diagnosis of central nervous system infiltration.
Discussion
Multiple myeloma is a hematological disorder caused by abnormal plasmocyte clones usually with production of monoclonal antibodies (M protein) on urine or blood samples [3]. The disease can cause some neurological symptoms secondary to peripheral nervous system disease, amyloidosis and spinal cord accometiment, for example. However, while some oncological diseases more commonly present with brain metastasis or leptomeningeal invasion, these are rare on multiple myeloma patients, with few case reports on literature until the present date [1, 2].
Leptomeningeal myelomatosis is rare and denotes a poor prognosis [2, 4]. It is associated with a disease’s very aggressive biological behavior. The incidence of meningeal accometiment on multiple myeloma patients is around 1%. A case series suggests that involvement of upper cranial nerves, encephalopathy, and symptoms of myelopathy are the most common suggestive signs of central nervous system accometiment [5].
Varga et al, described a case series of 13 patients with multiple myeloma and central nervous system relapse. They were younger than our patients and presented more with IgA and Light chain secretory profile, and some of them presented as primary plasma cell leukemia. Their dominant symptoms were cranial nerve palsies, while symptomatic cranial nerve palsies were not observed in our patients [6].
Multiple myeloma usually invades the central nervous system by hematogenous dissemination and/or contiguous spread of the tumor. Some mutations of tumor suppressor genes, oncogenes and altered expression of adhesion molecules may predispose these patients to have central nervous system metastasis [7].
Invasion of the central nervous system by multiple myeloma denotes a poor prognosis, with some studies demonstrating an average survival of 2 months, similar to the patients presented in this case [2].
Conclusion
The description of the two cases shows us rare, however severe, presentations of multiple myeloma. Knowledge of such manifestations and detailed investigation using complementary methods in these patients allows for an accurate diagnosis and better follow-up for such patients.
References
-
Kumar S, Rajkumar V, Kyle R, Duin M van, Sonneveld P, et al. (2017) Multiple Myeloma. Nat Rev Dis Primers 3: 17046.
-
Velasco R, Bruna J (2012) Neurologic Complications of Multiple Myeloma and Plasmacytoma. Eur Assoc NeuroOncol Mag 2: 71-77.
-
International Myeloma Working Group (2003) Criteria for the Classification of Monoclonal Gammopathies, Multiple Myeloma and Related Disorders: A Report of the International Myeloma Working Group. Br J Haematol 121: 749-757.
-
Velasco R, Petit J, Llatjós R, Juan A, Bruna J (2010) Can Leptomeningeal Myelomatosis Be Predicted in Patients with Igd Multiple Myeloma? J Clin Neurosci 17(8): 1071- 1072.
-
Chamberlain MC, Glantz M (2008) Myelomatous Meningitis. Cancer 112(7): 1562-1567.
-
Varga G, Mikala G, Gopcsa L, Csukly Z, Kollai S, et al. (2018) Multiple Myeloma of the Central Nervous System: 13 Cases and Review of the Literature. J Oncol 23: 3970169.
-
Nieuwenhuizen L, Biesma DH (2008) Central Nervous System Myelomatosis: Review of the Literature. Eur J Haematol 80(1): 1-9.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study