Evaluation of Scapular Dyskinesia in Checkout Operators and Its Association with Data Related to Work or Musculoskeletal Pain
The scapulothoracic joint has an essential function for the correct biomechanics of the shoulder. When the scapula has movements or abnormal positioning, the condition is called scapular dyskinesia, such dysfunction infers shoulder pain. Shoulder pain is one of the main complaints and reason for removal of checkout operators. Objective: To evaluate scapular dyskinesia in checkout operators, and its association with work-related data or musculoskeletal pain. Methodology: A cross-sectional descriptive research was carried out with 32 checkout operators. The ergonomic condition of the furniture was evaluated using the Couto Checklist and tests were performed to detect scapular dyskinesia as described by McClure. Conclusion: No significant results were found for the association of shoulder pain and scapular dyskinesia. There was an association of neck pain with scapular dyskinesia of the left upper limb in checkout operators.
Introduction
The shoulder complex is characterized by an extensive range of motion, however, it is constantly affected by pain and injury. Consequently, it is understood that it is the most mobile and least stable joint due to its anatomy, especially the glenohumeral joint [1].
To ensure stabilization and mobility, it is necessary to work in harmony, constant synchrony between static and dynamic structures that promote adequate kinematics [1].
For the functioning of the shoulder joint, several muscles act, with a joint action of the rotator cuff, promoting displacements and acting in an important way as a joint stabilizer. Injury to any tendon of the rotator cuff can determine a condition of pain, instability, and may also cause other symptoms. Therefore, the perfect functionality of these muscles is necessary for correct kinematics [2].
The movements that occur in the scapula and rib cage are the result of the cooperation of the acromioclavicular and sternoclavicular joints. When restriction occurs, changes in mobility and position are associated with imbalance, weakness, resulting in scapulohumeral rhythm leading to scapular dyskinesia [3].
Individuals with changes in shoulder girdle mobility often report shoulder pain. Especially those who perform elevation of the limb above 90º in abduction and flexion, repetitive activity of the upper limb, generating an impact on the tissues, possibly causing muscle fatigue, with an alteration in the scapulohumeral rhythm [3].
The scapulohumeral rhythm is the synergy between the scapular and humeral movements, which must occur in a coordinated manner, allowing a greater range of motion in the shoulder complex in relation to if the scapula were fixed. When the arm is raised, abducted or flexed, the scapula rotates, contributing to the total humeral range of motion [4].
As it occurs at 30° of humeral elevation, the scapula contributes about one-fifth of the glenohumeral joint. When elevating above 30º, the scapula rotates or rotates about 1º to 2º of movement of the humerus [4].
Changes in scapular biomechanics can cause muscle overload, restriction in strength, range of motion and pain in the shoulder joint. Therefore, the deformations that occur in the movement of the shoulder girdle have been correlated both in terms of pain and shoulder injuries, such as instability, tendonitis of the rotator cuff muscles and impingement syndrome [3].
It is reported that pain is frequently affected in individuals who operate with the upper limb in repetitive work that requires overload on the shoulder. Especially those above 90 degrees of abduction and/or flexion, which may interfere with the performance of their activity [3].
There are factors that have been leading to the association between shoulder pain and scapular dyskinesia, but there are not enough studies that prove scapulothoracic rhythm alteration as a contributor to risk and follow-up evidence [5].
Scapular dyskinesia is the term used when the scapula does not develop its stabilization work, that is, there is a biomechanical alteration of the scapula during movement or rest as a result of dysfunction, contracture or weakness of the stabilizers [6].
Ergonomics is a study that is characterized by the relationship between the institution/component and the man, through norms, principle, concept, aiming at comfort, safety, effectiveness, satisfaction for better productivity [7].
Given the above, this study aimed to evaluate scapular dyskinesia in checkout operators, and its association with data related to work or musculoskeletal pain.
Methodology
This is a cross-sectional analytical research. It was carried out after the opinion of the Research Ethics Committee nº
2,372,235. The study was carried out in 1 supermarket chain in the interior of Goiás.
Thirty-two female individuals aged between 18 and 45 years, with no associated pathologies, were evaluated. Female checkout operators who work at the company where the present study was carried out were included. Those with lower limb discrepancy were excluded; who work in more than one service; operator who presents rheumatic and neurological pathologies; those with less than 6 months in the job; physically handicapped; operators who have a history of fracture of the humerus, scapula and clavicle, those operators who have a history of dislocation of the upper limb joints within a period of 6 months.
Data collection was performed using sociodemographic questionnaires, Couto’s checklist and scapula evaluation using the scapular dyskinesia test, as in the study by McClure, et al.
The first step consisted of the authorization of the supermarket to carry out the observation, and the collection of questionnaires, which were applied to the checkout operators. The work to be carried out in the company was explained, followed by the delivery of the free and informed consent form (TCLE), the volunteers were informed of the research procedures and objectives.
After agreeing to participate in the research, the volunteer signed the TCLE, completed the evaluation form (personal data, inclusion and exclusion criteria) and answered the questionnaire and applied the scapular dyskinesia test by McClure, et al.
The sociodemographic questionnaire consisted of 21 questions, including age; sex; length of service in the activity; instruction level; height; Weight; work shift; previous practice as a cashier; the position you prefer to work; when changing the place of work, adjust the seat; feels pain while working; pains are caused by work; where is the pain; checkout could be more comfortable; feels shoulder pain; there is presence of scapular dyskinesia; classification of scapular dyskinesia; presented lower limb discrepancy; presents rheumatic or neurological pathology; presents or has already presented dislocation of the joints of the upper limb.
An evaluation of the workstation was carried out using Couto’s checklist, with the objective of verifying the furniture and work environment where the operator works. Through the questionnaires, an attempt is made to obtain quantitative information about the real situations in which the checkout operators carry out their activity, based on the interpretation criteria of Couto’s checklist.
In the items surveyed, and for the total number of items in this checklist, it was considered: Excellent ergonomic condition 91 to 100% of the points, good ergonomic condition 71 to 91% of the points, reasonable ergonomic condition 51 to 70% of the points, ergonomic condition bad 31 to 50% of the points and poor ergonomic condition less than 31% of the points.
In order to carry out this work, evaluation instruments were used, such as a female top, a flexicurve ruler, 1kg and 2kg dumbbells, white adhesive tape for the markings of the scapular dyskinesia test and a questionnaire, in order to collect data for the work. To verify scapular dyskinesia, white adhesive tape was used for the demarcations, 1 kg dumbbells for those operators with body weight up to 65 kg, and 2 kg for those with body weight above 65.1 kg, the type of dyskinesia was visually analyzed scapular.
The scapular dyskinesis test was performed with the patient in an orthostatic position, the upper limbs positioned around 35º anteriorly in the frontal plane, between flexion and abduction, requesting the abduction movement eight times, using load on both arms.
The evaluator positioned himself behind the patient and evaluated during the movement the symmetry of the scapular movement, as well as whether there was prominence of the inferior angle of the scapula, prominence of the inferior angle of the scapula and medial border, prominence of the inferior angle of the scapula the spine of the scapula.
A postural assessment was carried out with the aim of assessing thoracic kyphosis using a flexible ruler, called the flexicurve, used to assess spinal curvatures in the sagittal plane. The checkout operator positioned himself in an orthostatic position, barefoot, with a 90º flexion of the shoulders and elbows to prevent the upper limbs from overlapping the image of the thoracic spine.
Locating and marking the spinous processes from C7 to T12, the flexible ruler is initially positioned on the spinous process of C7, modeling the shape of the kyphotic curvature up to the spinous process of T12.
The phase of transcribing the format of the dorsal column to graph paper as soon as it was removed from the checkout operator, maintaining the format, was placed on the graph paper and the column was drawn as it was molded on the ruler on the side where it was resting on the volunteer’s back evaluating and demarcating points from C7 to T12.
After transferring to the graph paper, a straight line was drawn connecting the point of C7 to that of T12, another perpendicular line to the straight line made between the points of C7-T12, connecting the point of greater distance than the curve in relation to the straight line between C7 - T12.
The distances were demarcated as follows: The height (B) as the greatest distance from the curvature to the line joining the points of C7–T12. The average Xmeio is the distance between the point of T12 and the point of B, B being the one that touches the straight line that joins C7 and T12. The total measure is the distance of the straight line that joins C7 to T12.
To determine the thoracic kyphosis of the checkout operator through the flexicurve, a 60 cm trident flexible ruler was used, a ruler for demarcating the points on graph paper, adhesive tape, graph paper, pen and pencil, specific software made in Microsoft Excel base to calculate the thoracic kyphosis angle in degrees from a specific mathematical formula, described below:
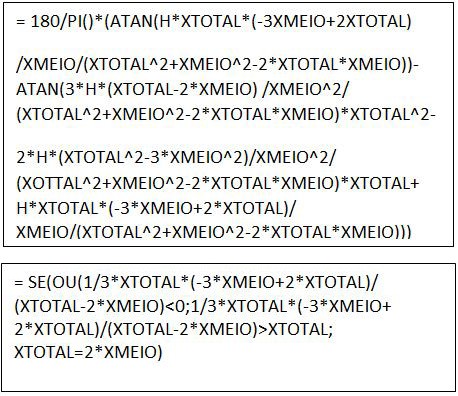
To confirm the correct data, use:
For statistical analysis, the SPSS 22.0 program was used. Descriptive statistics were performed with presentation of the mean and standard deviation of continuous data and relative and absolute frequency of nominal data, in addition, the chi-square test was performed in order to verify associations between variables. P values lower than 0.05 were considered significant.
Results
They were found in the 32 checkout operators at their respective workstations.
| Variable | Average | Standard deviation |
|---|---|---|
| Age | 30.4 | 7.73 |
| Service time | 1.96 | 0.89 |
| Height | 158.93 | 6.38 |
| Weight | 64.15 | 16.32 |
| kyphosis | 33.41 | 10.82 |
Table 1: Mean and standard deviation of age, length of service, height, weight and kyphosis.
| Characteristics | Number | Percentage (%) |
|---|---|---|
| Instruction Level | ||
| 1st degree | 3 | 9.4 |
| 2nd degree | 25 | 78.1 |
| 3rd degree | 4 | 12.5 |
| Work Shift | ||
| 1st shift | 16 | 50 |
| 2nd shift | 16 | 50 |
| Have Another Job | ||
| Yes | 0 | 0 |
| No | 32 | 100 |
| Previous Practice in the Role | ||
| Yes | 19 | 59.4 |
| No | 13 | 40.6 |
Table 2: Presents the absolute and relative frequency.
Characteristics Number percentage (%)
Preferred Position for Work
Sitting 18 56.3
Standing two 6.3
more sitting 7 21.9 more standing 5 15.6
Feel Pain While Working
Yes 23 71.9
No 9 28.1
Think Pain is Caused by Work
Yes 21 65.6
No 8 25
Absent 3 9.4
Checkout could be more Comfortable
Yes 23 71.9
No 9 28.1
Right Hand Pain
| Few | 4 | 40 |
|---|---|---|
| moderate | 3 | 30 |
| Many | 3 | 30 |
| Absent | 22 | 68.8 |
| Left Hand Pain | ||
| Few | two | 100 |
| moderate | 0 | 0 |
| Many | 0 | 0 |
| Absent | 30 | 93.8 |
| Right Arm Pain | ||
| Few | 1 | 11.1 |
| moderate | 5 | 55.6 |
| Many | 3 | 33.3 |
| Absent | 23 | 71.9 |
| Left Arm Pain | ||
| Few | 0 | 0 |
| moderate | two | 50 |
| Many | two | 50 |
| Absent | 28 | 87.5 |
| Neck Ache | ||
| Few | 0 | 0 |
| moderate | 5 | 45.5 |
| Many | 6 | 54.5 |
| Absent | 21 | 65.6 |
| Right Shoulder Pain | ||
| Little | 3 | 13 |
| moderate | 11 | 47.8 |
| Many | 9 | 39.1 |
| Absent | 9 | 28.1 |
| Left Shoulder Pain | ||
| Few | 4 | 36.4 |
| moderate | 4 | 36.4 |
| Many | 3 | 27.3 |
| Absent | 21 | 65.6 |
| Back Pain | ||
| Few | two | 13.3 |
| moderate | 6 | 40 |
| Many | 7 | 46.7 |
| Absent | 17 | 53.1 |
| Lumbar Region | ||
| Few | two | 18.2 |
| moderate | 4 | 36.4 |
| Many | 5 | 45.5 |
| Absent | 21 | 65.6 |
| Right Leg Pain | ||
| Few | two | 50 |
| moderate | two | 50 |
| Many | 0 | 0 |
| Absent | 28 | 87.5 |
| Left Leg Pain | ||
| Few | two | 100 |
| moderate | 0 | 0 |
| Many | 0 | 0 |
| Absent | 30 | 93.8 |
| Right Foot Pain | ||
| Few | 1 | 50 |
| moderate | 1 | 50 |
| Many | 0 | 0 |
| Absent | 30 | 93.8 |
| Pain In Left Foot | ||
| Few | 1 | 100 |
| moderate | 0 | 0 |
| Many | 0 | 0 |
| Absent | 31 | 96.9 |
| Checkout could be more Comfortable | ||
| Yes | 23 | 71.9 |
| No | 9 | 28.1 |
| Feel Shoulder Pain | ||
| Yes | 25 | 78.1 |
| No | 7 | 21.9 |
| Presents Scapular Dyskinesia MSD | ||
| Yes | 19 | 59.4 |
| No | 13 | 40.6 |
| Has MSE Scapular Dyskinesia | ||
| Yes | 22 | 68.8 |
| No | 10 | 31.3 |
| Presents Lower Limb Discrepancy | ||
| Yes | 0 | 0 |
| No | 32 | 100 |
Table 3: Presents the evaluation regarding comfort and presence of pain.
In the application of Couto’s checklist, the following data were found on the conditions of comfort in the execution of the work. In the evaluation of the chair, the ergonomic condition was reasonable (68%; the work table also obtained reasonable ergonomic condition (58%); keyboard support with poor ergonomic condition (50%); the keyboard with good ergonomic condition (75%); video monitor obtained poor ergonomic condition(50%); cabinet and CPU with excellent ergonomic condition (100%), interaction and layout with good ergonomic condition(72%); work system obtained poor ergonomic condition(50%), room lighting environment with poor ergonomic condition (50%) and accessibility with poor ergonomic condition (20%).
For the preferred position during work, the greatest preference was sitting, with 56.3% opting for this alternative, the second most preferred was more sitting and less time standing (21.9%), followed by more time standing and less sitting (15.6%) and finally standing with 6.3% opting for this preference.
Regarding comfort during checkout, 71.9% said it could be more comfortable, while 28.1% said no. In the question about feeling pain while working, 71.9% of the operators answered yes, and 65.6% believe that this pain is caused by work, while 25% believe that the pain is not related to work.
In the question about feeling pain in the shoulders, 71.9% said they felt pain in the shoulders, and only 28.1% said they did not feel any kind of pain in the region.
It was evaluated in which places the pain is more concentrated, which according to the information collected, most feel pain in the right shoulder, only 9 did not complain of pain in this place.
In the left shoulder, only 11 individuals complained of pain in the region. They also indicated pain in some other part of the body, such as arms, hands, legs, feet, neck, spine and lower back.
In the evaluation of scapular dyskinesia, 19 of the evaluated individuals had it in the MSD and 22 in the MSE.
| Type of dyskinesia | MSD | MSE | ||
|---|---|---|---|---|
| No | % | No | % | |
| Type I | 8 | 25 | 10 | 31.3 |
| Type 2 | 8 | 25 | 5 | 15.6 |
| Type 3 | 2 | 6.3 | 8 | 25 |
| No dyskinesia | 14 | 44 | 9 | 28.1 |
Table 4: Types of scapular dyskinesia in MSD and MSE.
In the chi-square test, to assess the association between previous practice of the function and scapular dyskinesia in the MSD (p=0.586) and LSM (p=0.335), there were no significant results.
In the evaluation of the association of pain in the right hand (p=0.108), left hand (p=0.717), right arm (p=0.487), left arm (p=500), shoulders (right: p=0166; left=519), right (p=0.500) and left foot (p=0.501), lumbar region and spine, no significant results were found in association with scapular dyskinesia of the MSD (p=0.177) and LSM (p=0.076).
Only neck pain was significant (p=0.015) in association with LSM scapular dyskinesia.
Discussion
This study aimed to evaluate scapular dyskinesia in checkout operators and its association with data related to work or musculoskeletal pain.
It was found in research carried out with checkout operators, that due to the conditions provided in the work environment, the position and the muscular effort made in the execution of the function, the checkout operators have a propensity to develop WMSDs. If preventive measures are not adopted, such as adequate environment, labor gymnastics, among others [7].
This propensity occurs due to the long period in which they remain in the same position, as shown in the data reported above where 56.3% work in a sitting position, as well as in the questionnaire 71.9% responded that the checkout could be more comfortable, which indicates that the evaluated feel discomfort in the execution of their function.
As for feeling pain while working, 65.6% answered yes, corroborating the results obtained in a study carried out with checkout operators [8] in which 65% of those evaluated reported feeling pain while working.
Of those evaluated, 46.9% complained of back pain, in two evaluations with checkout operators, 50% and 65% had back pain, results similar to those obtained during the research.
As for neck pain, 34.4% of those assessed, in a study evaluating the working posture of checkout operators, 49 % had pain in the neck region [9, 10].
For the assessment of pain in the shoulders, 78.1% had pain in this region, a result similar to Santana, et al. [11], but above that obtained by a study with 54% 11 of those assessed.
For the right shoulder 71.9% had pain and for the left 34.4%. Santana, et al. [11] also obtained similar results, where the majority had pain in the right shoulder (58.1%) and 25.8% in the left shoulder. In a study where pain in the right shoulder was evaluated, only 14.58% 12 had pain differing from the results obtained in the present study.
In the present study, no significant results were found regarding the association between work position and the presence of dyskinesia, which implies that the way the work is performed does not interfere with the development of dyskinesia.
No significant results were found regarding the association between shoulder pain and dyskinesia, a result that confirms those found in the literature [11, 12]. In relation to the other sites of pain, a significant association was found, only between neck pain and dyskinesia (P=0.015), no data was found in the literature to prove this connection, so further study is needed to confirm whether this is really valid. Association.
Matsuki, et al. [13] analyzed the scapulohumeral rhythm of the dominant and non-dominant limbs and found significant results for the non-dominant limb, similar to what was found in this study regarding the association of neck pain with scapular dyskinesia of the LSM.
The left upper limb is usually the non-dominant limb, that is, with less daily use, it has less strength, flexibility and resistance. So, when the non-dominant is used in bodybuilding exercises, it generates a greater co-contraction of the scapular and cervical musculature, causing movements out of rhythm and overload of the muscles with cervical fixation.
Conclusion
In view of the proposed objective, it was possible to analyze that there is an association with data related to work or musculoskeletal pain with checkout operators. No significant results were found for the association of shoulder pain and scapular dyskinesia. There was an association between neck pain and left upper limb scapular dyskinesia in checkout operators.
References
-
Saccol MF, dos Santos G, Oliano HJ (2017) Inter- and intra- examiner reliability in measuring shoulder rotator muscle strength in different positions with isometric dynamometry. Physioter Pesqui 2(4): 406-411.
-
Cortez PJO, Tomazini JE, Gonçalves M (2011) Strength of shoulder rotator muscles in healthy subjects. Health Science Magazine 1: 1.
-
Mello MAS, Batista LSP, Oliveira VMA, Pitangui ACR, Catuzzo MT, et al. (2014) Association between scapular dyskinesis and shoulder pain in bodybuilders. R brascisaude 18(4): 309-314.
-
Hall CZ, Marques NR, Silva SRD, Dieen JV, Gonçalves M (2011) Electromyographic activity of shoulder muscles during exercises performed with oscillatory and non- oscillatory poles. Rev Bras Fisioter 15(2): 89-94.
-
Miachiro NY, Camarini PMF, Tucci HT, McQuade KJ, Oliveira AS (2014) Is the clinical examination of observation of scapular dyskinesis capable of differentiating patients with the dysfunction from normal ones?.Braz J Phys Ther 18(3): 282-289.
-
Moreira LGP, Pereira L (2016) Association between scapular dyskinesia and pain processes resulting from injuries to the glenohumeral joint. Revista Univap 22(40): 1-5.
-
Souza JAC, Filho MLM (2017) Ergonomic analysis of movements and postures of checkout operators in a supermarket located in the city of Cataguases, Minas Gerais.
-
Battisti HH, Guimaraes ACA, Simas JPN (2005) Physical activity and quality of life of supermarket cashier operators. R Bras Ci Mov 13(1): 71-78.
-
Batiz EC, Santos AF, Licea OEA (2009) The attitude at work of supermarket checkout operators: a constant need for analysis. Production 19(1): 190-201.
-
Teixeira CS, Torres MKL, Moro ARP, Merino EAD (2009) Factors associated with the work of checkout operators: investigation of musculoskeletal complaints. Production 19(3): 558-568.
-
Santana EP, Ferreira BC, Ribeiro G (2009) Association between scapular dyskinesia and shoulder pain in swimmers. Rev Bras Med Esport 15(5): 342-346.
-
Oliveira VMA, Batista LSP, Pitangui ACR, Araújo RC (2013) Effectiveness of Kinesio Taping in pain and scapular dyskinesis in athletes with shoulder impingement syndrome. Rev Dor 14(1): 27-30.
-
Matsuki K, Matsuki KO, Mu S, Yamaguchi S, Ochiai N, et al. (2011) In vivo 3-dimensional analysis of scapular kinematics: comparison of dominant and non dominant shoulders. J Shoulder and Elbow Surgery 20(4): 659- 665.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial