Physiotherapy Management of Postoperative Peroneal Nerve Palsy in a Case of Hereditary Multiple Exostoses
Hereditary Multiple Exostoses (HME) is a non-frequent autosomal dominant disorder, described by nearness of exostoses. In symptomatic patient surgical intervention is required, most common surgery is wedge osteotomy. One of the complications of this surgery is peroneal nerve palsy. The intention of this case report is to explain the physiotherapy intervention strategies and report its effectiveness in symptomatic management of peroneal nerve palsy (axonotmesis) post-surgically in a 23-yearold male with HME. Patient had difficulty in moving his right ankle and shock like pain in his right lower limb post-operative. Patient was diagnosed to have right peroneal nerve injury. Patient was managed on the basis of clinical presentation with supervised and unsupervised physiotherapy for 10 weeks. Supervised physiotherapy intervention consisted of patient’s education, neural mobilization, electrical stimulation, sensory reeducation (cognitive behavior therapy), exercise therapy and counseling for 45-60 min a day for 6 days a week for first 6 week later 5 days per week. The effectiveness of supervised physiotherapy was followed for 10 weeks and sensory and motor assessment was performed, along with an S-D curve was performed to measure the improvement. For the next 3 month follow up for the patient was taken. Physiotherapy management was found to be effective in case of peroneal neuropathy with increased patient satisfaction.
Introduction
Hereditary multiple exostoses (HME) otherwise called familial osteochondromatosis is an acquired genetic disorder described by the nearness of different exostoses (osteochondromas) [1, 2]. HME is a rare autosomal dominant disorder [2, 3]. Its prevalence is 1 out of 50,000 in the population, although it is rarer in Indian population [2, 4, 5]. It is commoner in male than female [5]. HME is monogenetic autosomal dominant condition occur due to the deprivation of function of 2 genes: exostosin-1 (EXT1) on chromosome 8 and exostosin-2 (EXT2) on chromosome 11 [2]. It is a benign tumor defined by WHO as a cartilage- capped bony outgrowth. It can be broad based or stemmed and made up of cortex and a marrow cavity both continuous with the host bone. Osteochondroma develops and grows in number until the growth plate closes, frequent location of osteochondroma is on the active growth plates of long bones on the lateral part [2]. Frequently involve joint are pelvis, scapula and proximal tibia and distal femur [1, 2]. In most of the cases it is asymptomatic but complications due to HME are bone deformity, fractures, neurological compression, limb length discrepancy [4, 6]. Common deformities due to HME are Made lung type deformities Table 1 (forearm), coxa valgus (hip), genu valgus (knee), valgus angulation of ankle, Brachydactylic (hand), pseudo Tmallet finger or any angular deformity (usually on ulnar side) [2].
Classification is given as follows:
| I | No deformities & No functional limitations | A | Less than or equal five sites with osteochondromas |
|---|---|---|---|
| B | More than five sites with osteochondromas | ||
| II | Deformities with no functional limitations | A | Less than or equal five sites with deformities |
| B | More than five sites with deformities | ||
| III | Deformities and functional limitations | A | Functional limitation of one site |
| B | Functional limitation of more than one site |
Table 1: Clinical classification of HME is divided into 3 categories based on the bone segment affected and presence of deformiti
Diagnosis of HME can be done by genetic screening at an early stage. Radiographs can show osteochondromas of appendicular skeletal. CT scan is used for regions difficult to visualize such as spine, thorax and pelvis. For accurate measurement of cartilage cap thickness and lesion to surrounding soft tissue structure MRI is preferred [2]. Currently the treatment for severe symptomatic patients is surgery [1, 2, 3, 4, 8]. Correction of deformity is done by removal combined differently with osteotomies, stapling and lengthening procedure [9]. Conservative treatment can be given pre and post-surgery [1].
There are the complications of osteotomy surgery such as deep vein thrombosis, infections, and delayed union, stiffness of knee and paralysis of the common peroneal nerve [10]. The common and least understood complication of surgery is paralysis of the peroneal nerve that leads to weakness of dorsiflexors of foot and extensor hallucis longus, along with severe pain in foot and sensory disturbance [10]. Electro-diagnosis helps to determine the type and amount of nerve injury [11, 12]. Strength – Duration curve is used for regular evaluation of the condition [12]. The treatment includes ice therapy, heat therapy, and neural mobilization, strengthening exercise, soft tissue mobilization and sensory adaptation [11, 13, 14]. This case report is unique and focuses on physiotherapy management of common peroneal nerve involvement in post-surgical patients of HME.
Case Report
In a physiotherapy department a 23 year old person came with complaints of difficulty in walking and shock like pain in his right foot postoperatively from wedge osteotomies and correction surgery for HME since July 2019. Patient was diagnosed to have HME and he has multiple exostoses in tibia and femur in both knees and it was non- cancerous. It was asymptomatic before 3 years, but since last 1 year he was having difficulty and pain in walking and running. He consulted the doctor and he was advised for wedge osteotomy surgery. He had surgery for his left knee in December 2018. Non weight bearing with the help of a walking frame was advised for 20 days and he was having swelling in his left knee and ankle at that time physiotherapy treatment was given. After 45 days the patient was able to do his activities of daily living (ADL).
His right knee was operated on in July 2019. After two days post-operatively he was not able to move his right ankle and had severe pain in the lower limb. He consulted his surgeon, after the initial examination doctor prescribed him B12 medication and gabapentin. After a week there was no improvement in his condition and he was having difficulty in moving his ankle and great toe. He was discharged from hospital and recommended for physiotherapy Figures 1 & 2.
He visited our department after 20 days. He has a family history of multiple exostoses, but he was asymptomatic. Patient describes his pain as continuous and pins and pricks type which increases with ankle movement. NPRS score of patients 8/10. Patient had hyperesthesia. His sleep was disturbed due to pain.
We conducted the clinical examination of the patient. Patient left ankle positioned in equino-varus position. Edema was present and the skin temperature of the left ankle was a bit colder. Ankle reflex was absent. Sensory examination revealed superficial and deep sensory of the left ankle are affected. Tinel’s sign was positive. Bowel and bladder were intact. Following the motor examination, the left range of motion and strength was functionally full and painless. On
the right side the ankle range of motion is restricted and painful and muscle strength is affected. Investigation: X –ray of patient was performed before and
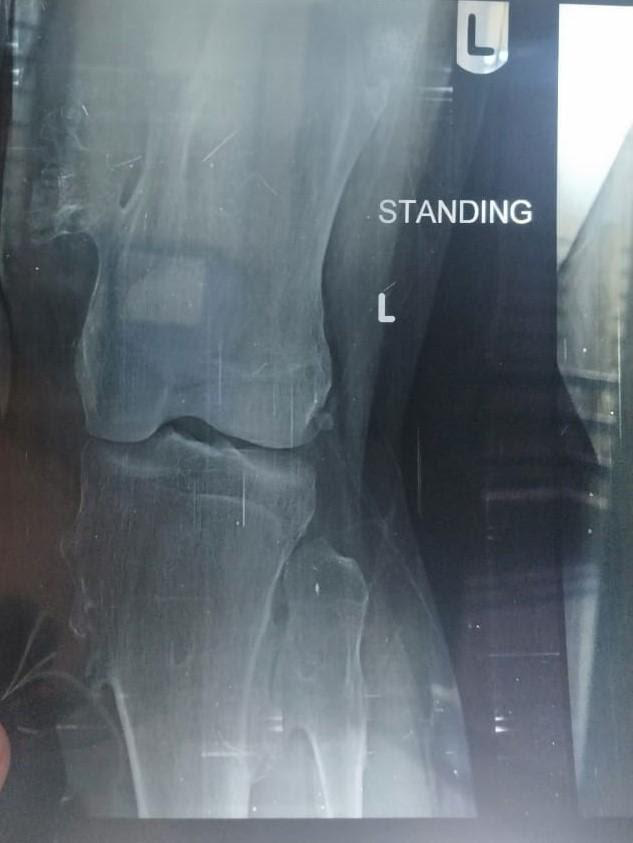
after. S-D curve was performed for the left peroneal nerve performed after 21 days post- surgery to know the extent of peripheral nerve injury.


X- Ray reports showed:
- Figure1: Multiple exostoses in tibia and femur.
- Figure 2: Wedge osteotomy with tibial fixation was performed
Physical Therapy Management
As per history and findings in physical therapy examination, physiotherapy rehabilitation program was designed for left peroneal nerve injury (axonotmesis) for 6 days a week for initial 6 week then it was reduced to 5 days a week for next 4 week.
In the first 6 week, the primary aim was to reduce pain, prevent contracture, motor retraining and desensitization and prevent further complication.
Secondary aim was to promote progressive weight bearing on the left limb. For the next 4 week, the primary aim was to improve proprioception and kinesthetic awareness of the joint. Additionally, sensory reeducation and strengthening of the muscles was considered. Secondary aim was to improve functional activity of daily living. Supervised physiotherapy consists of patient’s education, exercise therapy, electrotherapy and manual therapy, provided for 45-60 min. The unsupervised home exercise protocol (HEP) was designed based on his tolerance, improvement and maintenance of exercise adherence.
The initial treatment protocol was based on counseling regarding the condition and its prognosis to facilitate the exercise adherence. Physiotherapy in initial consist of passive range of motion, neural mobilization, electrical stimulation (interrupted galvanic current) and icing to reduce pain, swelling, improve range of motion and to prevent muscle atrophy and contracture along with desensitization in non-weight bearing. During later stage additional to the treatment mentioned above strengthening, sensory reeducation and functional retraining is included for muscle reeducation and weight-bearing in the limb. A HEP was designed and progressed as appropriate for better prognosis of the condition. He was provided with a manual for HEP which he had to follow strictly. HEP consists of self- calf stretching, active-assisted range of motion exercises and icing.
To maintain the muscle property we started with electrical stimulation as progression we went for isometric strengthening and gravity eliminated exercises, then we progressed to isotonic exercise against gravity with progressive resistance.
In 10 week, he received 56 supervised physiotherapy sessions approximately 45-60 minute a day and discharged with advice to resume daily activities and to exercise for at least 30 minute a day Tables 1-7. On discharge he had minimal sensory impairment and was able to walk independent. He was counsel for follow up sessions and after the finish of sessions patient was able to perform his activities of daily living independently.
Every month follow-up was taken for the next 3 months, during the follow up there was development of active insufficiency of tibialis anterior. Therefore, stretching of tibialis anterior was added. There was improvement in strength, proprioception and range of motion of the ankle and toe. Walking on various surfaces had also improved. Activities of daily living and Instrumental activities of daily living independently were performed by the patient.
| Sensation | Right Lower Limb (Affected Limb) | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | After 2 Weeks | After 4 Weeks | After 6 Weeks | After 8 Weeks | After 10 Weeks | ||
| Pain | 4 | 4 | 3 | 3 | 3 | 1 | |
| Touch | 3 | 3 | 2 | 1 | 1 | 1 | |
| Temperature | 5 | 2 | 2 | 1 | 1 | 1 | |
| Vibration | 6 | 5 | 4 | 2 | 2 | 2 | |
| Two Point Discrimination | 5 | 5 | 4 | 2 | 2 | 2 | |
| Kinesthesia | 4 | 2 | 2 | 1 | 1 | 1 | |
| Proprioception | 4 | 2 | 2 | 1 | 1 | 1 | |
| Streognosis | 2 | 2 | 2 | 1 | 1 | 1 | |
| Key To Grading | 1. Intact, 2. Decreased, 3. Exaggerated, 4. Inaccurate, 5. Absent, 6. Inconsistence |
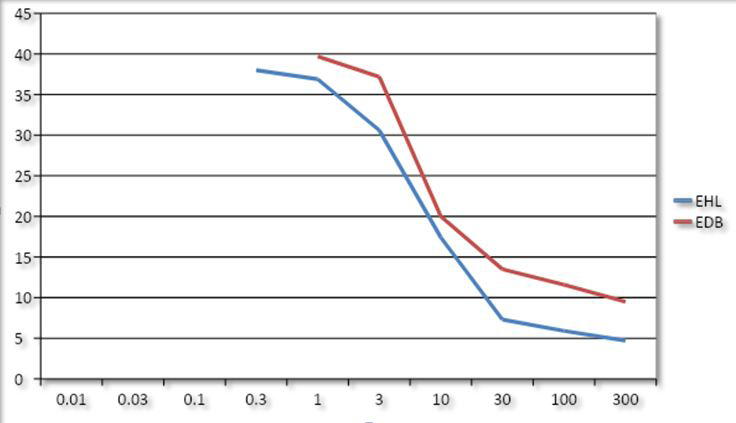
Table 2: S-D Curve Pre- Treatment (X axis- Duration (in milliseconds); Y axis- Intensity).
| Muscle Tested | Right Side (Affected) | Left Side (Non-Affected) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 2 Wk | 4 Wk | 6 Wk | 8 Wk | 10 Wk | Baseline | 2 Wk | 4 Wk | 6 Wk | 8 Wk | 10 Wk | |
| Knee Flexors | 4 | 4 | 4 | 4 | 4 | 4 | 4+ | 4+ | 4+ | 4+ | 4+ | 4+ |
| Knee Extensors | 4 | 4 | 4 | 4 | 4 | 4 | 4+ | 4+ | 4+ | 4+ | 4+ | 4+ |
| Ankle Dorsiflexion | 1 | 2 | 3 | 3- | 3+ | 4 | 4+ | 4+ | 4+ | 4+ | 4+ | 4+ |
| Ankle Plantar Flexors | 2 | 2+ | 3 | 3+ | 3+ | 4 | 4+ | 4+ | 4+ | 4+ | 4+ | 4+ |
| Invertors | 1 | 4- | 4+ | 4+ | 4+ | 4+ | 4+ | 4+ | ||||
| Evertors | 1 | 2+ | 3 | 3+ | 4 | 4 | 4+ | 4+ | 4+ | 4+ | 4+ | 4+ |
| Toe Extensors | 1 | 2- | 2 | 3- | 3 | 3+ | 4+ | 4+ | 4+ | 4+ | 4+ | 4+ |
| Toe Abductors | 1 | 1+ | 2- | 3 | 3 | 3+ | 4+ | 4+ | 4+ | 4+ | 4+ | 4+ |
Table 3: S-D Curve Pre- Treatment (X axis- Duration (in milliseconds); Y axis- Intensity).
| Duration | Baseline (21 Days After) | After 10 Weeks Of Treatment | ||
|---|---|---|---|---|
| EHL (Proximal Muscle) | EDB ( Distal Muscle) | EHL | EDB | |
| 300 Ms | 4.7 | 11.6 | 3 | 10 |
| 100 Ms | 5.9 | 12.2 | 3.1 | 10.1 |
| 30 Ms | 7.3 | 15.5 | 3.1 | 10.2 |
| 10 Ms | 17.4 | 20 | 3.1 | 10.2 |
| 3 Ms | 30.6 | 37.2 | 3.1 | 10.2 |
| 1 Ms | 36.9 | 39.7 | 5 | 20 |
| 0.3 Ms | 35.5 | NR | 7 | 25.5 |
| 0.1 Ms | NR | NR | 10 | 26 |
| 0.03 Ms | NR | NR | 11.5 | 26.3 |
| 0.01 Ms | NR | NR | 13.2 | 32.1 |
| (EHL-extensor hallucis longus ; EDB- extensor digitorum brevis; NR- No response) |
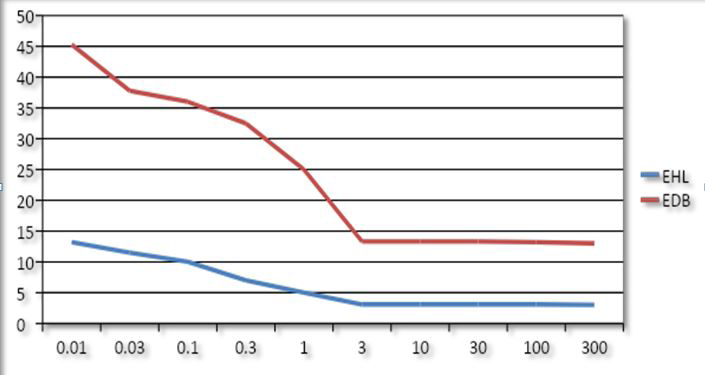
Table 5: S-D Curve Pre- Treatment (X axis- Duration (in milliseconds); Y axis- Intensity).
| Baseline (21 Days After) | After 10 Weeks Of Treatment | |||
|---|---|---|---|---|
| Duration | EHL (Proximal Muscle) | EDB (Distal Muscle) | EHL | EDB |
| Duration | ||||
| 300 Ms | 4.7 | 11.6 | 3 | 10 |
| 100 Ms | 5.9 | 12.2 | 3.1 | 10.1 |
| 30 Ms | 7.3 | 15.5 | 3.1 | 10.2 |
| 10 Ms | 17.4 | 20 | 3.1 | 10.2 |
| 3 Ms | 30.6 | 37.2 | 3.1 | 10.2 |
| 1 Ms | 36.9 | 39.7 | 5 | 20 |
| 0.3 Ms | 35.5 | NR | 7 | 25.5 |
| 0.1 Ms | NR | NR | 10 | 26 |
| 0.03 Ms | NR | NR | 11.5 | 26.3 |
| 0.01 Ms | NR | NR | 13.2 | 32.1 |
| (EHL-extensor hallucis longus; EDB-extensor digitorum brevis; NR- No response) |
Table 4: S-D Curve Pre- Treatment (X axis- Duration (in milliseconds); Y axis- Intensity).
| Intensity | Frequency | Duration | |
|---|---|---|---|
| Cryotherapy | 10-15 min | Given in all PT session | 56 sessions |
| Electrical stimulation for muscles supplied by peroneal nerve (interrupted galvanic current) | 30 contraction, 3 sets | Given in all PT session | 56 sessions |
| Electrical stimulation for peroneal nerve (faradic current) | 30 contraction, 3 set | Started at the end of 4 week | 32 sessions |
| Neural mobilization of peroneal nerve | 90 repetition, 3 set | Given in all PT session | 56 sessions |
| Active assisted movement of ankle | 10-15 repetition for each movement | Started at the end of 2 week | 44 sessions |
| Ankle proprioceptive training | 10-15 repetition for 2 set | Started at the end of 6 week | 20 sessions |
| Desensitization training (softer to rougher surface) | Initially: for 1-2 min | Given in all PT session | 56 sessions |
| Desensitization training (softer to rougher surface) | Progressively: 5-10 min | Given in all PT session | 56 sessions |
| Sensory reeducation | 3-4 repetition for couple of minute | Started at the end 3 week | 38 sessions |
| Isometric exercise of all ankle muscles | 10 sec hold for 10 repetition 2 set | Started at the end of 2 week | 44 sessions |
| Isotonic exercises of all ankle muscles with manual resistance | 5-10 second hold for 10 repetition 2 set | Started at the end of 4 week s | 32 sessions |
Table 6: Physiotherapy intervention for patient with PNP.
| Home exercise program | Intensity | Frequency | Duration |
|---|---|---|---|
| Icing | 15-20 minute | 3 times a day | 56 sessions |
| Calf self-stretching | 30 second hold, 3 repetitions | Twice a day | 44 sessions |
| Active – assisted range of motion exercises | 10 repetitions | Twice a day | 44 sessions |
| Calf raise | 5 to 10 repetitions | Twice a day | 44 sessions |
| Walking on various surfaces | 30 minute at least | Once a day at least | 40 sessions |
Table 7: Home exercise program for patient with PNP.
Discussion
The case report is intended to outline one of the least understood complication peroneal nerve palsy of wedge osteotomy surgery performed on a young patient diagnosed to have hereditary multiple exostoses and to provide insight in physiotherapy management. In our case the patient had difficulty and pain in moving his right ankle, along with hypersensitivity of the sole of foot. The physiotherapy management was based on a combination of electrical stimulation, sensory reeducation, peripheral nerve mobilization and various exercises consisting strengthening and proprioceptive training.
There are few literatures that describe physiotherapy management of peroneal neuropathy. Literature shows modalities such as moist heat, ice pack and electrical stimulation can be used with precautions for neuropathy and nerve mobilization can also be used [11, 12, 13, 14]. Previous reports suggest that neural mobilization may be helpful in unfavorable conditions such as disc herniation and neuropathy [13, 14].
No literature is available that describes the combination of electrical stimulation, neural mobilization, sensory reeducation and different exercise in case of postoperative peroneal nerve injury in a young patient having multiple exostoses. In our case we used a combination of above mentioned techniques with unsupervised home based protocol to give satisfactory treatment. Our patient had been benefited with exercises and symptoms were relieved.
Conclusion
Physiotherapy management was initially given in the form of desensitization of the hypersentive area, galvanic stimulation and neural mobilization. As there was improvement in the condition later sensory reeducation, supervised and unsupervised exercises were added. The protocol is effective for postsurgical peroneal nerve palsy in young patients with hereditary multiple exostoses. Further research is required before generalizing the findings for other patients.
References
-
Kanik ZH, Gunaydin G, Sozlu U, Citaker S, Esen E (2016) Eccentric training as an adjunct to rehabilitation program for hereditary multiple exostoses: a case report. Journal of clinical and diagnostic research 10(2): YD03-04.
-
Beltrami G, Ristori G, Scoccianti G, Tamburini A, Capanna R (2016) Hereditary multiple exostoses: a review of clinical appearance and metabolic pattern. Clinical Cases in Mineral and Bone Metabolism 13(2): 110-118.
-
Pacifici M (2017) Hereditary multiple exostoses: new insights into pathogenesis, clinical complications, and potential treatments. Current osteoporosis reports 15(3): 142-152.
-
Nasr B, Albert B, David CH, da Fonseca PM, Badra A, et al. (2015) Exostoses and vascular complications in the lower limbs: two case reports and review of the literature. Annals of vascular surgery 29(6): 1315-e7.
-
Kalyani R, Prabhakar K, Gopinath B, Sheik Naseer B, Krishnamurthy DS (2014) Multiple heriditary exostoses in a family for three generation of Indian origin with review of literature. Journal of clinical and diagnostic research 8(10): LD01-LD03.
-
Yinusa W, Owoola AM, Esin IA (2010) Hereditary multiple exastoses: Case report. Nigerian journal of clinical practice 13(2): 218-222.
-
Mordenti M, Ferrari E, Pedrini E, Fabbri N, Campanacci L, et al. (2013) Validation of a new multiple osteochondromas classification through Switching Neural Networks. American Journal of Medical Genetics Part A 161(3): 556-560.
-
Payne R, Sieg E, Fox E, Harbaugh K, Rizk E (2016) Management of nerve compression in multiple hereditary exostoses: a report of two cases and review of the literature. Child’s Nervous System 32(12): 2453- 2458.
-
Fabbri N, Donati D (2014) Multiple Exostoses. In Picci P, et al. (Eds.), Atlas of Musculoskeletal Tumors and Tumor like Lesions. Springer pp: 71-74.
-
Jackson JP, Waugh W (1974) The technique and complications of upper tibial osteotomy: a review of 226 operations. The Journal of bone and joint surgery 56(2): 236-245.
-
Baima J, Krivickas L (2008) Evaluation and treatment of peroneal neuropathy. Current reviews in musculoskeletal medicine 1(2): 147-153.
-
Forster A, Clayton EB, Palastanga N (1985) Clayton’s electrotherapy: theory and practice. In Bailliŕe Tindall 5th (Edn.), pp: 240.
-
Villafañe JH, Pillastrini P, Borboni A (2013) Manual therapy and neurodynamic mobilization in a patient with peroneal nerve paralysis: a case report. Journal of chiropractic medicine 12(3): 176-181.
-
Anandkumar S (2012) Physical therapy management of entrapment of the superficial peroneal nerve in the lower leg: a case report. Physiotherapy theory and practice 28(7): 552-561.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial