Effectiveness of Ultrasound-Guided Dry Needling In Painful Musculoskeletal Conditions: A Systematic Review and Meta-Analysis
Objective: To identify the treatment effects of pain and disability in US-guided DN on various painful musculoskeletal conditions. Methods: A comprehensive literature search of six databases without language restrictions was conducted for relevant articles containing quantitative data. Randomized controlled trials (RCTs) or quasi-experimental studies involving the effectiveness of US-guided DN on pain and disability in adult patients (age >18 years) with painful musculoskeletal conditions were included. Studies that not related to US-guided DN, paediatric patients, and patients with acute, trauma, postoperative, or malignant pain were excluded. The quality and certainty of the included articles were assessed using the PEDro scale and the GRADE approach respectively. Results: Four high-quality studies with a total of 240 patients’ data, aged 18-71 years old, were included in this meta-analysis. Results showed a significant improvement in pain with US-guided DN (p<0.001) with a standardized mean difference of 0.96 (95% CI: 0.66, 1.27; I2=31.23). On the other hand, a significant improvement in disability is seen with US-guided DN (p<0.001) with a standardized mean difference of 0.85 (95% CI: 0.61, 1.09; I2=30.89). Both outcomes had symmetric funnel plots, and the results of Egger’s test showed no significant publication bias. Conclusion: US-guided DN is a safe and effective treatment modality for reducing pain and disability for some painful musculoskeletal conditions in the short-term. However, only limited high-quality study examined the effectiveness of USguided DN over various painful musculoskeletal conditions. Further high-quality studies that focus on the long-term treatment effects of US-guided DN on various painful musculoskeletal conditions are warranted. Impact statement: Our systematic review suggested that ultrasound guided dry needling has short-term effects for those painful musculoskeletal conditions which led 2 out of 10 people to seek medical care annually in reducing pain and disability
Introduction
Around one-third of the world’s population experiences a chronic and painful musculoskeletal condition [1]. Musculoskeletal conditions comprise more than 150 diseases that affect the bones, joints, muscles, fascia, tendons, and ligaments, which are the major structures causing pain and disability [2]. These musculoskeletal conditions can significantly impact a person’s quality of life, physical functioning, and ability to work or perform daily activities [2]. They can also result in increased healthcare costs and may require long-term management and treatment [3]. In England, musculoskeletal conditions led 2 out of 10 people to seek medical care annually, either in primary or secondary care [4]. Effective management of chronic musculoskeletal conditions is important to reduce pain, improve physical functioning, and prevent further complications.
Dry needling (DN) is widely used in the management of a variety of musculoskeletal conditions. It is regarded as a minimally invasive technique [5], which involves the insertion of a thin needle into soft tissues where hyperchromatic, rounded nodules and bead-like or spindle-shaped muscle fibres are formed [6]. DN potentially decreases peripheral nociceptive inputs mechanically [7] and activates the endogenous opioid system to induce an analgesic effect for pain relief [8]. DN was postulated to reduce the overlap of the contractile proteins and relax the sarcomeres [9]. Therefore, DN was extensively utilized for pain management and soft tissue tension relief in musculoskeletal conditions. In previous meta-analysis, DN showed some relief in pain [10, 11] and disability [12] in musculoskeletal conditions.
Recently, musculoskeletal ultrasound (US) has been frequently utilized by physiotherapists for the visualization of musculoskeletal structures in painful musculoskeletal conditions. US-guided DN can potentially offer more accurate and precise admission of the DN by targeting specific trigger points or structures causing the patient’s condition. Real- time visualization by US also enables the insertion of the needle at the appropriate depth and angle, which enhances the safety of DN and reduces the risk of adverse events such as damaging the major artery or nervous tissue [13]. The effectiveness of US-guided DN on pain and disability has been investigated in a wide range of musculoskeletal conditions, including myofascial pain syndrome [14], tendinopathy [15], knee osteoarthritis [16], etc. Nevertheless, there is no prior study summarizing information on whether the change in pain and physical function was consistent after US-guided DN in painful musculoskeletal conditions.
This systematic review and meta-analysis aims to identify the short-term treatment effect of pain and disability in US- guided DN on various painful musculoskeletal conditions. The hypotheses of this meta-analysis are that: US-guided DN is more effective in reducing pain and disability than control or no-treatment group in painful musculoskeletal conditions.
Methods
Data Sources and Searches
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [17] and Meta-Analysis of Observational Studies in Epidemiology (MOOSE) [18] standards were followed for conducting this meta- analysis. The meta-analysis’s protocol was made available in the PROSPERO database under the registration number CRD42022347522. To specifically identify the effectiveness of US-guided DN, we only included studies with US-guided DN as the intervention group, hence the slight deviation from the published protocol. On April 28, 2023, a comprehensive literature search was conducted without regard to language in the CINAHL Complete, Cochrane Library, EMBASE, Medline, PubMed, and PsycINFO databases for all relevant studies with quantitative data to minimize the possibility of missing data. For non-English content, we first utilized “Google Translate,” followed by the advice of native translators. The search history is presented in Supplementary Table 1, while the search terms are listed in Supplementary Table 2.
Study Selection
Randomized controlled trials (RCTs) or quasi- experimental studies involving the effectiveness of US-guided DN on pain and disability in adult patients (age >18 years) with painful musculoskeletal conditions were included. We aim at musculoskeletal conditions with the following criteria: back problems, including lumbago, backache, cervicalgia, degeneration of lumbar, lumbosacral or intervertebral disc, and displacement of lumbar intervertebral disc; joint disorders, including joints in lower leg, ankle, foot, shoulder region, pelvic region and thigh; and musculoskeletal or connective tissue disorders, including limb pain, plantar fascial fibromatosis, enthesopathy of unspecified site, myalgia and myositis, and muscle spasm [19]. In addition, to ensure rigorous results, only studies with a low risk of bias were included. Studies involved with mini-scalpel needle therapy, electro-acupuncture, conventional acupuncture technique based on the traditional Chinese medicine approach, paediatric patients, and patients with acute, trauma, postoperative, or malignant pain were excluded. Additionally, abstracts, editorial comments, and unpublished studies were also omitted.
Data Extraction and Quality Assessment
Two independent reviewers independently screened the title and the abstracts for eligibility, the remaining full text were assessed. Any disagreements were resolved with consensus of a third reviewer. A standardized data extraction sheet that included the names of the authors, the year of publication, the clinical status, the number of participants, participant characteristics, experimental and control interventions, intervals of intervention, outcome measures, results, and adverse events was used to extract pertinent information from the included studies. Any missing data were reported and handled by contacting the authors.
Two independent reviewers used the PEDro scale [20] and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach [21] to assess the quality and certainty of the included studies respectively. Any disagreements were resolved by a third reviewer. The PEDro scale has a maximum score of 11 points, with a score from 0 to 5 representing low quality and a score from 6 to 10 representing high quality [22]. All studies below a score of 6 were excluded. Based on the GRADE’s five criteria, risk of bias, inconsistency, indirectness, imprecision, and publication bias, there are four different degrees of certainty in the evidence, very low, low, moderate, and high [21]. All outcomes were assessed individually, as the certainty may vary across outcomes.
Data Synthesis and Analysis
Comprehensive Meta-Analysis version 3.0 (Biostat, Englewood, New Jersey, USA) was used for the statistical analysis. Participants who received US-guided DN were compared to those who received placebo US-guided DN, pharmaceutical interventions, or no intervention. Participants’ baseline data in pain and disability were compared to that of follow-up in the short-term (<12 weeks) for calculation of effect sizes. The outcomes were presented as a standardized mean difference (SMD) with 95% confidence intervals (CIs). All p-values in this meta-analysis were two-tailed, with statistical significance set at ≤0.05. The risk of heterogeneity was assessed by the I2 index, and a fixed-effects model was selected if the heterogeneity was <50%. Funnel plots and Egger’s test was used to assess the risk of publication bias, with an asymmetric plot and p≤0.05 indicated the risk of publication bias. Additionally, a sensitivity analysis was also conducted to evaluate the robustness of outcomes by step-wise removal of each study.
Role of the Funding Source
The funders played no role in the design, conduct, or reporting of this study.
Result
Search Outcomes
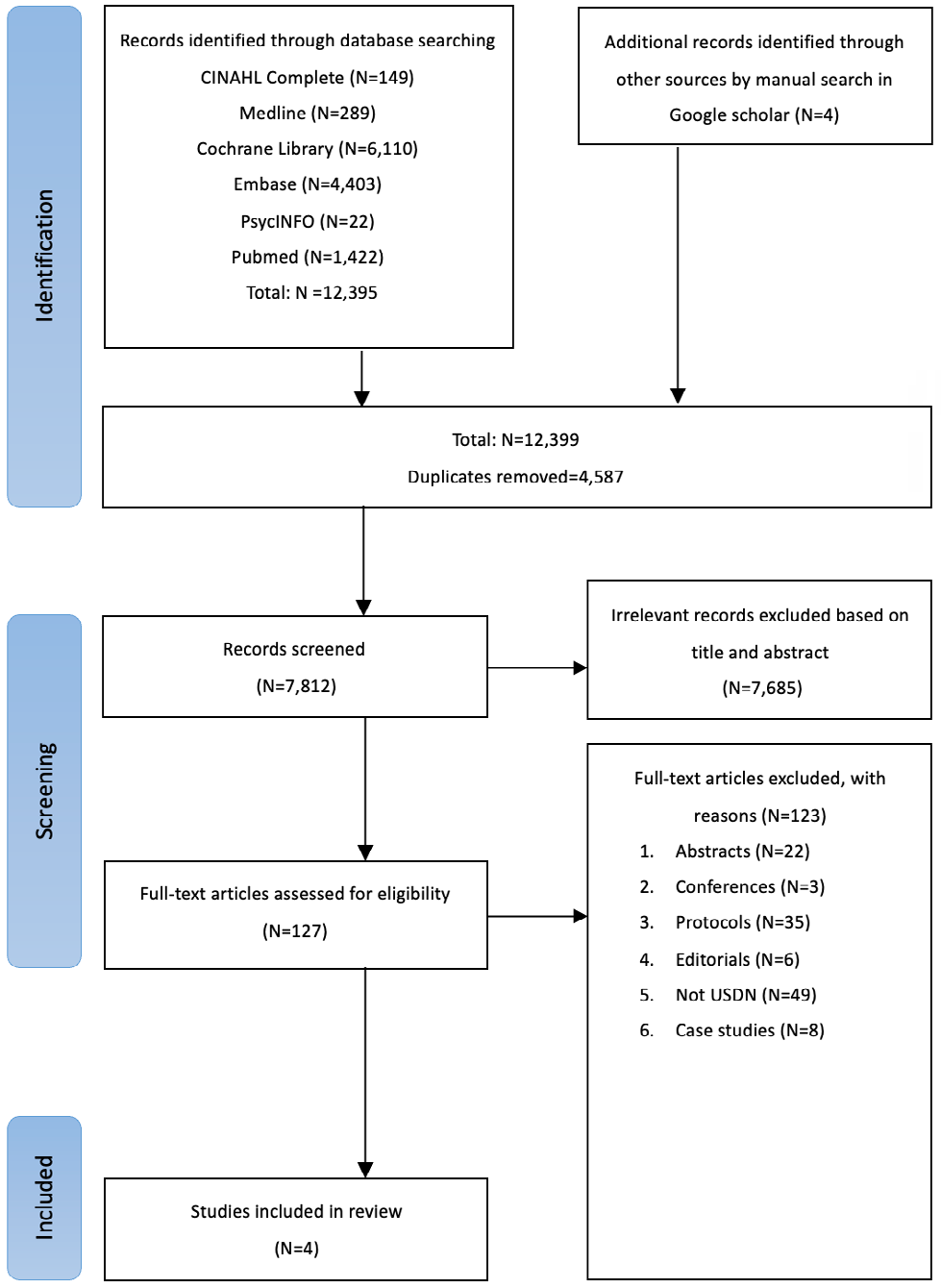
A total of 12,399 studies were retrieved from the databases. A total of 4,587 duplicate studies were identified and removed. A further 7,685 studies were excluded by reviewing the titles and abstracts, and an addition of 123 studies were removed after assessing the full texts by two independent reviewers. Finally, a total of four studies [15, 16, 23, 24] were included in our meta-analysis. The PRISMA flowchart of the study selection was presented in Figure 1, with the reasons of exclusion documented in Supplementary Table 3. A third reviewer resolved any disagreements during the screening process and no authors were contacted for further data acquirement.
Characteristics of the Included Studies
Four high-quality studies with a total of 240 patients’ data, aged 18-71 years old, were included in this meta- analysis. All studies incorporated US guidance into DN as the intervention groups, with conventional treatment approaches as the control groups. Among the four studies, two identified treatment effects of US-guided DN in patients with knee conditions, including knee osteoarthritis and jumper’s knee. One study identified treatment effects of US- guided DN in patients with piriformis syndrome, while the other focused on patients with postherpetic neuralgia mixed with myofascial pain syndrome. The patients with younger age involved piriformis syndrome and jumper’s knee, while the patients with older age involved myofascial pain syndrome and knee osteoarthritis. The characteristics of the included studies are described in Table 1.
| Authors | Conditions | US DN group | Control group | Adverse events | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of partici pant | Age | Gender (female) | Treatment technique | Treatment interval | Received treatment | No. of participant | Age | Gender (female) | |||
| Huang, et al. [25] (2022) | Postherpetic neuralgia mixed with myofascial pain syndrome | 28 | 69.5 (1.6) | 16 | The myofascial trigger points were punctured with stainless steel filiform needle on the real-time US- guided in-plane technique to induce obvious aching and distending pain. | Once a week for 4 weeks | Pharmaco therapeutic intervention | 26 | 70 (1.25) | 16 | No serious adverse events recorded |
| Tabatabaiee, et al. [24] (2019) | Piriformis syndrome | 15 | 31.26 (6.09) | 10 | DN needle was moved towards to piriformis muscle while the needle tip was observed using US. The dynamitic needling technique was performed by slowly moving the needle in and out of the muscle with a goal to eliciting a local twitch response. | Three sessions with 48-hours intervals over one week | Waitlist with advice only | 15 | 30.26 (5.54) | 9 | Two participants reported adverse effects during DN including severe pain and bleeding |
Table 1: Characteristics of the included studies.
| Pang, et al. [17] (2022) | Knee osteo arthritis | 30 | 60.56 (5.93) | 21 | Under US guidance, DN needles were inserted to area with heterogenicity and mucoid degenerative changes. The needles was then manipulated in- and-out of the targeted tissue five times every five minutes over fifteen minutes. | One session per week for 4 weeks | Routine exercise program and educational material related to knee osteoarthritis | 30 | 61.97 (5.49) | 24 | No serious adverse events recorded |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sharif, et al. [16] (2023) | Jumper’s knee | 48 | 22 (4.75)* | 24 | Treatment area were identified with degenerative change under US guidance, three DN needles were placed, of which was left for three seconds, depending on the extent of tendon degenarations, the total number of needle insertions can range from 20 to 30. | Two sessions per week for one month | Conventional physical therapy | 48 | 22 (3) | 18 | Not mentioned |
Table 2: Characteristics of the included studies.
Quality Assessment of Included Studies
All studies scored 8 on the PEDro assessment, indicating high quality studies. All studies failed to blind participants and therapists, resulting in the deduction of scores. In addition, all outcomes were graded as having high certainty. The PEDro assessment of all included studies and the GRADE score of all outcomes were presented in Supplementary Tables 4 and 5 respectively.
Pain
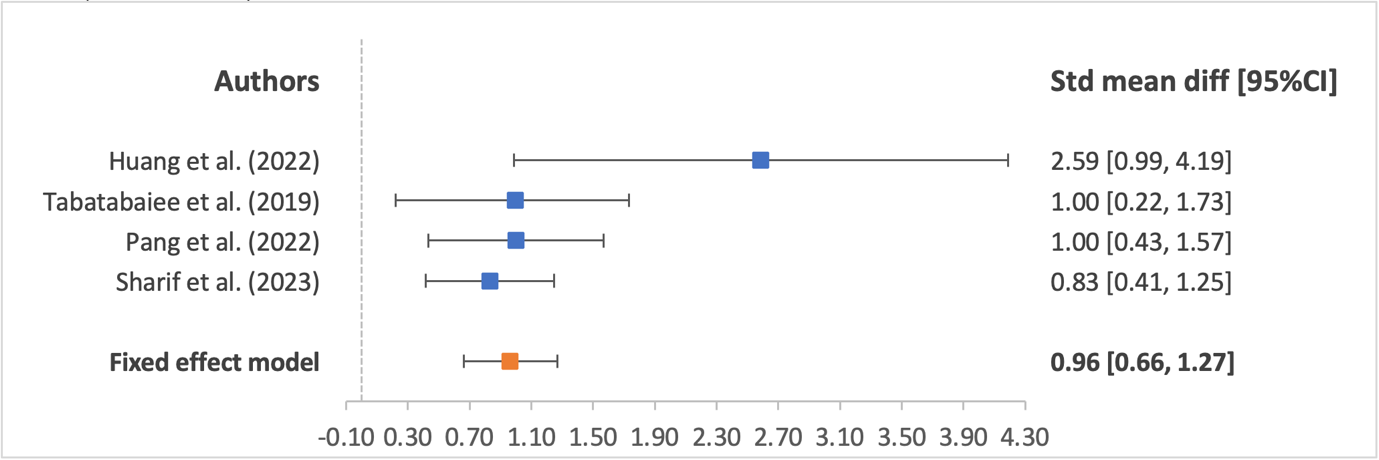
The standardized mean difference of pain before and after treatment in the short term (<12 weeks) was presented in a forest plot in Figure 2. All studies utilized the visual analog scale (VAS) to measure the treatment effect of US- guided DN in pain. With a fixed effect model, results showed a significant improvement in pain with US-guided DN (p<0.001) with a SMD of 0.96 (95% CI: 0.66, 1.27; I2=31.23).
Disability
The standardized mean difference of disability before and after treatment in the short term (<12 weeks) was presented in a forest plot in Figure 3. Pang, et al. [17] used the Knee Injury and Osteoarthritis Outcomes Score (KOOS) subscales of pain, symptoms, and quality of life (QoL), while Sharif, et al. [16] used the KOOS total score to measure the treatment effect of US-guided DN on disability. On the other hand, Tabatabaiee, et al. [24] used the Oswestry Disability Index (ODI) for disability. Huang, et al. [25] did not report any outcomes regarding disability. With a fixed effects model, results showed a significant improvement in disability with US-guided DN (p<0.001) with a SMD of 0.85 (95% CI: 0.61, 1.09; I2=30.89).
![Figure 3: Pang, et al. [17] used the Knee Injury and Osteoarthritis Outcomes Score (KOOS) subscales of pain, symptoms, and quality of life (QoL), while Sharif, et al. [16] used the KOOS total score to measure the treatment effect of US-guided DN on disability. On the other hand, Tabatabaiee, et al. [24] used the Oswestry Disability Index (ODI) for disability. Huang, et al. [25] did not report any outcomes regarding disability. With a fixed effects model, results showed a significant improvement in disability with US-guided DN (p<0.001) with a SMD of 0.85 (95% CI: 0.61, 1.09; I2=30.89).](/fulltextimages/11301/fig_3.png)
Publication Bias Analysis
The funnel plots of the outcomes of pain and disability are documented in Supplementary Figure 1. Both outcomes had symmetric funnel plots, and the results of Egger’s test showed no significant publication bias (pain: p=0.068; disability: p=0.604).
Sensitivity Analysis
The leave-out-one sensitivity analysis was used to examined the robustness of results. The stepwise exclusion of each study had no impact on the results. More details were provided in Supplementary Table 6.
Discussion
The results of this meta-analysis suggest that US- guided DN is more effective in reducing pain and disability than control or no intervention in the treatment of painful musculoskeletal conditions with high quality evidence. In a short-term follow-up period (<12 weeks), the treatment effects were measured by VAS for pain and KOOS and ODI for disability and showed significant improvement in reducing pain (p<0.001) and disability (p<0.001). To the best of our knowledge, this meta-analysis is the first to investigate US-guided DN compared to control or no intervention for treating painful musculoskeletal conditions. However, our meta-analysis only supports short-term treatment effects, as there are a lack of studies that examine the long-term treatment effects of US-guided DN. As a result, caution in the interpretation of the results is warranted.
The findings of this meta-analysis are in agreement with those of previous similar reviews of DN in treating painful musculoskeletal conditions [10, 11, 25, 26, 27]. DN is superior to no treatment of sham needling in reducing pain in the immediate and short-term [10]. In addition, the treatment effects of US-guided DN are larger than DN alone for reducing pain and disability as the physiotherapist is able to visualize the anatomical structure that may be the cause of the patients’ symptoms and disability using US-guidance [16]. Conventionally, the selection of puncture sites are determined by the physiotherapist during physical examination with patient’s symptoms and the identification of myofascial trigger points (MTrPs) [16]. During needle advancement, once a desired local twitch response (LTR) has been obtained, the physiotherapist usually manipulates the needle in a piston-like motion at that layer. Yet, the depth of needle puncture maybe misguided by a LTR that occurred before the needle reaches the problematic structure. Moreover, a LTR may happen at a depth that the advancement of needle must be stopped, yet the problematic structure is located within a deeper layer, with signs of pain hidden from deeper structure, such as joint capsule, articular ligament, hyaline cartilage, or articular retinaculum [16]. Heterogeneous echogenicity, which can indicate mucoid degenerative change, musculoskeletal conditions, and/or a superimposed interstitial tear often appear in ultrasound imaging in painful musculoskeletal conditions [16]. Additionally, the presence of calcium pyrophosphate dihydrate crystals may be indicated by the present of hyperechoic foci in ultrasound imaging [16]. US-guidance in DN can provide an initial awareness of an anatomical abnormality in painful musculoskeletal conditions. Pang, et al. [17] suggested the puncture site can be chosen for US-guided DN if the abnormal sonographic finding matches the symptoms and physical examination of the patient. Consequently, the addition of US-guidance to DN improved the accuracy of needle puncturing into and out of the targeted problematic tissue and allowed for better visualization of the needles’ advancement than traditional DN.
In this meta-analysis, the treatment effects of US- guided DN were compared to those of pharmacotherapeutic intervention for postherpetic neuralgia mixed with myofascial pain syndrome, traditional physiotherapy for jumper’s knee, no-treatment control for piriformis syndrome, and exercise therapy and care education for knee osteoarthritis, with results showing positive treatment effects in reducing pain and disability. Our results also showed low heterogeneity (I2<50%) among the four included studies, indicating low diversity of outcomes and constant effectiveness of US- guided DN on various painful musculoskeletal conditions. Moreover, Huang, et al. [25] and Pang, et al. [17] reported no adverse effects of US-guided DN, Sharif, et al. [16] did not mention any adverse effects, and Tabatabaiee, et al. [24] reported two participants experienced adverse effects during US-guided DN, including pain and bleeding. As a result, US-guided DN is a safe and effective passive treatment modality that decreases musculoskeletal pain and is an ideal addition to physiotherapy treatment that facilitates active functional training to maximize recovery and minimize patients’ disability.
Limitations
Only short-term treatment effects of US-guided DN on painful musculoskeletal conditions were found in the studies included in this meta-analysis. There is a lack of studies indicated long-term treatment effects of US-guided DN. US- guided DN’s efficacy in treating painful musculoskeletal conditions was therefore unknown. We also searched six scientific databases without regard to language. As a result, our findings ought to cover the majority of pertinent published studies. However, it was inevitable that some pertinent studies might have been overlooked. We manually searched the reference lists of all relevant studies in an effort to reduce the likelihood of missing any studies. As a result, we believed that the number of studies missed in our review was small and had little effect on our findings. Yet, we only identified four high-quality studies that investigated the treatment effect of US-guided DN on painful musculoskeletal conditions. However, our results showed low heterogenicity (I2<50%) among the four included studies, indicating consistency of results and efficacy of US-guided DN over those painful musculoskeletal conditions. Yet, four studies with different painful musculoskeletal conditions may not be adequate for generalization of results to other painful musculoskeletal conditions. In addition, publication bias can exaggerate treatment effects when none exist. This meta- analysis showed symmetrical funnel plots and a negative Egger’s test, which are indications of no publication bias. The number of studies identified in this systematic review was so limited, subgroup analysis could not be done, therefore, the subgroup difference of the effects of USDN cannot be evaluated. For example, the effects of USDN in younger people and older people may be different as the healing shoulder be faster in younger people. More studies of USDN on different musculoskeletal conditions in younger and older people are necessary in the future.
Conclusion
Painful musculoskeletal conditions causing pain and disability are growing in the aging population around the world. US-guided DN is a safe and effective treatment modality for reducing pain and disability for painful musculoskeletal conditions in the short-term. However, only a limited, high- quality study examined the effectiveness of US-guided DN over various painful musculoskeletal conditions. In addition, scanty studies have assessed the treatment effect of US- guided DN on painful musculoskeletal conditions over the long-term. As a result, further high-quality studies that focus on the long-term treatment effects of US-guided DN on various painful musculoskeletal conditions are warranted.
- Data Availability The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/ Supplementary Material. The Supplementary Material for this article can be found online at: https://osf.io/mgtnr/. DOI 10.17605/OSF.IO/MGTNR
- Funding Funded by Research Rehab Centre
References
-
Briggs AM, Woolf AD, Dreinhöfer K, Homb N, Hoy DG, et al. (2018) Reducing the global burden of musculoskeletal conditions. Bull World Health Organ 96(5): 366-368.
-
(2022) Musculoskeletal health, World Health Organizatio.
-
Kelsey JL, White 3rd A, Pastides H, Bisbee GE (1979) The impact of musculoskeletal disorders on the population of the United States. JBJS 61(7): 959-964.
-
Woolf AD, Pfleger B (2003) Burden of major musculoskeletal conditions. Bull World Health Organ 81(9): 646-656.
-
Jordan KP, Jöud A, Bergknut C, Croft P, Edwards JJ, et al. (2014) International comparisons of the consultation prevalence of musculoskeletal conditions using population-based healthcare data from England and Sweden. Ann Rheum Dis 73(1): 212-218.
-
Pai MYB, Toma JT, Kaziyama HHS, Listick C, Galhardoni G, et al. (2021) Dry needling has lasting analgesic effect in shoulder pain: A double-blind, sham-controlled trial. Pain Reports 6(2): 939.
-
Zhuang X, Tan S, Huang Q (2014) Understanding of myofascial trigger points. Chin Med J 127(24): 4271- 4277.
-
Cagnie B, Barbe T, De Ridder E, Oosterwijck JV, Cools A, et al. (2012) The influence of dry needling of the trapezius muscle on muscle blood flow and oxygenation. J Manipulative Physiol Ther 35(9): 685-691.
-
Hsieh YL, Hong CZ, Liu SY, Chou LW, Yang CC, et al. (2016) Acupuncture at distant myofascial trigger spots enhances endogenous opioids in rabbits: a possible mechanism for managing myofascial pain. Acupunct Med 34(4): 302-309.
-
Shah JP, Gilliams EA (2008) Uncovering the biochemical milieu of myofascial trigger points using in vivo microdialysis: an application of muscle pain concepts to myofascial pain syndrome. Journal of Bodywork and Movement Therapies 12(4): 371-384.
-
Gattie E, Cleland JA, Snodgrass S (2017) The effectiveness of trigger point dry needling for musculoskeletal conditions by physical therapists: a systematic review and meta-analysis. J Orthop Sports Phys Ther 47(3): 133-149.
-
Sánchez-Infante J, Navarro-Santana MJ, Bravo-Sanchez A, Jiménez Diaz F, Abián-Vicén J (2021) Is dry needling applied by physical therapists effective for pain in musculoskeletal conditions? A systematic review and meta-analysis. Phys Ther 101(3): pzab070.
-
Ughreja RA, Prem V (2021) Effectiveness of dry needling techniques in patients with knee osteoarthritis: A systematic review and meta-analysis. J Bodyw Mov Ther 27: 328-338.
-
Secorro N, Guerra R, Labraca X, Lari M, Pecos D, et al. (2019) Clinical criteria for the application of dry needling in myofascial pain Syndrome: An expert consensus document and a cross-sectional study among physical therapists. Revista Fisioterapia Invasiva/Journal of Invasive Techniques in Physical Therapy 2(02): 050-054.
-
Ebrahimi Takamjani I, Ezzati K, Khani S, Sarrafzadeh J, Tabatabaei A (2020) The Effects of Ultrasound-guided Dry Needling on Patients With Myofascial Pain Syndrome. Iranian Rehabilitation Journal 18(4): 369-176.
-
Sharif F, Ahmad A, Gilani SA (2023) Effectiveness of ultrasound guided dry needling in management of jumper’s knee: a randomized controlled trial. Sci Rep 13(1): 4736.
-
Pang J, Fu A, Lam S, Fu ACL (2022) Effectiveness of ultrasound-guided dry needling in physiotherapy management of knee osteoarthritis: A randomized, double-blinded and controlled study. Physiotherapy 114(1): 176-177.
-
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, et al. (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International Journal of Surgery 88: 105906.
-
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, et al. (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA 283(15): 2008-2012.
-
Woolf AD, Vos T, March L (2010) How to measure the impact of musculoskeletal conditions. Best Prac Res Clin Rheumatol 24(6): 723-732.
-
(1999) PEDro Scale, Physiotherapy Evidence Database.
-
Granholm A, Alhazzani W, Møller MH (2019) Use of the GRADE approach in systematic reviews and guidelines. Bri J Anaesth 123(5): 554-559.
-
Paci M, Matulli G, Baccini M, Rinaldi LA, Baldassi S, et al. (2010) Reported quality of randomized controlled trials in neglect rehabilitation. Neurol Sci 31(2): 159-163.
-
Tabatabaiee A, Ebrahimi-Takamjani I, Ahmadi A, Sarrafzadeh J, Emrani A (2019) Comparison of pressure release, phonophoresis and dry needling in treatment of latent myofascial trigger point of upper trapezius muscle. J Back Musculoskelet Rehabil 32(4): 587-594.
-
Huang Y, Gao M, Li Q, Zhang X, Chen H, et al. (2022) Ultrasound-Guided Dry Needling for Trigger Point Inactivation in the Treatment of Postherpetic Neuralgia Mixed with Myofascial Pain Syndrome: A Prospective and Controlled Clinical Study. Pain Res Manag 2022: 2984942.
-
Butts R, Dunning J, Serafino C (2021) Dry needling strategies for musculoskeletal conditions: Do the number of needles and needle retention time matter? A narrative literature review. J Bodyw Mov Ther 26: 353-363.
-
Navarro-Santana MJ, Gómez-Chiguano GF, Cleland JA, Arias Buria JL, Fernández-de-Las-Peñas C, et al. (2021) Effects of trigger point dry needling for nontraumatic shoulder pain of musculoskeletal origin: A systematic review and meta-analysis. Phys Ther 101(2): pzaa216.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial