The Effect of RBD-Based Vaccines on Covid-19 XBB 1.5 Subvariant
COVID-19 (Coronavirus disease 2019 or severe acute respiratory syndrome coronavirus 2) is a transmissible illness affected by a virus of the Coronaviridae family. Omicron is one of the COVID-19 variants of SARS-CoV-2 that firstly informed from Botswana B.1.1.529 was the original subvariant of omicron and then numerous sub-variants of Omicron have appeared comprising: BA.1, BA.2, BA.3, BA.4, and BA.5, BQ.1 and BQ.1.1, XBB.1, and XBB 1.5. The aim of this in silico research is to investigate the effect of monovalent (monovalent) vaccines on the XBB.1.5 variant. In this in silico study the sequence of spike protein obtained from NCBI and then the mutations of XBB 1.5 were add to obtained sequence. Since most of the currently used vaccines belong to the RBD region, in this study the RBD mutations were analyzed. All B cell and T cell epitopes of original strain (Wuhan) recorded and the epitopes that changed via mutation (XBB 1.5) were removed. The original virus has 10 B-cell epitopes in the RBD region. 5 of these epitopes were not mutated (unchanged. Besides the B cells epitopes, 45 alleles of T cell epitopes were also unchanged. The result of this study informed that the monovalent vaccine can produce humoral and especially cellular immunity and the vaccines help protect against severe illness, hospitalization, and death. The mutations will certainly reduce the effectiveness of monovalent vaccine, so the use of bivalent vaccines is recommended. Some countries do not have bivalent vaccines; these countries can still use monovalent vaccines.
Introduction
COVID-19 (Coronavirus disease 2019 or severe acute respiratory syndrome coronavirus 2) is a transmissible illness affected by a virus of the Coronaviridae family. The virus was first reported from Wuhan, China, in December 2019 [1], and then spread to other countries. The Coronavirus disease 2019 symptoms comprise headache, loss of smell, fever, fatigue, cough, and loss of taste and breathing [2, 3].
Omicron is one of the COVID-19 variants of SARS- CoV-2 that firstly informed from Botswana B.1.1.529 was the original subvariant of omicron and then numerous sub- variants of Omicron have appeared comprising: BA.1, BA.2, BA.3, BA.4, and BA.5 [4]. In October 2022, two sub-variants of BA.5 called BQ.1 and BQ.1.1 have reported [5]. Towards the end of 2022 XBB.1.5, which is grown from the XBB sub- variant has emerged. By the end of 2022, 40.5% of new cases of US have been infected by XBB [6].
The spike protein of the Omicron is characterized by at least 34 mutations (30 amino acid substitutions, three deletions, and one amino acid insertion). Remarkably, 15 aa substitutions are in the RBD (Receptor Binding Domain). The RBD amino acid substitutions are following as: G339D, S371L, S373P, S375F, K417N, N440K, G446S, S477N, T478K, E484A, Q493R, G496S, Q498R, N501Y and Y505H. XBB.1 is a subvariant of omicron, through two other Spike protein mutations (N460K, F490S) and XBB.1.5 is a subvariant of XBB, with an extra Receptor Binding Domain mutation S486P. The XBB.1.5 subvariant was detected in the US on October 2022. The variant has also been detected in the EU and Asia [7]. As of 11 January 2023, more than 669 million people have been infected, with about 6.7 million deaths. Different vaccines have been used throughout the pandemic and several research studies are proceeding to recognize potential antivirals or different drugs to treat COVID-19 patients [8].
COVID-19 vaccination supports protecting people
by producing antibody responses without you having to experience potentially severe disease or post-COVID conditions. Getting sick with COVID-19 can cause severe illness or death [9]. There are a small number of updated vaccines in the world. For example a booster dose of Omicron BA- 4 / BA- 5 the bivalent vaccine has been approved for emergency use via USA Food and Drug Administration (FDA) (pfizer.com, 2023). Zou, et al. reported that the bivalent BA.4/5 vaccine is more immunogenic than the original BNT162b2 monovalent vaccine against circulating Omicron subvariants (BA.4/5, BA.4.6, BA.2.75.2, BQ.1.1, and XBB.1) [10]. Whereas xbb 1.5 is the most transmissible variant, but there is no published research on the effect of monovalent (non-updated) vaccines on XBB. 1.5 Variant. The aim of this in silico research is to investigate the effect of monovalent (non-updated) vaccines on the XBB.1.5 variant.
Material and Methods
This study aimed to investigate the XBB 1.5 mutations by Bioinformatic analysis. In this in silico study the sequence of spike protein obtained from NCBI (NCBI Reference Sequence: YP_009724390.1) and then the mutations of XBB 1.5 were add to obtained sequence (Figure 1).

Most vaccines (Pfizer, Moderna, Sputnik V, Novavax, Astrazeneca, Soberana, Spikogen, Cov Pars, Noora and etc) are designed by targeting the RBD region. For this reason the B and T cell epitopes of original virus (Wuhan) which are obtained and mutated epitopes are evaluated (Figure 2).

B-cell epitopes were acquired by Immune Epitope Database server (IEDB) [11, 12]. We used PropredI for prediction of MHC class I epitopes. In this research the epitopes were evaluated for their binding affinity with all HLA alleles (p values <0.05 were considered significant) [13, 14]. After that the epitopes changed as a result of the mutation and the epitopes that were not affected by the mutation were recorded and then compared.
Result and Discussion
Since most of the currently used vaccines belong to the RBD region, in this study the RBD mutations were analyzed. The spike protein sequence of severe acute respiratory syndrome coronavirus-2 was obtained from National Center for Biotechnology Information (NCBI). The B cell epitopes (predicted by IEDB) having a score higher than
0.35 were selected and PropredI was used for prediction of MHCI epitopes. All B cell and T cell epitopes of original strain (Wuhan) recorded and the epitopes that changed via mutation (XBB 1.5) were removed.
The original virus has 10 B-cell epitopes in the RBD region. 5 of these epitopes were not mutated (unchanged). The unchanged epitopes are shown in Figure 3.
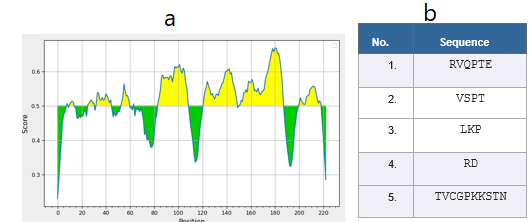
Besides the b cells epitopes, 45 alleles of T cell epitopes were also unchanged (Table 1).
| Epitope | Allele |
|---|---|
| VLSFELLHA | HLA-A*0201 |
| VVVLSFELL | HLA-A*0205 |
| KCYGVSPTK | HLA-A*1101 |
| CYGVSPTKL | HLA-A24 |
| VYAWNRKRI | |
| RVVVLSFEL | |
| KCYGVSPTK | HLA-A3 |
| QIAPGQTGK | |
| VQPTESIVR | HLA-A*3101 |
| VYADSFVIR | |
| SVYAWNRKR | HLA-A*3302 |
| VYADSFVIR | |
| SVYAWNRKR | HLA-A68.1 |
| ASVYAWNRK | |
| RKRISNCVA | HLA-A20 |
| FKCYGVSPT | |
| ELLHAPATV | HLA-A2.1 |
| VRFPNITNL | HLA-B14 |
| ESIVRFPNI | |
| VRFPNITNL | HLA-B*2702 |
| VRFPNITNL | HLA-B*2705 |
| NRKRISNCV | |
| QPTESIVRF | HLA-B*3501 |
| GPKKSTNLV | |
| FERDISTEI | HLA-B*3701 |
| NDLCFTNVY | |
| QPTESIVRF | HLA-B*3801 |
| CYGVSPTKL | |
| VRFPNITNL | HLA-B*3901 |
| RVVVLSFEL | HLA-B*3902 |
| DDFTGCVIA | HLA-B40 |
| FELLHAPAT | |
| NDLCFTNVY | HLA-B*4403 |
| IAPGQTGKI | HLA-B*4403 |
| LPDDFTGCV | |
| GPKKSTNLV | |
| IAPGQTGKI | HLA-B*5101 |
| LPDDFTGCV | |
| GPKKSTNLV | |
| IAPGQTGKI | HLA-B*5102 |
| GPKKSTNLV | |
| IAPGQTGKI | HLA-B*5103 |
| LPDDFTGCV | |
| NVYADSFVI | HLA-B*5201 |
| LPDDFTGCV | HLA-B*5301 |
| FPNITNLCP | |
| FPNITNLCP | HLA-B*5401 |
| LPDDFTGCV | HLA-B*51 |
| FPNITNLCP | |
| FTNVYADSF | HLA-B*5801 |
| QPTESIVRF | |
| FERDISTEI | HLA-B60 |
| FERDISTEI | HLA-B61 |
| FELLHAPAT | |
| DDFTGCVIA | |
| GQTGKIADY | HLA-B62 |
| RISNCVADY | |
| RVVVLSFEL | HLA-B7 |
| VVVLSFELL | |
| APGQTGKIA | |
| RKRISNCVA | HLA-B*0702 |
| GPKKSTNLV | |
| KPFERDIST | |
| WNRKRISNC | HLA-B8 |
| VSPTKLNDL | |
| GPKKSTNLV | |
| ESIVRFPNI | |
| VVVLSFELL | HLA-Cw*0301 |
| VRFPNITNL | |
| CYGVSPTKL | HLA-Cw*0401 |
| QPTESIVRF | |
| VSPTKLNDL | HLA-Cw*0602 |
| RVVVLSFEL | |
| VRFPNITNL | |
| NDLCFTNVY | HLA-Cw*0702 |
| VRFPNITNL | MHC-Db |
| VYAWNRKRI | |
| VVVLSFELL | MHC-Db |
| CGPKKSTNL | MHC-Dd |
| VSPTKLNDL | |
| CYGVSPTKL | MHC-Kd |
| VYAWNRKRI | |
| FERDISTEI | MHC-Kk |
| TESIVRFPN | |
| FELLHAPAT | |
| ESIVRFPNI | |
| QPTESIVRF | MHC-Ld |
| VSPTKLNDL |
Table 1: The amino acid sequence of T cell (MHC I) epitopes.
Since most monovalent vaccines target the Receptor Binding Domain (RBD) of the spike protein of COVID-19, in this in silico study, the RBD mutations of XBB 1.5 has been investigated. The results acquired from the IEDB indicated that there are a minimum of five highest score B cell epitopes that remained unchanged. The PropredI analysis indicated that there are still 45 unchanged and common epitopes (for different MHCI) between the original variant (Wuhan) and XBB 1.5.
XBB.1.5 is a subvariant of the XBB, and is currently expected to have a large growth advantage over previously circulating variant in the world, even though these estimates are related with important uncertainty. There is a risk that this variant may have an increasing effect on the number of COVID-19 cases in the world. The result of this study informed that the monovalent vaccine can produce humoral and especially cellular immunity and the vaccines help protect against severe illness, hospitalization, and death. The mutations will certainly reduce the effectiveness of monovalent vaccine, so the use of bivalent vaccines is recommended. Some countries do not have bivalent vaccines; these countries can still use monovalent vaccines.
References
-
Page J, Hinshaw D, McKay B (2021) In Hunt for Covid-19 Origin, Patient Zero Points to Second Wuhan Market- The Man with the First Confirmed Infection of the New Coronavirus Told the WHO Team that His Parents had shopped there. The Wall Street Journal.
-
Islam MA, Kundu S, Alam SS, Hossan T, Kamal MA, et al. (2021) Prevalence and Characteristics of Fever in Adult and Paediatric Patients with Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of 17515 Patients. PLOS ONE 16(4): e0249788.
-
Saniasiaya J, Islam MA, Abdullah B (2021) Prevalence of Olfactory Dysfunction in Coronavirus Disease 2019 (COVID-19): A Meta-analysis of 27,492 Patients. Laryngoscope 131(4): 865-878.
-
Vitiello A, Ferrara F, Auti AM, Di Domenico M, Boccellino M (2022) Advances in the Omicron Variant Development. J Intern Med 292(1): 81-90.
-
Yao L, Zhu KL, Jiang XL, Wang XJ, Zhan BD, et al. (2022) Omicron Subvariants Escape Antibodies Elicited by Vaccination and BA.2.2 Infection. Lancet Infect Dis 22(8): 1116-1117.
-
Russell P (2023) Omicron XBB.1.5: What Do We Know So Far? Medsacape UK.
-
European Centre for Disease Prevention and Control (ECDC) (2023) Update on SARS-CoV-2 Variants: ECDC Assessment of the XBB.1.5 sub-lineage.
-
WorldOmeter (2023) COVID-19 Coronavirus Pandemic.
-
Centers for Disease Control and Prevention (CDC) (2023) Stay Up to Date with COVID-19 Vaccines Including Boosters.
-
Zou J, Kurhade C, Patel S, Kitchin N, Tompkins K, et al. (2023) Improved Neutralization of Omicron BA.4/5, BA.4.6, BA.2.75.2, BQ.1.1, and XBB.1 with Bivalent BA.4/5 Vaccine. BioRxiv Preprint.
-
Tazehkand MN, Hajipour O (2020) In silico Recombinant Vaccine Candidate against Coronavirus (2019-nCoV). Acta Scientific Microbiology 3(4): 17-23.
-
Tazehkand MN, Hajipour O (2020) Evaluating the Vaccine Potential of a Tetravalent Fusion Protein against Coronavirus (COVID-19). J Vaccines Vaccin 11(2): 412.
-
Tazehkand MN, Hajipour O (2019) In Silico Design A Vaccine Candidate against _Corynebacterium Diphtheriae_. International Journal of Molecular and Clinical Microbiology 9(1): 1082-1089.
-
Tazehkand MN, Hajipour O (2019) Multi Epitope Vaccine Candidate against Mycobacterium Tuberculosis. Drug Designing & Intellectual Properties International Journal 3(2): 351-358.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study