Pain Neuroscience Education for Occupational Therapy Students: An Exploratory Online and In-Person Multi-Site Study
Background: Educating occupational therapy (OT) students in pain science is essential to align with biopsychosocial treatment models and multidisciplinary approaches. This knowledge equips them to tackle the pain and opioid epidemic in clinical practice. This study aimed to evaluate if a pain neuroscience education (PNE) lecture for OT students produced immediate positive shifts and whether these changes correlated with those observed in physical therapy and physician assistant students. Methods: This case series involved 120 OT students from four United States (US) schools who participated in a two-hour PNE lecture, delivered in-person or online. Pre- and post-lecture assessments included the revised neurophysiology of pain questionnaire (rNPQ), Likert Scale questions on pain beliefs, and the pain attitudes and beliefs scale (biomedical) PABS-BM and pain attitudes and beliefs scale (biopsychosocial) PABS-BPS to evaluate changes in pain knowledge and attitudes. Results: Data collected from 120 OT students enrolled in four entry-level OTD programs yielded significant changes in rNPQ (p
Abbreviations
COVID-19: Corona virus disease of 2019; HC-PAIRS: Health Care Provider’s Pain and Impairment Relationship Scale; NPQ: Neurophysiology of pain questionnaire; OT: Occupational therapy; OTD: Occupational therapy doctorate; PABS: Pain attitudes and beliefs scale; PABS- BM: Pain attitudes and beliefs scale biomedical; PABS-BPS:
Pain attitudes and beliefs scale psychosocial; PNE: Pain neuroscience education; rNPQ: revised neurophysiology of pain questionnaire; US: United States.
Introduction
Epidemiological data indicates that one in four people in the United States (US) suffers from some form of persistent pain, with musculoskeletal pain representing 70% of this total [1]. Alarmingly, the data shows that the pain epidemic has nearly doubled in the last three decades [1, 2], and more recently it has been postulated that the corona virus disease of 2019 (COVID-19) will not only increase the rate of persistent pain, but also intensify the overall pain experience of those already challenged by persistent pain [3, 4]. A very troubling consequence of the pain epidemic is the resulting US opioid epidemic. In 2016, healthcare providers across the US wrote more than 214 million prescriptions for opioid pain medication-a rate of 66.5 prescriptions per 100 people [5]. As many as 1 in 5 people receive prescription opioids long-term for non-cancer pain in primary care settings, and every day, more than 1,000 people are treated in emergency departments for misusing prescription opioids [5, 6].
The enormity of the pain and opioid epidemic clearly indicates that one approach and one profession does not have the answer. Given the complexity of the human pain experience, a multi-disciplinary, biopsychosocial approach is needed to help curb the pain epidemic [7, 8]. In rehabilitation, based on the current best-evidence, it is well established that treatment for pain, especially persistent pain, must focus on three key elements - cognitive treatment, movement, and strategies to calm down the central and peripheral nervous system [8, 9, 10, 11]. In physical therapy, a cognitive treatment specifically aimed at helping people with persistent pain and targeting all three categories, has emerged in the last 20 years, referred to as pain neuroscience education (PNE) [12, 13]. PNE is an educational strategy that focuses on teaching people more about the neurobiological and neurophysiological processes involved in their pain experience [14, 15]. Current best-evidence regarding musculoskeletal pain provides strong support for PNE to positively influence pain ratings, dysfunction, and limitations in movement, pain knowledge, and healthcare utilization [14, 16, 17]. Additionally, PNE has shown to powerfully influence psychosocial issues that powerfully influence pain and depression: fear-avoidance and pain catastrophizing [14, 18].
The mandate of the persistent pain and opioid epidemic does not only call for evidence-based biopsychosocial approaches, but also multidisciplinary and interdisciplinary care [19, 20]. In this approach, various healthcare providers bring their unique vantage points and strengths to the problem at hand, including a person struggling with persistent pain. This approach, however, requires all healthcare providers to follow an evidence-based, standardized approach, including a uniform message around pain [19, 21, 22]. To this effect, PNE research has since branched into various non-physical therapy studies, including multidisciplinary audiences. For example, Louw, et al. showed that a PNE lecture to 270 healthcare providers resulted in positive changes in pain knowledge, attitudes, and beliefs regarding pain and self- reported changes in clinical behavior one year later [21]. Similarly, it has been shown that physician assistant students learning more about pain increased their knowledge of pain, attitudes, and beliefs about pain, and shifted from a predominant focus on medication to treat pain toward a more holistic approach that includes non-pharmacological ways to treat pain [22, 23]. In occupational therapy (OT), very little research specific to PNE is available. In various multidisciplinary studies, OTs are represented in the studies but not specifically aimed at them [21, 24]. In a recent OT- led study, it was shown that PNE delivered to nurses by an OT in an inpatient rehabilitation facility powerfully shifted nurses to offer patients more non-pharmacological ways to ease their pain [25].
A key element of the current PNE push is training students to equip them with tools when they enter clinical practice and face the pain and opioid epidemic. To date, PNE research has been conducted on physical therapy students and physician assistant students [22, 23, 26], but not OT students. Student studies show positive effects on students following a PNE lecture, including increased knowledge of pain, healthier attitudes and beliefs about pain, as well as increased aptitude for non-pharmacological treatments for pain [22, 23, 26]. More recently, in line with the International Association for the Study of Pain guidelines, OT research has shifted towards pain science, PNE, and OT pain curriculums, showing a need to advance strategies such as PNE in OT schools [27, 28]. The aim of this study was to determine if a PNE lecture, delivered to OT students, yields any immediate post-education positive shifts and if these changes correlate to changes seen in physical therapy and physician assistant students.
Methods
Participants and Procedure
Participants consisted of a convenience sample of entry-level or post-professional OTD students from four participating universities. Institutional review board approval was obtained from the University of Southern Indiana. No personal identifiable information was collected and participation in the study was entirely voluntary.
Educational Protocol
The content of the lecture has been used in previous PNE physical therapy and physician assistant student studies described elsewhere [22, 23, 26]. In short, the OT lecture was a 2-hour lecture using PowerPoint™ to teach OT students about the neurophysiology and neurobiology of pain. The lecture covered content regarding challenges with current biomedical approaches to treating persistent pain and updated neuroscience of pain information (ion channels, nociceptive input, dorsal horn wind-up, neuronal facilitation/inhibition, pain matrix, environmental and stress effects on pain perception) [23, 29]. The content focused on pain neuroscience and did not cover any content specific to the pre- and post-education questionnaire. The 2-hour lecture was chosen due to its ability to positively change pain knowledge, attitudes, and beliefs regarding pain and fit into class schedules. The lecture was delivered by clinicians and educators with advanced post-professional training in PNE. Education was delivered either via an online synchronous, online session or via onsite live lecture.
Instrument
In line with the aim of the study, students completed a series of pre- and immediately post PNE surveys:
Demographic Survey (Only prior to PNE): Students were required to complete a demographic survey containing items (i) that aid in describing the cohort of students and (ii) capture relevant variables that may correlate to their pre- and post- PNE survey results. No personal identifiable information was collected, and included age, gender, ethnicity, and pain experience.
Pain Knowledge: Pain knowledge was measured using the revised neurophysiology of pain questionnaire (rNPQ). The rNPQ is based on a current pain science text and was used in a previous study measuring the neurophysiology knowledge of patients and healthcare personnel [24, 30]. No data is available in patients or healthy controls as to what constitutes a meaningful shift. Adult studies (ages 18 and above) have shown rNPQ mean improvements after a PNE session to typically range between 25-30% [15, 24, 31].
Pain Beliefs: Healthcare provider’s attitudes and beliefs regarding persistent pain are often measured with the Health Care Provider’s Pain and Impairment Relationship Scale (HC- PAIRS) [32]. Upon review of the HC-PAIRS and the aims of the study, a series of numeric rating scale questions pertaining to beliefs about pain were established by the authors for this study and used in previous studies [21, 22]. The numeric rating scale is anchored between 0 (strongly disagree) and 10 (strongly agree). Five questions were established to allow surveys to be completed prior to and following the PNE session in the allotted time. Beliefs statements were:
- Pain is normal; without being able to feel pain you will not survive.
- Pain means something is wrong with your tissues.
- Pain always means you have to stop what you are doing.
- You can control how much pain you feel.
- Your brain decides if you feel pain, not your tissues.
Pain Attitudes and Beliefs (Pain Attitudes and Beliefs Scale - PABS): The PABS is a self-administered instrument developed to discriminate between a predominantly biomedical and bio-psychosocial treatment orientation of healthcare providers towards low back pain management [33]. A characteristic of a biomedical orientation is the belief that pain, and disability are the consequence of specific pathology or tissue damage, and that treatment is therefore aimed at signs and symptoms of pathology. Indicative for a bio-psychosocial orientation is the belief that pain and disability are not necessarily signs of tissue damage but can be influenced by psychological and social factors [34]. Responders indicate on a 6-point Likert scale (1 = totally disagree, 6 = totally agree) their endorsement on each statement. Treatment orientation is measured on two sub- scales, labelled ‘biomedical’ and ‘biopsychosocial.’ Sub-scale scores are calculated by a simple summation of the responses to the sub-scale items. Higher scores on a sub-scale indicate a stronger treatment orientation [35]. A statistical difference and shift of 2.0 points on the biomedical and 1.5 points on the biopsychosocial scales have been reported as being meaningful [35].
Statistical Analysis
Means, counts, and standard deviations were used as summary statistics in examining demographic information of the study cohort. Missing values for rNPQ, Pain Beliefs, and PABS were inputted using overall group median values. To assess whether values for each measure of rNPQ, Pain Beliefs, or PABS (both biomedical and psychosocial) varied across sites, eight separate Levene tests were conducted at the a = 0.05 significance level, as well as eight separate Shapiro- Wilks tests for normality at the same level of confidence. To test for meaningful differences between pre/post scores for rNPQ, a Wilcoxon signed rank test was used at the a = 0.05 confidence level. Pre/post differences for PABS-BM and PABS-BPS were evaluated using a paired t-test at the a = 0.05 confidence level with a Bonferroni correction such that each PABS measurement was tested at the a = 0.025 level of confidence. Differences in the five statements regarding pre/ post pain beliefs were assessed with the Wilcoxon test at the a = 0.05 confidence level (each statement evaluated at a = 0.01 with a Bonferroni correction). To evaluate whether these differences varied across research sites, a single one- way ANOVA was used at the a = 0.05 confidence level.
Results
Participants
In all, 120 OT students participated in the study and provided demographic information (Table 1).
| Variable | Result |
|---|---|
| Age - years (Mean and SD) | 24.2 (3.38) |
| Female gender (%) | 105 (87.5) |
| Ethnicity (%) White, Caucasian Hispanic Asian Other African American Not answered | 98 (81.7) 8 (6.7) 7 (5.8) 3 (2.5) 2 (1.7) 2 (1.7) |
| Currently experiencing pain (%) | 32 (26.7) |
| Mean self-reported pain rating for those experiencing pain (Numeric pain rating scale) | 1.29 |
| Experienced pain within the last 6 months (%) | 82 (68.3) |
| Know someone personally with chronic pain (%) | 69 (57.5) |
Table 1: Participant demographics.
Pain Knowledge
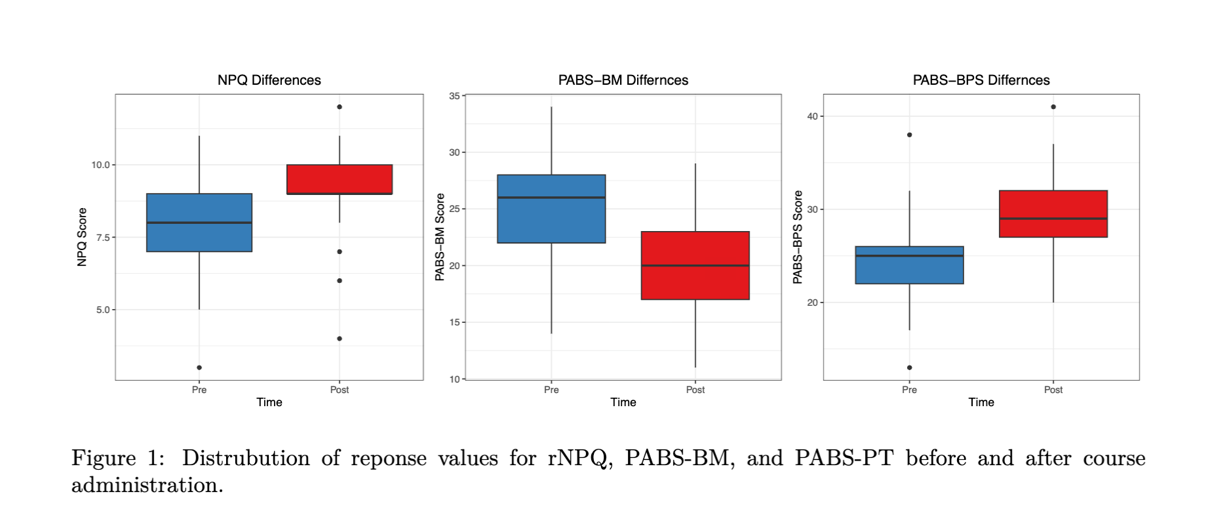
Mean rNPQ scores shifted from 7.77 pre-PNE to 9.32 post-PNE (p < 0.001), increasing pain knowledge by 12.9% (Figure 1) (Table 2).
Pain Attitudes and Beliefs
Biomedical beliefs associated with pain decreased from 25.1 prior to PNE, to 20.01 following the PNE lecture (p < 0.001) (Figure 1) (Table 2). Conversely, biopsychosocial beliefs increased from 24.3 prior to the PNE lecture to 29.42 following the lecture (p < 0.001) (Figure 1, Table 2).
| Outcome measures | Mean pre-PNE score | Mean post-PNE score | Difference | |
|---|---|---|---|---|
| Pain knowledge (rNPQ) | 7.77 | 9.32 | <0.001 | |
| Pain attitude and beliefs - biomedical (PABS-BM) | 25.09 | 20.01 | <0.001 | |
| Pain attitudes and beliefs - psychosocial (PABS-BPS) | 24.26 | 29.42 | <0.001 | |
| Pain belief | Mean pre-score | Mean post-score | Difference | p |
| Pain is normal; without being able to feel pain you will not survive. | 7.07 | 7.78 | 0.71 | 0.03 |
| Pain means something is wrong with your tissues. | 4.65 | 3.56 | -1.09 | 0.002 |
| Pain always means you have to stop what you are doing. | 2.64 | 1.25 | -1.38 | < 0.001 |
| You can control how much pain you feel. | 4.41 | 6.19 | 1.78 | < 0.001 |
| Your brain decides if you feel pain, not your tissues | 5.6 | 8.26 | 2.66 | < 0.001 |
Table 2: Differences in outcome measures before and after the PNE lecture.
Pain Beliefs
Average pain belief ratings increased for statements 1, 4, and 5. For statements 2 and 3, the average level of agreement decreased. The largest change in pain beliefs was in statement 5: “Your brain decides if you feel pain, not your tissues.” with participants increasing level of agreement by an average of 2.66 points (Table 3).
Online Versus In-Person Training
A one-way ANOVA was performed to see if changes in rNPQ and PABS vary across data collection sites. No site was found to be statistically significantly different from the others in relation to their changes in rNPQ, PABS, or Pain Beliefs (p > 0.05 for all tests on 3 d.f.), indicating comparable results for online, synchronous delivery of PNE and live, in-person training (Figure 2).
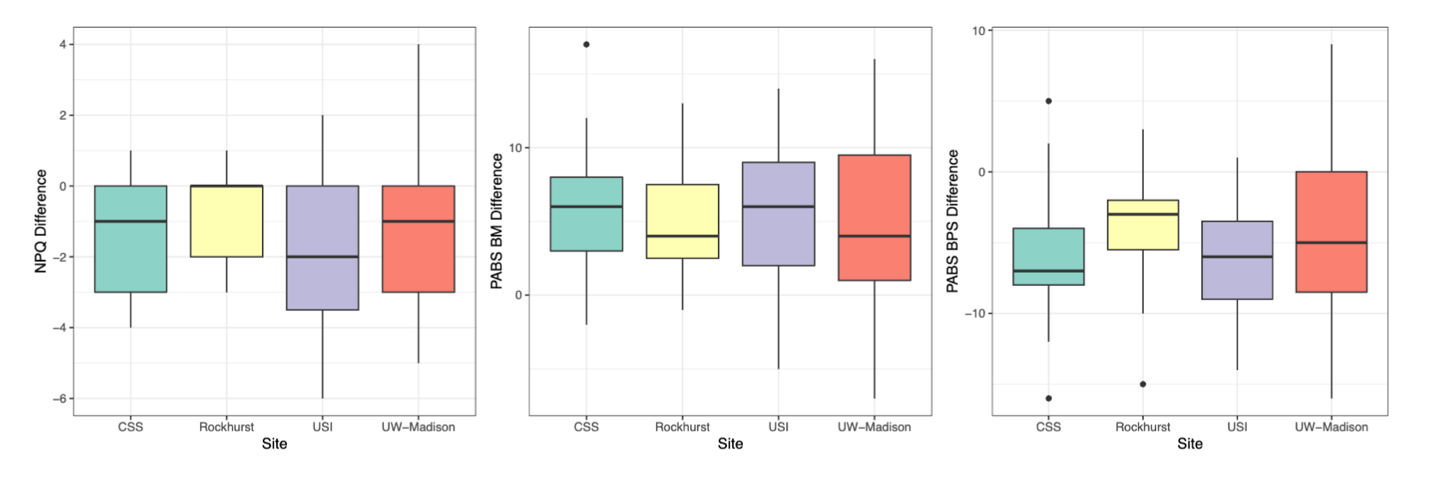
A post-hoc power analysis was conducted to determine statistical power in our results based on sample and calculated effect size. Results reported high statistical power near 1, indicating that these results are likely to be replicated in a larger sample, and can be considered generalizable to the study population.
Discussion
To our knowledge, this is the first study exploring the effect of PNE training for OT students. The results indicate that a one-time, live, in-person or online lecture on PNE results in significant improvements in OT students’ knowledge of pain and beliefs regarding pain, shifting them from a biomedical approach to a biopsychosocial approach toward people in persistent pain. The increase in pain knowledge in this study is consistent with various other healthcare provider studies indicating a PNE lecture’s ability to improve pain knowledge [24, 26]. To date, this has not been studied in OT students but rather in OT clinicians [22, 24]. In this study, pain knowledge increased by 12.9%, whereas the original physical therapy student study showed an increase of 45.7% [26]. It is important to note that the physical therapy student study used the original NPQ tool, which has since been altered to deliver a more accurate tool (rNPQ), which was used in this study. More importantly, the OT student pre-PNE pain knowledge starting score was already much higher (64.2%) compared to the starting point for the OT students, yielding a ceiling effect as seen in these results. Regarding practicing OTs, the student improvement in pain knowledge concurs with previous studies showing an ability to improve pain knowledge following a PNE lecture. This increase in pain knowledge for OT students is important, since it has been shown that improved pain knowledge is tied to healthier attitudes, increased compassion, and empathy toward patients with persistent pain [36]. This concurs with the additional results from this study indicating significant positive shifts in beliefs regarding persistent pain after the PNE lecture. Furthermore, increased pain knowledge, facilitated by a PNE lecture, has been tied to actual and self- reported improvements in patient outcomes [36, 37].
This study showed that OT students learning more about PNE shift from a biomedical to a biopsychosocial attitude and belief when it comes to persistent pain. This is critical since current best evidence strongly supports the use of a biopsychosocial model for persistent pain [8]. Persistent pain is complex and a powerful interplay between biological, psychological, and social factors and must be seen as such and addressed as such to truly impact the current pain epidemic. In fact, it has been demonstrated that a stringent biomedical model and approach to pain is a big driving force behind the pain epidemic, opioid epidemic, and over- medicalization of persistent pain [7, 38]. Biomedical models, which only tie the health of a person’s tissue to their pain, fuel increased use of imaging and invasive techniques aiming to restore these biomedical issues, often ignoring powerful psychosocial contributions to a persistent pain experience. The results from this study, specific to OT students, are important since they allow early-career clinicians the ability to enter the workforce with a more robust, well-rounded, and evidence-based approach to persistent pain [27, 28]. Additionally, for OTs to rightfully take their place in a much- needed multi- and interdisciplinary team treating persistent pain, a stronger biopsychosocial approach is needed.
A third, and significant, additional finding of the study is the fact that PNE delivered online provided similar results to live, in-person sessions. This allows for strategies to disseminate PNE content more readily to OT schools all over the US, and even internationally. With PNE in its relative infancy in OT, the ability to spread this message to more schools will allow a speedier adoption of the International Association for the Study of Pain guidelines via online, synchronous sessions. The study contains numerous limitations. First, it only provides immediate post-education results, which do not show long-term changes or retention. Second, and most importantly, a missed opportunity was to obtain student feedback on the PNE program.
Conclusion
A PNE lecture to OT students, results in increased knowledge of pain, healthier beliefs regarding persistent pain and a shift from a biomedical attitude and belief to a more well-rounded biopsychosocial attitude and belief. This education can be delivered live online or in-person. The PNE results from this OT study concur with studies in other healthcare professions, underscoring the need for a unified approach to pain, especially chronic pain. With the OT profession adopting the International Association for the Study of Pain guidelines, additional research should be undertaken in regard to PNE for OT students and clinicians.
References
-
Şentürk İA, Şentürk E, Üstün I, Gökçedağ A, Yıldırım NP, et al. (2023) High-impact chronic pain: evaluation of risk factors and predictors. Korean J Pain 36(1): 84-97.
-
Woolf AD, Pfleger B (2003) Burden of major musculoskeletal conditions. Bull World Health Organ 81(9): 646-656.
-
Clauw DJ, Häuser W, Cohen SP, Fitzcharles MA (2020) Considering the potential for an increase in chronic pain after the COVID-19 pandemic. Pain 161(8): 1694-1697.
-
Louw A (2020) Letter to the editor: chronic pain tidal wave after COVID-19: are you ready? Physiother Theory Pract 36(12): 1275-1278.
-
Tong ST, Hochheimer CJ, Brooks EM, Sabo RT, Jiang V, et al. (2019) Chronic Opioid Prescribing in Primary Care: Factors and Perspectives. Ann Fam Med 17(3): 200-206.
-
Florence CS, Zhou C, Luo F, Xu L (2016) The Economic Burden of Prescription Opioid Overdose, Abuse, and Dependence in the United States, 2013. Med Care 54(10): 901-906.
-
Jull G (2017) Biopsychosocial model of disease: 40 years on. Which way is the pendulum swinging? Br J Sports Med 51(16): 1187-1188.
-
Zimney K, Bogaert WV, Louw A (2023) The Biology of Chronic Pain and Its Implications for Pain Neuroscience Education: State of the Art. J Clin Med 12(13): 4199.
-
Bernardy K, Klose P, Busch AJ, Choy EH, Häuser W (2013) Cognitive behavioural therapies for fibromyalgia. Cochrane Database Syst Rev 9: CD009796.
-
Larun L, Brurberg KG, Odgaard-Jensen J, Price JR (2019) Exercise therapy for chronic fatigue syndrome. Cochrane Database Syst Rev 10(10): CD003200.
-
Nijs J, Wijma AJ, Willaert W, Huysmans E, Mintken P, et al. (2020) Integrating Motivational Interviewing in Pain Neuroscience Education for People with Chronic Pain: A Practical Guide for Clinicians. Phys Ther 100(5): 846- 859.
-
Moseley L (2002) Combined physiotherapy and education is efficacious for chronic low back pain. Aust J Physiother 48(4): 297-302.
-
Moseley GL (2003) Joining forces - combining cognition- targeted motor control training with group or individual pain physiology education: a successful treatment for chronic low back pain. Journal of Manual & Manipulative Therapy 11(2): 88-94.
-
Louw A, Zimney K, Puentedura EJ, Diener I (2016) The Efficacy of Therapeutic Neuroscience Education on Musculoskeletal Pain - A Systematic Review of the Literature. Physiotherapy Theory and Practice 32(5): 332-355.
-
Meeus M, Nijs J, Oosterwijck JV, Alsenoy VV, Truijen S (2010) Pain Physiology Education Improves Pain Beliefs in Patients With Chronic Fatigue Syndrome Compared With Pacing and Self-Management Education: A Double- Blind Randomized Controlled Trial. Arch Phys Med Rehabil 91(8): 1153-1159.
-
Lin LH, Lin TY, Chang KV, Wu WT, Özçakar L (2024) Pain neuroscience education for reducing pain and kinesiophobia in patients with chronic neck pain: A systematic review and meta-analysis of randomized controlled trials. Eur J Pain 28(2): 231-243.
-
Shin S, Kim H (2013) Carryover Effects of Pain Neuroscience Education on Patients with Chronic Lower Back Pain: A Systematic Review and Meta-Analysis. Medicina (Kaunas) 59(7): 1268.
-
Louw A, Wendling E, Hawk D, Sturdevant N, Louw H, et al. (2021) Pain Neuroscience Education for Depression: A Pilot Study. Psychological Disorders and Research 42(2): 1-7.
-
Agarwal V, Louw A, Puentedura EJ (2020) Physician- Delivered Pain Neuroscience Education for Opioid Tapering: A Case Report. Int J Environ Res Public Health 17(9): 3324.
-
Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJ, Ostelo RW, et al. (2015) Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ 350: h444.
-
Louw A, Vogsland R, Marth L, Marshall P, Cox T, et al. (2019) Interdisciplinary Pain Neuroscience Continuing Education in the Veteran’s Affairs: Live Training and Live-Stream with 1-year Follow-up. Clin J Pain 35(11): 901-907.
-
Louw A, Schmieder A, Peppin E, Farrell K, Zimney K, et al. (2020) Can a pain neuroscience edcuation lecture alter treatment choices for chronic pain in physician assistant students? Psychological Disorders and Research 3(2): 1-5.
-
Zimney K, Louw A, Johnson J, Peppers S, Farrell K (2018) Effects of Pain Science Education on Physician Assistant Students Understanding of Pain and Attitudes and Beliefs about Pain. South Dakota Medical Journal 71(11): 506-511.
-
Moseley GL (2003) Unravelling the barriers to reconceptualisation of the problem in chronic pain: the actual and perceived ability of patients and health professionals to understand the neurophysiology. J Pain 4(4): 184-189.
-
Doyle MO, Gustafson B, Louw A, Podolak J (2022) Non-Pharmacological Pain Self-Management in an Inpatient Rehabilitation Setting: An Exploratory Quality Improvement Study. Annals of Physiotherapy and Occupational Therapy 5(2): 1-9.
-
Cox T, Louw A, Puentedura EJ (2017) An Abbreviated Therapeutic Neuroscience Education Session Improves Pain Knowledge in First Year Physical Therapy Students But Does Not Change Attitudes or Beliefs. Journal of Manual & Manipulative Therapy 25(1): 11-21.
-
Lagueux E, Masse J, Pagé R, Marin B, Tousignant- Laflamme Y (2023) Management of Chronic Pain by Occupational Therapist: A Description of Practice Profile. Can J Occup Ther 90(4): 384-394.
-
Rider JV, Khau V, Valdes KA (2024) Survey of Pain Curriculum Among Entry-Level Occupational Therapy Programs in the United States. Journal of Occupational Therapy Education 8(1): 1-25.
-
Moseley GL (2007) Reconceptualising pain according to modern pain sciences. Physical Therapy Reviews 12(3): 169-178.
-
Pietro FD, Catley MJ, McAuley JH, Parkitny L, Maher CG, et al. (2014) Rasch analysis supports the use of the Pain Self- Efficacy Questionnaire. Physical therapy 94(1): 91-100.
-
Oosterwijck JV, Meeus M, Paul L, Schryver MD, Pascal A, et al. (2013) Pain physiology education improves health status and endogenous pain inhibition in fibromyalgia: a double-blind randomized controlled trial. The Clinical journal of pain 29(10): 873-82.
-
Latimer J, Maher C, Refshauge K (2004) The attitudes and beliefs of physiotherapy studetns to chronic back pain. Clinical Journal of Pain 20: 45-50.
-
Bishop A (2010) Pain Attitudes and Beliefs Scale (PABS). J Physiother 56(4): 279.
-
Mutsaers JH, Peters R, Pool-Goudzwaard AL, Koes BW, Verhagen AP (2012) Psychometric properties of the Pain Attitudes and Beliefs Scale for Physiotherapists: a systematic review. Man Ther 17(3): 213-218.
-
Eland ND, Kvåle A, Ostelo RWJG, de Vet HCW, Strand LI (2019) Discriminative Validity of the Pain Attitudes and Beliefs Scale for Physical Therapists. Phys Ther 99(3): 339-353.
-
Louw A, Brette N, Brian F, Terry C (2019) Pain Neuroscience Education for Physiotherapy Receptionists. Pain and Rehabilitation 2019(46): 24-31.
-
Louw A, Puentedura EJ, Denninger TR, Lutz AD, Cox T, et al. (2022) The clinical impact of pain neuroscience continuing education on physical therapy outcomes for patients with low back and neck pain. PLoS One 17(4): e0267157.
-
Nijs J, Roussel N, Wilgen CP, Köke A, Smeets R (2013) Thinking beyond muscles and joints: therapists’ and patients’ attitudes and beliefs regarding chronic musculoskeletal pain are key to applying effective treatment. Man Ther 18(2): 96-102.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial