The Effect of HIV/HPV on the Structure of the Placental Villi
A placenta obtained of patient with co-infection HPV/HIV antiretroviral therapy and serology negative for another illness was analysed with the purpose of demonstrate the effect of this infection on the structure of the placental villi. The features of patient, the diagnostic, methods used, exam of material with H&E stain and sampling was done according morphological criterion of the literature as written in a previous article. Villi with interrumped syncytium are seen communicating the stromal region with the intervillous space. A group of them are associated by fibrinoid deposition, cells of the cellular island lack of cytoplasm, severe changes are observed in stem villi, many placental ramifications are immature, zones of calcification are observed and numerous remainders of villi are noted. The presence of this viral combination has provoked a strong attack to the structure of the villi which put in danger the normal interchange of gases and nutrients in the maternal-fetal intervillous space.
Olivar C Castejon S* and Angela J Lopez G
olivar.ciadanauc@gmail.com gases and nutrients in the maternal-fetal intervillous space.
Keywords: Co-infection HPV/HIV; Histopathological changes; Placental villi
Introduction
The placenta acquires viral infections proceedings from the mother [1]. Extensive microscopic infarction, distal villous hypoplasia, increased syncytial knots, increased perivillous fibrin, stem villous thrombosis, avascular villi, villous stromal kariorrhesis and villitis of unknown etiology has been found in placentas from pregnancies in HIV-infected women [2].
In the cases where placental pathology findings are found among HIV-infected and uninfected women the chorioamnionitis, deciduitis, Hofbauer cell hyperplasia, villitis, villous stromal edema and intravillous hemorrhage are more prevalent in HIV-infected women [3].
Studies suggest that most perinatal immunodeficiency virus (HIV) type 1 infections occur at or near birth [4]. Others indicate that most transmission occurs in utero through transplacental transmission [5]. It is known that placental inflammation increases the risk of vertical HIV transmission [6].
If the placenta is damaged and the blood from the infected mother transfers into the blood circulation of the foetus as occurs in chorioamnionitis there is increased HIV transmission risk. Might be that maternal infected cells travel across the placenta and from here the virus gets to the stromal vessels of the placental villi reaching the foetus. D’Costa, et al. found a non-inflammatory lesion in the pathology of the placenta in HIV infection as cytotrophoblastic hyperplasia and the placental disc did not show any significant decrease in dimensions [7].
Patterson et al presented data to suggest that Leukemia inhibitory factor (LIF) inhibits HIV-1 replication and is upregulated in the placentas of nontransmitters women. LIF, a member of the IL-6 cytokine family has their receptor (LIFR) in the trophoblast and some women that express lower quantities of LIF increase the risk of mother to infant transmission [8].
It would seem that HIV-1 transmission from an infected mother to her infant is the result of a complex interplay between virus and host in which genotypes of virus, mother and infant impact the risk of transmission [9].
Hofbauer cells sequester HIV-1 in intracellular compartments that can be accessed by HIV-1 specific antibodies in the stromal region; activity that may be overridden when a strong association between maternal human cytomegalovirus viremia promotes inflammation, chronic villitis and trophoblast damage provoking no placental protection, facilitating in utero transmission of HIV-1 [10].
Many years ago it was described that the few studies which have reported the histopathology of placentas from HIV seropositive women have failed to demonstrate either villositis or a consistent microscopic lesion [11].
By other hands HPV was associated with chorioamnionitis, lymphohistiocytic villitis, sclerosing villitis, villitis of unknown etiology, perivillous fibrin embracing disintegrated syncytiotropho- blast, fibrosis, vascular obliteration, aggregated villi and syncytium loss [12].
HPV16/18 was detected in 24.4% of placentas from term deliveries by PCR [13]. In a HPV family study this virus was found in mother, neonate and umbilical cord as HPV16, 6, 83 and 39 [14]. Transplacental transmission of HPV was considered when type-specific HPV concordance was found between the mother, the placenta and the newborn or the mother and cord blood in a study where allowed the identification of genotypes 6/11,16,18,31,33,42,52 and 58 [15].
To date, approximately 200 different genotypes of HPVs have been indentified; categorized in the high- risk(HPV16,18,31) and the low-risk types(HPV6,11).Infection with low-risk HPVs usually results in benign epithelial warts, while with the high-risk HPVs can lead to cervical cancer. Infection with HPV may result in death of trophoblasts, malfunction or malignancy and these changes can disrupt the integrity of the trophoblast and cause spontaneous abortions or preterm delivery.HPV infections are more abundant in human HIV- positive pacients [16].
Material and Methods
Placenta was obtained of patient of low socioeconomic recourse with co-infection HPV/HIV, at 38 weeks, who had antiretroviral therapy by human acquired immunodeficiency syndrome using protocol of the group of clinical essay of pediatrics AIDS [17]. PACTG 076 according to sigla in English, indicating 3´Azido 3´deoxythymidine(AZT) as Connor, et al. during the third trimester of pregnancy [18].
The features of patients, their diagnostic, methods used, sampling, examination of placenta infected and control, were described according to morphological criterion of the literature as has been written in preliminar article.
Results
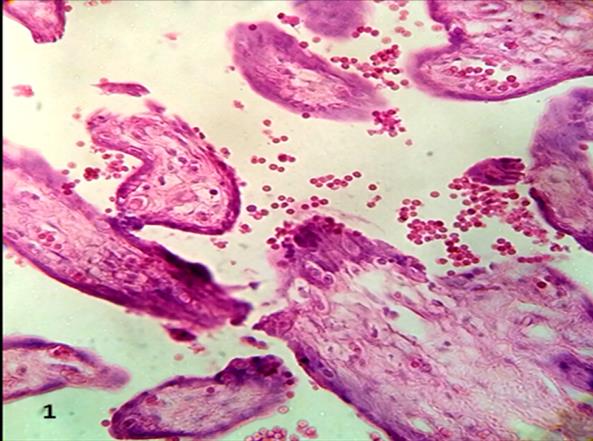
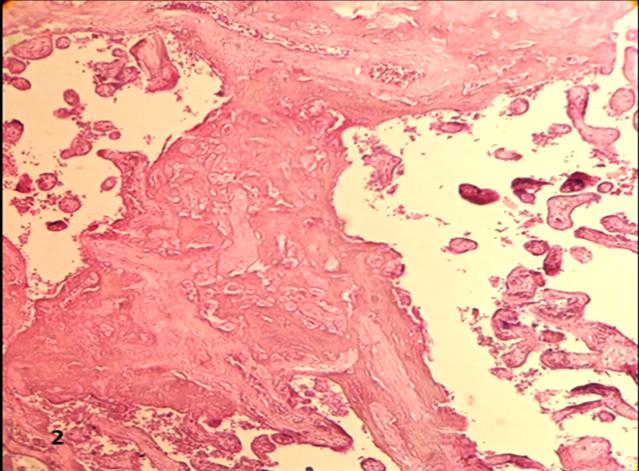
Placental villi were seen with interrumped syncytium suffering necrosis and being very thin. A great deal of them are absent of syncytium and the stromal region is relationed with the intervillous space (Figure 1). Villi that are very near and have lost part of syncytium tend to cellular fusion by means of fibrinoid deposition (Figure 2). Numerous cells of Cellular Island were observed with cytoplasmic lysis (Figure 3).
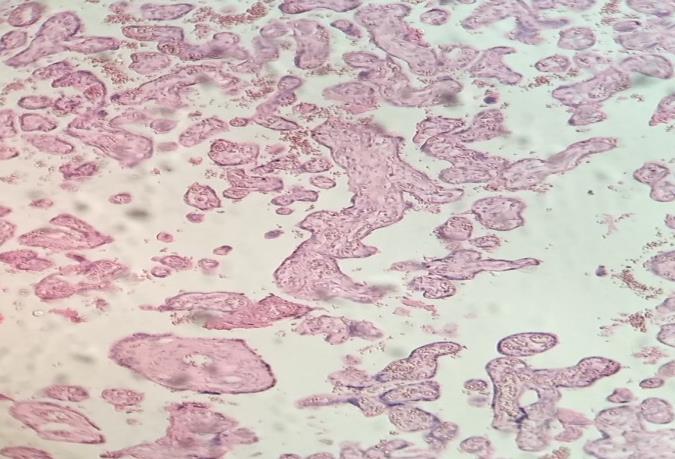
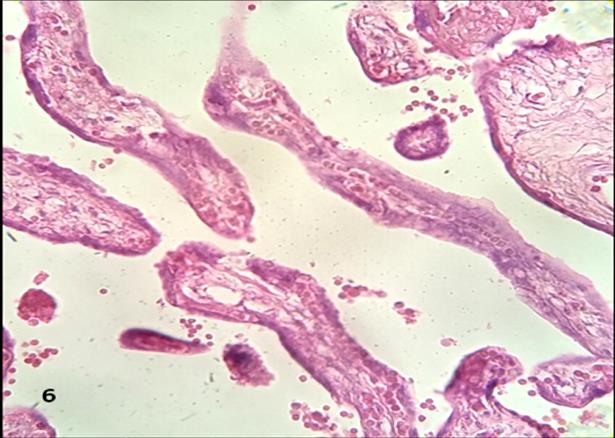
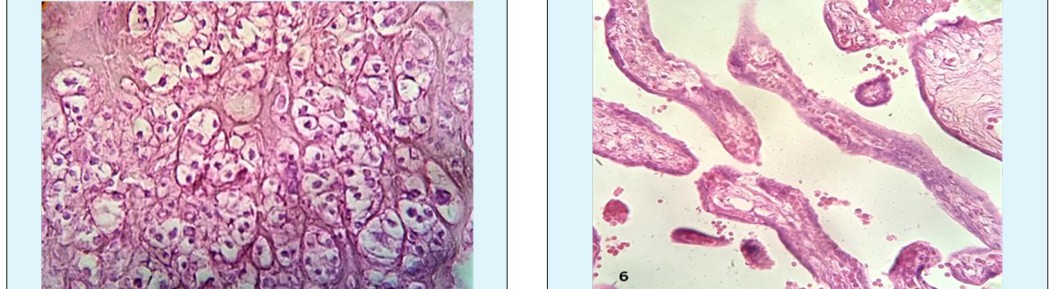
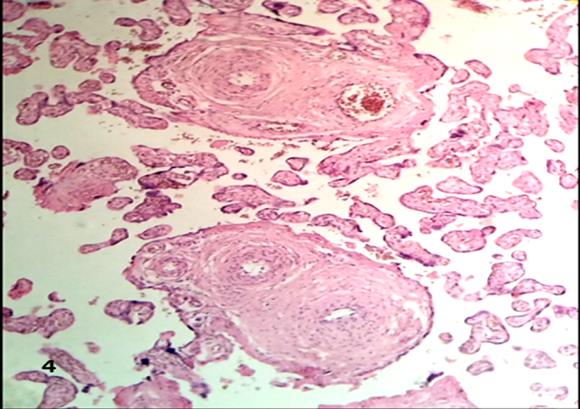
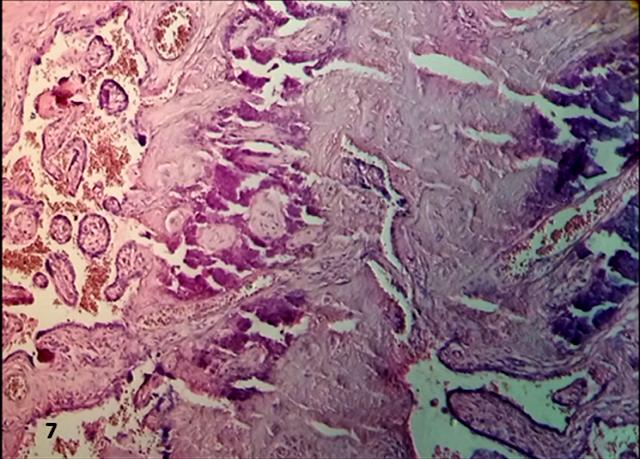
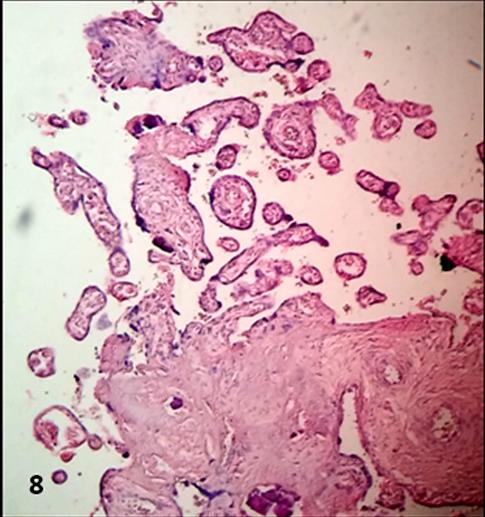
The stems villi were noted with changes in the tunica intima and media of blood vessels. Damaged endothelium and separate muscle cells were observed (Figure 4). Immature ramifications of placental villi persist with frecuency in the observations which not correspond at 38 weeks of pregnancy (Figure 5). Short mature intermediate villi without terminal villi were found with degenerative changes at level of the syncytium (Figure 6). Regions of calcified placental villi can be observed (Figure 7). With frequency debris of stem villi and intermediate villi appeared in the intervillous space (Figure 8).
Discussion
The interruption of the syncytial membrane in presence of HIV/HPV can impede the pregnancy provoking death fetal Replication of HPV is increased in trophoblast cells of HIV patients without inducing an immune response [16]. Oncogenetic human papillomavirus cause squamous intraepithelial lesions and cancer of the uterine cervix in human immunodeficiency virus seropositive women [22].
Similar lesions are also observed in syncytium of placental villi under the influence of HIV. This virus can enhance the risk of HPV infection, promote their latent infection and favour their persistence [23]. We don’t know for example, if HPV16 viral load is provoking the same effect that induces in human uterine cervix associate to cervical dysplasia. However, we in a preliminary study have found stem villi with fibrotic stroma and numerous fibrotic villi that lost their vessels which could to correspond with a process similar to a fibrodysplasia. The stromal tissue of the placental villi is substituted by fibrous tissue [21].
The lost of a region of syncytium in two villi or more that are very near provably produces in them develops of cytotrophoblasts that secrets matrix-type fibrinoid, which represent the glue that guarantees adhesiveness, the re- epithelialization of damaged villous surface by the viruses and the develops of a new villi [19].
The infection by HIV has a cytolitic effect and the infection by HPV has effect of vacuolization of the cytoplasm as vacuolants agents, both viruses have provoked the cytoplasmic lysis observed in cell island [21].
The changes observed in stem villi have contributed with the fibrous tissue noted which were not seen in control placenta. The stem villous thrombosis that occurs in these cases of infection by HIV associate to avascular villi has been inhibiting the normal develop of the placental villi showing an immature tree at term [2].
Zones of calcification have indicated the presences of severe degenerative changes provoked by the activity of HIV/HPV producing a strong destructive effect on the placenta.
Debris of placental villi which were seen in the intervillous space are expression of the increased viral attack.
The local spread of HPV from the genital tract may result in placental infection that induces cell death of the trophoblast, placental dysfunction, preeclampsia and spontaneous preterm delivery [22].
There is evidence to show that HPV types 11, 18 and 31 can replicate in trophoblast in vivo [23].
The impaired immunity in HIV positive patients will lead possibly to increased HPV infection contributing with an expansion of lesions in the structure of the placental villi as has been suggested in the uterine cervix [24].
HIV related immunodeficiency alters the relative carcinogenicity of HPV types. A lower fraction of invasive cervical cancer is caused by HPV 16 but the attributable fraction for HPV 18 is concomitantly higher [25].
We have not found these carcinogenetic effects in the placental villi.
Although has been presented that in seven placentas, n=7/12, had a high carcinogenic risk of types 16, 18, 52 and 58 [15].
Infected maternal blood macrophages transmit the infection to placental trophoblasts. Transcytosis, endocityc pathway, is the entry mechanism of these viruses to the placental villi. E5, E6, E7 oncoproteins of HPV are viroporins that generates pores in the syncytium promoting the apoptosis process. This could explain the syncytial interruption observed [26].
This higher aggressiveness of the HPV in patients with HIV due to progressive immunosuppression has been reflected in increased damage to the structure of the villi.
The zidovudine treatment could also to affect the structure of the villi since this has effect on the damage to the mitochondria of the cells [18].
In conclusion, the presence of this viral combination has provoked a higher attack to the structure of the villi which put in danger the normal interchange of gases and nutrients in the maternal-fetal intervillous space.
References
-
Kalter SS (1983) viral expression in the trophoblast. In: Loke YW, Whyte A, (Eds.), Biology of Trophoblast, Elsevier, Ámsterdam, pp: 627-645.
-
Kalk E, Schubert P, Bettinger JA, Cotton MF, Esser M, et al. (2017) Placental pathology in HIV infection at term: a comparison with HIV-uninfected women. Trop Med &Internat Health 22(5): 604-613.
-
Schwartz DA, Sungkarat S, Shaffer N, Laosakkitiboran J, Supapal W, et al. (2000) Placental abnormalities associated with human immunodeficiency virus type 1 infection and perinatal transmission in Bangkok, Thailand. J Infect Dis 182(6): 1652-1657.
-
Bryson YJ (1996) Perinatal HIV-1 transmission: recent advances and therapeutic interventions. AIDS 10(3): S33-S42.
-
Douglas GC, King BF (1992) Maternal-fetal transmission of human immunodeficiency virus: a review of possible routes and cellular mechanisms of infection. Clin Infect Dis 15(4): 678-691.
-
Duryea E, Ramanathan A, Stack S, Rogers V, Roberts S et al. (2012) Placental pathology in HIV infected women. Am J Obstet Gynecol 206(1): S266.
-
D'costa GF, Khadke K, Patil YV (2007) Pathology of placenta in HIV infection. Indian J Pathol Microbiol 50(3): 515-519.
-
Patterson BK, Behbahani H, Kabat WJ, Sullivan Y, O’Gorman MRG, et al. (2001) Leukemia inhibitory factor inhibits HIV-1 replication and is upregulated in placenta from nontransmitting women. J Clin Invest 107(3): 287-294.
-
Spector SA (2001) Mother-to-infant transmission of HIV-1: the placenta fights back. J Clin Invest 107(3): 267-269.
-
Johnson EL, Chakraborty R (2016) HIV-1 at the placenta: immune correlates of protection and infection. Curr Opin Infect Dis 29(3): 248-255.
-
Schwartz DA, Nahmias AJ (1991) Human immunodeficiency virus and the placenta. Current concepts of vertical transmission in relation to other viral agents. Ann Clin Lab Sci 21(4): 264-274.
-
Slatter TL, Hung NG, Clow WM, Royds JA, Devenish CJ, et al. (2015) A clinicopathological study of episomal papillomavirus infection of the human placenta and pregnancy complications. Mod Pathol 28(10): 1369- 1382.
-
Skoczyński M, Goździcka-Józefiak A, Kwaśniewska A (2011) Prevalence of human papillomavirus in spontaneously aborted products of conception. Acta Obstet Gynecol Scand 90(12): 1402-1405.
-
Sarkola ME, Grénman SE, Rintala MA, Syrjänen KJ, Syrjänen SM (2008) Human papillomavirus in the placenta and umbilical cord blood. Acta Obstet Gynecol Scand 87(11): 1181-1188.
-
Rombaldi RL, Serafini EP, Mandelli J, Zimmermann E, Losquiavo KP (2008) Transplacental transmission of Human Papillomavirus. Virol J 5: 106.
-
Chisanga C, Eggert D, Mitchell CD, Wood C, Angeletti PC (2015) Evidence for Placental HPV Infection in Both HIV Positive and Negative Women. J Cancer Ther 6(15): 1276-1289.
-
Bulterys M (2001) Preventing vertical HIV transmission in the year 2000: progress and prospects-a review. Placenta 15: S5-S12.
-
Connor EM, Sperling RS, Gelber R, Kiselev P, Scott, G et al. (1994) Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. Pediatric AIDS Clinical Trials Group. Protocol 076 Study Group. N Engl J Med 331(18): 1173-1180.
-
Benirschke K, Kaufmann P (2000) Pathology of the human placenta. 4th (Edn.), New York: Springer- Verlag.
-
Lewis SH, Perrin E (1999) Pathology of the human placenta, 2nd (Edn.), Churchill Livingstone, New York.
-
Castejón SOC, López GAJ (2013) The placenta infected by HIV and HPV. Rev Electron Biomed/ Electron J Biomed 3: 28-35.
-
Gomez LM, Ma Y, Ho C, McGrath CM, Nelson DB, et al. (2008) Placental infection with human papillomavirus is associated with spontaneous preterm delivery. Hum Reprod 23(3): 709-715.
-
You H, Liu Y, Agrawal N, Prasad CK, Edwards JL, et al. (2008) Multiple human papillomavirus types replicate in 3A trophoblasts. Placenta 29(1): 30-38.
-
Weissenborn SJ, Funke AM, Hellmich M, Mallmann P, Fuchs PG, et al. (2003) Oncogenic human papillomavirus DNA loads in Human Immunodeficiency virus-Positive women with high- grade cervical lesions are strongly elevated. J Clin Microbiol 41(6): 2763-2767.
-
Clifford GM, de Vuyst H, Tenet V, Plummer M, Tully S, et al. (2016) Effect of HIV Infection on Human Papillomavirus Types Causing Invasive Cervical Cancer in Africa. J Acquir Immune Defic Syndr 73(3): 332-339.
-
León-Juárez M, Martínez-Castillo M, González-García LD, Helguera-Repetto AC, Zaga-Clavellina V, et al. (2017) Cellular and molecular mechanisms of viral infection in the human placenta. Pathog Dis 75(7): 1- 15.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer