Lung Cancer Therapeutics Landscape, A Current Overview
Lung cancer is the leading cause of death across the world, both among men and women. According to the CDC, Center for Disease Control and Prevention, every year, about 200,000 people are diagnosed and about 150,000 people die because of lung cancer. Lung cancer begins in the lungs, a pair of respiratory organs in the thoracic cavity. Majority of the lung cancers are carcinogenic in nature, which means the uncontrolled tumor cell growth causes malignant tumor cells, eventually spread out from the lungs to the nearby lymph nodes and possibly to other organs, for example, the brain. Two major types of lung cancers are small cell and non-small cell lung cancers. Non-small cell lung cancer constitutes 80 to 90% of all lung cancers and can further be subdivided into adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. These different types of lung cancers develop differently, grow differently, and are treated differently. Cigarette smoking has been attributed to the number one cause of lung cancer across the world and links to almost 80 to 90% of all lung cancers. Historically, lung cancers have been treated, using conventional therapies which include resection surgery, radiotherapy, and chemotherapies. Recent advancement in science lead to targeted therapies for lung cancer, which includes ALK inhibitors, EGFR inhibitors, VEGF inhibitors, and immunotherapies. This review delves into the recent advancement in the lung cancer therapeutic landscape and discusses recent treatment strategies and options available to the patients. This review also discusses new therapies in the pipeline for lung cancers including allogeneic vaccines. Peptide or protein vaccines, autologous dendritic cell vaccines, DNA vaccines, vector-based vaccines, CAR-T therapies, and Heme-sequestering proteins, which are used to target cancer cells.
Introduction
Background
As the primary source of cancer-related death in the United States -more than colon, breast, and prostate cancers combined [1], lung cancer is one of the most heavily researched diseases in current medicine. Lung cancer is categorized into two subtypes: small-cell lung carcinoma (SCLC) and non-small-cell lung carcinoma (NSCLC), with NSCLC making up approximately 84% of cases. The disease presentation in early stages often mimics other respiratory diseases, preventing early diagnosis and often resulting in poor prognoses and high death rates. With recent improvements in the field of genetic research and drug development, survival rates and life expectancies are on the rise.
Incidence
By 2022, in the United States, there will be an estimated 236,740 new cases and 130,180 deaths, with the disease affecting 1 in 15 men and 1 in 17 women on average [2]. This was estimated to be about 35.1 people out of 100,000 who develop lung cancer in 2018 when the most recent full- scale report was completed [3]. Regarding minority groups, lung cancer is 15% more likely in black men compared to white men, and 14% less likely in black women compared to white women. Globally, an estimated 2.2 million cases of lung cancer were diagnosed in 2020 [4]. Furthermore, the likelihood of developing or dying from lung cancer increases dramatically with age, with a 0.1% chance in individuals under 50 developing the disease and a 5.2% chance in individuals over 70. Variations by global regions and sex directly reflect the prevalence of tobacco smoking.
Risk Factors
The most prevalent risk factor for the development of lung cancer is exposure to tobacco smoke, with approximately 80% of cases being attributed to smoking and acquired genetic mutations from smoking. At least 70 chemical components in tobacco smoke are known carcinogens, and individuals who smoke cigarettes or other tobacco-containing products are 15 to 30 times more likely to get lung cancer [5].
The other 20% of cases result from inherited genetic variations, exposures to secondhand smoke, or other substance exposures. Radon exposure, which enters buildings from cracks or holes that allow the gas in, follows behind tobacco as the second leading cause of lung cancer. Similarly, substances such as asbestos, arsenic, and diesel exhaust can contribute to the development of cancerous cells in the lungs.
Disease Origins
Regarding lung cancer resulting from tobacco smoke, the general mechanism involves carcinogenic material in the smoke that alters DNA function. Once inhaled, the carcinogens are either deactivated and excreted or activated and produce DNA adducts. This altered genetic material can then either be repaired or continue to miscode. Cancer is a result of these mutations and miscoding, occurring in oncogenic or tumor suppressor genes.
![Figure 1: Smoking and its causal relationship with cancer onset [6].](/fulltextimages/8704/fig_1.png)
Since there are many control mechanisms in place to prevent the development of cancer in a healthy individual, those diagnosed with lung cancer may also have defective repair mechanisms or inherited mutations that prevent the normal restoration of healthy cells or genetic material. Specifically, nucleotide excision repair (NER), mismatch repair (MMR), and base excision repair (BER) are common mechanisms for restoring original nucleotide sequences after DNA damage. When these mechanisms are faulty, as is the case in some hereditary diseases [7], DNA adducts cannot be repaired and uncontrolled cell growth results.
Abnormality of the epidermal growth factor receptor (EGFR) gene is the most frequently observed genetic mutation in NSCLC, seen in 10-35% of cases [1], and up to 60% of metastatic NSCLCs [8]. In this case, mutations in exons 19 or 21 result in activation of the tyrosine kinase portion of the gene, which results in excess production of the EGFR protein. Unsurprisingly, this gene has been the target of many drug candidates for lung cancer [9].
Other common sites of mutation include genes such as the RB1 tumor suppressor gene, the p16 tumor suppressor gene, the KRAS oncogene, and the Tp53 tumor suppressor gene. Continued oxidative stress can also lead to the activation of specific transcription factors that may transform normal cells into oncogenic cells.
Diagnosis
Early detection of symptoms suggestive of lung cancer can vastly improve a patient’s prognosis. Once symptoms appear, a chest x-ray is often performed to visualize any masses suspected of being cancer. The next step, if the chest x-ray indicates there is a mass that could be cancerous, is to perform computed tomography (CT) scan for a more accurate picture. Some cancers that may not appear in a chest x-ray can show up on a CT scan [8].
SCLC most commonly originates in the bronchi and often spreads to lymph nodes or smaller lung structures, and this subtype tends to be more responsive to chemotherapy. NSCLC progresses at a slower rate and often is not diagnosed until later and in more severe stages. A diagnostic tool for SCLC involves sputum samples that can be used to identify cancerous cells from upper airway origins. Unfortunately, this tool is not as effective in the diagnosis of the more common NSCLC [8].
Further tests, such as needle biopsies, ultrasounds, PET scans, and MRIs can be done to confirm the presence of cancer or determine if cancer has metastasized. Blood tests such as CBCs and blood chemistries can also be obtained as biomarkers of organ function and allow the ruling out of any other potential diseases [8].
Signs & Symptoms
Although many signs and symptoms of respiratory diseases overlap, some of the most prominent symptoms of lung cancer include a persistent cough, hemoptysis, unexplained weight loss, and chest pain or tightness [3]. Unfortunately, most signs and symptoms distinct to cancer will not appear until later stages when cancer has metastasized. At this point, bone pain, neurological changes, jaundice, or swelling in the lymph nodes may appear. Because of this, early recognition has become a challenge and patient prognoses are often poor.
Prognosis
As one of the deadliest diseases in the field of medicine, the prognosis for lung cancer has historically been poor;
however, recent developments in the drug industry have extended life expectancies and chance for recovery in recent years. Currently, the relative five-year survival rates for localized NSCLC and SCLC are 63% and 27%, respectively. These rates drop to 7% and 3% respectively for stages where cancer has metastasized to distant regions of the body such as the brain, liver, or bones [4]. The risk for metastasizing cancerous activity is relatively high for NSCLC as the disease is not often caught in early stages due to a lack of obvious symptoms, meaning the five-year survival rate for all cases of NSCLC is generally closer to that of metastatic cases. Specifically, the combined five-year survival rate for NSCLC is 25%, while the combined rate for SCLC is 7%.
Prevention
Because the largest risk factor for lung cancer is smoking tobacco, the most effective preventative measure is avoiding tobacco products. Previous studies have concluded that one decade of abstinence from smoking can reduce the risk of lung cancer by up to 50% [10]. Additionally, avoidance of radon, asbestos, and secondhand smoke reduces the risk of developing lung cancer in non-smokers.
Aside from avoidance, the incorporation of antioxidants and vitamin supplements into one’s diet, as well as adequate exercise, has also been linked to reduced risk for lung cancer. Antioxidant-rich foods aid in the prevention of oxidative- based genetic mutations that produce oncogenic cells.
Conventional Treatment Therapies for Lung Cancer
Resection Surgery
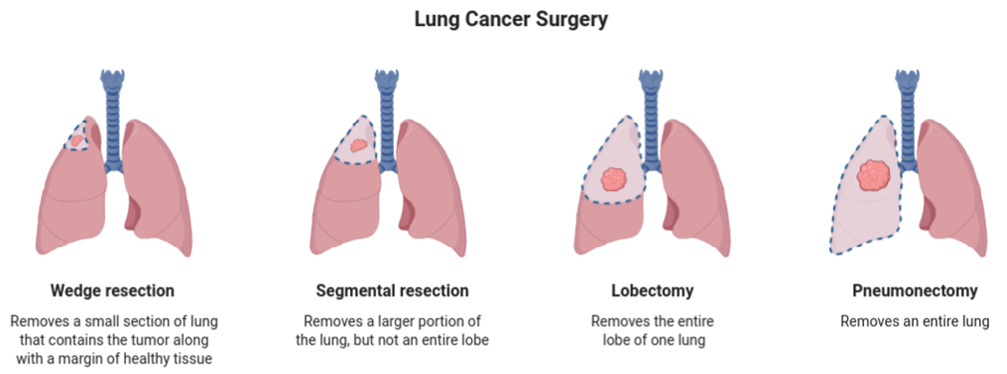
The conventional treatment protocols for lung cancer have been ever so evolving just like the nature of this disease. It is known that most NSCLCs, in earlier stages, are treated with resection surgeries to remove the growing tumor. However, this method alone has proven to be less effective due to its high risk and the need for high precision and skills. Moreover, there were chances of having leftover tumor growths that might not have been dissected completely [11]. Due to this, approaches with radiotherapies and chemotherapies came into existence.
Radiotherapies
Conventional radiation therapies involve external irradiation of high energy radiations onto the tumor growth by locating the tumor via imaging, to decrease the size of the tumor considerably. This chronicled method involved external radiation and was termed External Beam Radiation Therapy (EBRT) [12]. These entailed two-dimensional imaging of the tumor for detection during radiation.
To further enhance this area, conformal radiotherapies that included 3-dimensional imaging were introduced. The 3D (3-Dimensional) imaging would be possible due to Computed Tomography (CT) scans such as in 3D- Conformal Radiotherapy (3D-CRT). 3D-CRT allows for the initial increase in localization to the tumor site with a higher radiation dosage than compared to conventional RT. This allowed for increased tumor diminishment, however, also increased cytotoxicity and decreased specificity of the tumor tissue [13]. Intensified Modulated radiotherapy (IMRT) was further developed which used 3D imaging as well; however, here the radiation was more controlled with radiation dosages in multiple sample fractions, allowing for the radiation to be more concentrated at the region of the tumor site [14]. This also allows for less damage to the neighboring healthy tissues and a decrease in cell toxicity [13].
As 3D-CRT allows for detection of the position of the tumor, a higher technique to account for the motion of the tumor due to respiration is the 4D-CRT. Through this technique, the tumor can be visualized live, and its motion can be accounted for when irradiating. Therefore, the radiation can accurately be targeted the tumor tissue to further reduce unwanted damage and to also enhance the suppression of the tumor [13, 15]. Stereotactic body radiation therapy (SBRT) is another radiation technique that utilizes even higher doses of radiation in even smaller fractions to highly target the tumor site. This method also uses constant imaging and tracking of the location of the tumor. It would be of absolute importance to track the tumor in SBRT since due to its high dosages of radiation, any chances of irradiating on the wrong site would cause dire effects which can even prove to be fatally harmful [15]. It has been seen that SBRT has been used in the early stages of lung cancer in both operable and inoperable patients. However, the level of cytotoxicity increase has been higher than usual. For instance, a phase II study of treating early-stage inoperable lung cancer using SBRT depicted a triple-fold increase in toxicity [12, 16]. Apart from these above-mentioned external radiotherapies, there have been radiotherapies that have been introduced inside the body space to irradiate radiation internally near the tumor site. One such example of lung cancer is Brachytherapy. Here radioactive isotope seeds are placed in the thoracic cavity through surgery usually after the resection of tumor tissues. Depending on the rate at which the radiation is given per time, Brachytherapy can be divided into High dose rate (HDR) and Low dose rate (LDR) [12].
For NSCLC that has metastasized to the brain to form brain tumors, Stereotactic Radiosurgery (SRS) came into existence. In SRS, the metastasized brain tumors from NSCLC can be targeted non-invasively, which uses similar methods of imaging to focus on the tumor and irradiate high doses of radiation in fractions [17]. Though radiotherapy is a pioneer in the reduction and possible cure of lung cancer, it comes with its drawbacks. First, off it can be deduced that due to the radiation, there is a high chance of damage to normal cells as well. Therefore, if these radiations do interact with healthy cells, they can cause several adverse effects, such as DNA breaks and mutations [18].
Chemotherapies
Apart from Radiotherapy, tumor suppression has been made possible with techniques of chemotherapy where certain chemicals having the capability to suppress and shrink tumor growth, are delivered to the target site. Each of these chemotherapeutical drugs targets an essential functionality of the cell and aims to arrest the cell growth and cycle of preferentially the tumor cells. Some drugs such as cisplatin (PLATINOL®, originally patented by Bristol- Myers Squibb) and carboplatin (PARAPLATIN®, originally patented by Bristol-Myers Squibb) induce cessation of transcription and replication of DNA so that the cell cannot further continue in its cell cycle. This would eventually lead to cell death. The mechanism to achieve these results involves interfering with the nitrogenous base pairs of DNAs via binding and thus altering its function [19]. Drugs that can still affect the transcription of DNA without itself binding to the DNA molecules have also been synthesized. These drugs instead target crucial enzymes involved in the process of transcription and hinder their function. One such example would be Lurbinectedin (ZEPZELCA®, originally patented by Jazz Pharmaceuticals). This drug inhibits the over-transcription performed by the tumor cells through its binding on RNA polymerase II. Since RNA Polymerase II is needed for transcription to successfully occur, Lurbinectedin inhibits its function and causes a halt to cell growth [20].
Other classes of drugs such as Paclitaxel (TAXOL®, by Bristol-Myers Squibb) and Docetaxel (TAXOTERE®, by Sanofi Aventis) are some of the other common drugs used in chemo- regiments. These drugs target the microtubular dynamics of the cell, causing the cell’s tubulin network to disintegrate and therefore cause the cell to arrest. This is achieved by these drugs via their ability to bind to B-tubulin subunit with high affinity. One of the vital classes of drugs used against lung cancer is antifolates. Pemetrexed (ALIMTA®, originally patented by Eli Lilly) is one such antifolate commonly used, that targets the folate-dependent biosynthetic pathways. Adenine, guanine, and thymine synthesis are carried out through these folate pathways, folate being a vital co-factor in these processes. Inhibiting these folates would alter the synthesis of these nucleotides, which in turn, hinders DNA synthesis, therefore, affecting cell growth. This can be achieved by antifolates that can inhibit the actions of folate or the production of folate. Pemetrexed specifically inhibits multiple enzymes involved in these pathways, such as dihydrofolate reductase (DHFR) and thymidylate synthase (TS) [21].
Chemotherapy regimens usually have multi-drug deliveries to counter the cancer growth from multiple perspectives. Common regiments such as Paclitaxel and Carboplatin or Cisplatin as used in the treatment of NSCL [22, 23]. Furthermore, many areas of the target can be found in which different chemotherapeutic drugs have been developed to reach the results of halting the tumor cell cycle and growth.
However, it can be already deduced that since these drugs target essential functions of the cell cycle and growth, they have major debilitating side effects. For instance, Paclitaxel and Pemetrexed are known to cause myelosuppression and cell cytotoxicity [24]. Pemetrexed can also lead to hematological toxicity in the absence of any folate and vitamin supplements [25]. Moreover, chemotherapies instigate the excess release of reactive oxygen species (ROS), which are harmful to the normal functioning of the cells as they are mutagenic which further induces the development of cancers [26]. Apart from cellular effects, chemotherapies have noticeable physical effects such as drastic hair loss, malaise, nausea, and much more [27]. In addition to that, evidence of resistance to these drugs has been found in lung cancers, where the tumors have adapted means to bypass the effects of these drugs and instead cause side effects. Such as, Paclitaxel resistance developed in NSCLC in recent years, has allowed the tumor cells to overcome the effects of B-tubulin binding by Paclitaxel, due to tubulin structure disruptions [28].
Due to these reasons and side effects, the conventional approaches and therapies toward lung cancers are being challenged and new therapies and protocols are arriving as we speak. These are necessary as we continue to fight for an absolute cure or a better option with minimal side effects and high benefits towards resolving the illness of lung cancer.
Targeted Therapies
Introduction
Although conventional therapies like chemotherapy, radiation, and surgery are often the options that come to mind when cancer treatment is first brought up, targeted therapies represent a major resource for tumor suppression in hard-to-treat cancers. The two major types are small- molecule drugs and monoclonal antibodies [29]. Small- molecule drugs can enter cells due to their small size and act on internal targets, while monoclonal antibodies are lab-produced and bind externally, producing a variety of responses including marking cells for the immune system, growth arresting cancer cells directly, or releasing toxins that lyse the cells. Other types of targeted therapies exist, such as tyrosine kinase inhibitors, which are small molecules that act on the surface of cancer cells.
ALK Inhibitors
According to the National Cancer Institute, run by the National Institutes of Health (NIH), the premier medical research center of the United States government, anaplastic lymphoma kinase (ALK) is a normal cell surface protein, often involved in the development of the brain and neurons during embryogenesis [30]. An ALK-positive cancer, however, often has a modified form of the ALK gene or an excess of ALK protein that contributes to the uncontrolled growth of these cancer cells. Not all cancers are ALK-positive, but one notable, conventionally hard-to-treat type is non-small cell lung cancer (NSCLC). An ALK inhibitor is a type of targeted cancer therapy, known as a tyrosine kinase inhibitor, whose role is to block ALK function, which may halt the growth and spread of the cancer cells.
Xalkori™ (Crizotinib, PF-02341066) was the initial first- generation ALK inhibitor that was created and received fast-tracked approval by the Food and Drug Administration (FDA) for the treatment of ALK-positive NSCLC [31]. For ALK NSCLC, the objective response rate (ORR) has been shown, to be near 60% and there is a median progression-free survival (PFS) estimate of 8 to 10 months [31, 32, 33]. Unfortunately, there has been an emergence of resistance to Crizotinib, as of late. Therefore, new ALK inhibitors that target other kinases and have demonstrated greater potency have been developed.
The second-generation ALK inhibitors, that have emerged to deal with the expansion of resistance include Alectinib (marketed as Alecensa™), which has activity against L1196M, a common secondary mutation that is one of the leading causes of Crizotinib resistance [34, 35]. Studies have shown its effectiveness even in metastatic forms of ALK NSCLC [36]. Other notable ALK NSCLC drugs from the same generation include Ceritinib and Brigatinib (marketed as Alunbrig™), a potent inhibitor, and an Epidermal Growth Factor Receptor (EGFR) as well.
Despite the promising effects of these second- generation variants, the further occurrence of resistance in these ALK cancer tumors prompted the creation of a third-generation ALK inhibitor known as Lorlatinib (PF- 06463922, Lorbrena®). So far, this drug has proven to be effective against all currently known resistant mutants [37, 38, 39]. It achieves this by working in combination with PI3K pathway inhibitors [40].
EGFR Inhibitors
EGFR, also known as HER1 (human epidermal growth factor receptor 1) or ErbB1, belongs to the family of tyrosine kinase receptors, and in cancer cells causes cell proliferation, angiogenesis, resistance to apoptosis, cell invasion, and ultimately, metastasis of note [41, 42], vascularization through angiogenesis is essential for tumor growth and maintenance due to the higher metabolic needs and waste production of these tumors [43].
EGFR inhibitors can be categorized into two types: tyrosine kinase inhibitors (TKIs) and monoclonal antibodies (mAbs). EGFR TKIs function by preventing autophosphorylation of the adenosine triphosphate (ATP) pocket and therefore disrupting downstream signaling, while EGFR mAbs are antagonists for extracellular EGFR receptors, causing a dampening of their functions [41].
Tarceva® (Erlotinib) is a small-molecule, tyrosine kinase inhibitor that has been developed to block EGFR signaling pathways in NSCLC patients [44]. It was the first EGFR inhibitor that showed a survival benefit in patients with lung cancer during clinical trials and was subsequently approved by the FDA in 2004. In a European randomized trial that compared the effectiveness of Tarceva to the more standard platinum-based chemotherapy approach in patients with advanced NSCLC, Tarceva was superior in the metric of progression-free survival. Like other EGFR inhibitors, a rash is a common symptom of Tarceva use and has been proposed as a potential biomarker of drug activity. In addition, diarrhea was also seen with greater frequency in the Tarceva experimental group than in the placebo group.
VEGF Inhibitors
Vascular endothelial growth factor (VEGF), sometimes called vascular permeability factor (VPF), is a known angiogenic factor and is often up-regulated in tumors [45]. It is similar in function to EGFR, and they work in cohesion;
VEGF signaling is up-regulated when EGFR is expressed, and VEGF up-regulation causes resistance to EGFR inhibition [46]. Therefore, VEGF inhibitors are often used at the same time as EGFR inhibitors as a targeted approach. Often, the addition of a VEGF inhibitor can help overcome the resistance that has been developed by the tumor against EGFR inhibitors.
Avastin® (Bevacizumab, by Genentech), which falls in the mAb category of targeted therapies, is used against many cancer types including NSCLC. It was the first angiogenesis inhibitor to be approved and it was the first drug that helped NSCLC patients live longer than one year in combination with chemotherapy [43]. The pivotal study E4599 demonstrated a reduction in risk of death by 21% when used in combination with the chemotherapies Carboplatin and Paclitaxel, as compared to when the chemotherapies were utilized alone. Avastin works by binding to all isoforms of VEGF-A and thereby inhibiting VEGF signaling pathways by blocking the ligand VEGFR. Although novel angiogenesis inhibitors continue to be created, Avastin is still highly utilized and will likely retain its importance in the foreseeable future within the drug treatment landscape.
KRAS Inhibitors
The KRAS gene contains the instructions for encoding a protein called K-Ras, which is part of the RAS/MAPK signaling pathway [47]. This pathway is responsible for relaying the message to the nucleus that the cell is ready to proliferate or differentiate. The protein itself, K- Ras, is a GTPase, which means it is responsible for the conversion of GTP into GDP as soon as GTP binds. Bound GTP causes the protein to be activated and the signal to be transmitted, while conversion to GDP causes the protein to be turned off and for signal relay to stop.
The KRAS gene belongs to the RAS family of oncogenes and can become cancerous upon mutation. 32% of all NSCLCs have mutated forms of the KRAS gene that can be targeted by KRAS inhibitors [48]. Originally K- Ras was considered an undruggable protein, despite it having a large role in cancer development. This was largely due to the fact, that it lacks an obvious pocket in which an allosteric inhibitor can bind.
However, in 2013 the narrative changed when Kevan Shokat from the University of California, San Francisco, discovered Lumakras. Lumakras® (Sotorasib, by Amgen) was the first KRAS inhibitor to be approved by the FDA after less than three full years of clinical testing. It was licensed for the specific use in the case of a G12C substitution and the stipulation that the patient has already failed to respond to at least one other therapeutic. The inhibitor works by creating an irreversible covalent bond that targets the sulfur group in the introduced cysteine. The approval of Lumakras has stimulated further research and development into other KRAS inhibitors for different mutants of the gene and will hopefully lead to novel therapeutics for patients diagnosed with NSCLC.
Immunotherapy: Checkpoint blockade
Overview
Current treatment protocols call for the 1st line treatment of lung cancers with immune checkpoint inhibitors (ICIs), with or without chemotherapy [49]. ICIs represents a systemic approach to restoring immune-mediated anti-tumor activity. Pembrolizumab (Keytruda®; by Merck) is a PD-L1 blocking agent that has emerged as the immunotherapy of choice for NSCLC and other cancers, becoming the highest-selling cancer drug worldwide [50].
The development of ICIs represents collaboration between industry and scientists doing basic research. Dr. James P. Allison, Ph.D., of Texas, and Dr. Tasuku Honjo, MD, Ph.D., of Kyoto, Japan received the 2018 Nobel Prize in Physiology or Medicine for their pioneering work in discovering proteins that serve as breaks in the immune system [51]. Biologics targeting and releasing these breaks in the immune system became the first immune checkpoint inhibitors (ICIs).
ICI’s application was the first time when immunotherapy had been successfully used to treat cancer. At that time, research was mostly dedicated to developing molecularly targeted drugs against cancer. However, the use of targeted therapies almost always leads to cancer drug resistance. ICIs can lead to long-lasting recoveries and a virtual cure for some patients. ICIs work on a systemic level to “turn up” the immune response so that T cells can recognize and destroy cancer cells [52].
The immune system is tightly controlled to be able to both respond to pathogens, yet also not attack the body’s own tissues and cause autoimmune disease. CTLA-4 and PD-1 are two immune-cell surface receptors that serve as brakes on the immune system. Cancer takes advantage of these proteins to dampen further dampens the immune response and prevent the immune system from attacking cancer. Drugs developed to inhibit CTLA-4 and PD-1 represent the newest class of immunotherapies, ICIs [52].
Safety Profile
ICIs have a favorable safety profile as compared to most chemotherapy. However, as ICIs release the brakes on the immune cells, complications related to the immune system are possible. Most patients report some side effects, with the most common side effect including tiredness, diarrhea, pain in muscles and joints, and shortness of breath [52, 54]. Special care should be given when administering ICIs to patients with pre-existing autoimmune disorders.
Approval and Endpoints
Due to their unique mechanism of action, immunotherapies cannot be evaluated with the same endpoints as chemotherapies. As compared to chemotherapies, immunotherapies show significant effects after several weeks and improve overall survival rates in patients. Furthermore, some patients who respond well to ICIs experience sustained remission for more than 10 years, leading to a virtual “cure” [55]. These issues were important regulatory considerations during the clinical trial evaluation of the first FDA-approved ICI, ipilimumab. Ipilimumab was first evaluated for use in advanced melanoma but did not yield significant results when compared to chemotherapies using traditional endpoints. A pivotal study was needed in which Bristol Myers Squibb committed to measuring overall 5-year survival to show the dramatic effects of ICIs in patients who do respond Fellner C, et al. [52].
FDA Approved Immunotherapies
Ipilimumab (Yervoy®) developed by Bristol Myers Squibb and first validated by Dr. James Allison in his research lab at Berkeley is a CTLA-4 inhibitor. Ipilimumab was first developed to treat melanoma but is now indicated for many types of cancer. Pembrolizumab (Keytruda®; Merck) and nivolumab (Opdivo®; Bristol Myers Squibb) are PD-1 inhibitors also approved for many cancer subtypes. Keytruda is the highest-selling cancer drug worldwide, generating $14.38 billion USD in 2020 [50].
ICIs can be used alone or in combination with other cancer therapies such as chemotherapies, targeted therapies, radiation therapies, and surgery. Keytruda can be used alone when a tumor cannot be respected by surgery and expresses high levels of PD-L1 [54]. PD-L1 is a biomarker used to determine the responsiveness of a patient to Keytruda and tumors that express little to no PD-L1 are difficult to treat using immunotherapies.
Factors Influencing Response Rates
For patients, immunotherapies often represent a favorable treatment modality. Immunotherapies generally lead to fewer side effects as compared to chemotherapy and targeted therapies, and treatments are less frequent (every 3 weeks for Keytruda). However, response rates to immunotherapies can vary [56]. Certain types of cancer, such as melanoma can have a high response rate, up to nearly 60%. However, for lung cancers, the response rate is much lower, between 20-30%. Many factors influence this response rate, including the tumor mutational burden. Tumors with higher mutational burdens (defined as greater than or equal to 10 mutations per Mb DNA) have a higher response rate than those with a lower mutational burden. As such, the FDA has approved the use of PD-1 inhibitors for any solid tumor with a mutational burden greater than or equal to 10 mutations per Mb [56].
Another factor influencing response to immunotherapies is the gut micro biome and consumption of dietary fiber [57]. Patients on a high dietary fiber diet had increased response rates to ICIs. Furthermore, patients taking supplemental probiotics showed a lower response rate to ICIs. These results implicate the gut micro biome as a likely modulator of immune function and checkpoint inhibition of immune cells.
The tumor microenvironment is also a key player in modulating the immune response, and consequently response rates to ICIs. T cells must be able to differentiate and infiltrate the tumor microenvironment, in order to elicit a response. The tumor microenvironment prevents this by using complex stimulatory and inhibitory signaling pathways [58].
Keytruda SCLC Withdrawal
On March 1, 2022, Merck & Co., Inc. voluntarily withdrew the indication for pembrolizumab (Keytruda®) in small cell lung cancer (SCLC) [59]. This decision followed a lack of clinical data in showing significant increases in progression- free or overall survival when Keytruda is used for SCLC in conjunction with platinum-based chemotherapy or after the use of platinum-based chemotherapy and another line of treatment.
Merck had initially been given accelerated approval for Keytruda by the FDA, under the condition that this approval would only continue given, that favorable data from post- market surveillance is obtained. Failure to meet these requirements and based on the FDA’s advice, Merck decided to withdraw this indication.
Keytruda Patent Litigation
Merck’s best-selling cancer drug, Keytruda, faced patent- infringement litigation. In January 2017, Merck settled with Bristol-Myers Squibb and Ono Pharmaceutical. Merck paid $625 million in cash to these two companies and agreed to pay a 6.5% royalty on Keytruda sales until December 2023 [60, 61]. The patent-infringement case was mired in legal complexities stemming from overlapping patent families. After this resolution, another lawsuit followed, this time in Japan and with Dr. Tasuku Honjo as the plaintiff. Dr. Honjo received the ½ share of the 2018 Nobel Prize in Physiology or Medicine for his discovery of the PD-1 receptor. Dr. Honjo claimed that we were not being fairly compensated for his discovery and his role in Ono Pharmaceutical’s successful litigation against Merck. The dispute was eventually settled with Ono Pharmaceutical agreeing to pay Dr. Honjo 5 billion yen and donating 23 billion yen to Kyoto University, where Dr. Honjo made his breakthrough discovery [62, 63].
The Pipeline
New Therapies in Development
In addition to the anticancer therapies mentioned above, there are a number of new therapies in various stages of preclinical and clinical development with hopes of reaching patient populations. These therapies, such as cancer vaccines, CAR-T therapy, and HeSPs, aim to target cancer without the limitations of existing treatment modalities and help to overcome drug resistance and therapeutic failure. They are described as follows:
Cancer Vaccines
Cancer vaccines are a novel form of immunotherapy where the immune system is selectively sensitized to an antigenic target. The goal of the cancer vaccine is to invoke an immune response to target the tumor tissue. Cancer vaccines have been developed against NSCLC but have been largely shown to be ineffective in phase II trials even though they have displayed a positive safety profile. There are four main vaccine targets: gangliosides, tumor-associated antigens (TAAs), cancer-testis antigens (CTAs), and normal cell antigens with higher expression in cancer [64]. These targets can be targeted in five cancer vaccine types, discussed below: Allogeneic Vaccines: Allogeneic vaccines derive their antigens from cancer cells of another patient. Antigens are taken from a patient with a similar tumor type as another patient and injected into the other patient to elicit an immune response. One such vaccine, Belagenpumatucel-L, was made by a transfecting NSCLC cell line with the plasmid containing TGF-β2 antisense transgene [65]. Although phase II clinical trials were promising, phase III clinical trials failed to reach OS endpoints and were largely discontinued. Peptide/Protein Vaccines: Peptide or protein vaccines are derived from recombinant antigens intended to facilitate an immunogenic response. One such example is CimaVax-EGF, which was developed in Cuba against NSCLC and is currently undergoing testing in the United States, among other countries [66]. CimaVax works by causing an immune response against epidermal growth factor (EGF). EGF overexpression is seen in cancer, and overexpression is seen in angiogenesis and metastatic factors such as migration and invasion properties of tumors. Targeting of EGFR (epidermal growth factor receptor) with small molecules such as gefitinib (Iressa®, by AstraZeneca), erlotinib (Tarceva®, by Genentech), afatinib (Gilotrif®, by Boehringer Ingelheim), Osimertinib (Tagisso®, by AstraZeneca), and monoclonal anti-EGFR antibody Cetuximab (Erbitux®, by ImClone LLC) has seen varying degrees of success. CimaVax-EGF raises antibodies against EGF with lowers blood levels of EGF and prevents simulation of EGFR by EGF (EGF is EGFR’s main ligand). Thus, CimaVax- EGF has the potential to be a successful preventative vaccine, with positive results seen in clinical trials in Cuba. Autologous Dendritic Cell Vaccines: These are an emerging treatment modality in which the vaccines are made from the patient’s own cells. Patient blood samples are taken from which immune cells are isolated. These cells are then cultured and then exposed to tumor antigens, thus creating antigen-presenting dendritic cells, which can be reinjected into the patient to facilitate an immune response against cancer. One such example is MIDRIXNEO-LUNG, which are currently in phase I clinical trials [67]. DNA Vaccines: DNA vaccines work by directly introducing a plasmid with a DNA sequence in order to have antigen production within the cell. An example of this is MAGEA3 (Melanoma antigen-A3, which is a cancer-testis antigen), is currently in Phase 1/2 clinical trials for NSCLC [68]. KRAS DNA vaccines have also been explored in mice, although the current biotech atmosphere seems to be more in the direction of small molecule KRAS inhibitors, such as Sotorasib (Lumakras®, by Amgen) and Adagrasib (by Mirati Therapeutics, Inc.) [69]. Vector-Based Vaccines: Vector-based vaccines make use of mainly viruses or bacteria to introduce antigens into the body in order to facilitate an immune response. An example is TG4010, which uses a viral vector that encodes MUC1 and IL2. This drug is currently in phase II and III clinical trials for NSCLC in combination therapy with the immunotherapy Nivolumab (Opdivo®, by Bristol Myers Squibb) [70].
CAR-T
Chimeric antigen receptor T-cell, or CAR-T, therapy is a novel therapy that uses T-cells removed from the patient’s blood that are genetically edited to incorporate specific antigen receptors on the surface. These CAR-T cells are then reinfused back into the patient’s blood to hopefully elicit an immune response against cancer cells displaying that same antigen [71].
While CAR-T therapy has displayed many recent successes in non-solid tumors, solid tumors display challenges making them resistant to CAR-T. Solid tumors display high antigen heterogeneity, which eludes CAR-T cell efficacy due to antigen specificity. Decreasing receptor antigen specificity could alleviate this issue but increased the risk for off-target interactions [72]. Additionally, both the surrounding collagen dense surrounding of the tumor and the tumor microenvironment pose challenges. Thus, it is unlikely to see success for CAR-T therapy in clinical solid lung tumors in the near future.
However, some success has been seen in mouse models [73]. Li and colleagues engineered T-cells to display EGFR antigen, which displayed anti-tumor efficacy in EGFR positive NSCLC xenografts in mice.
Benefits Compared to Traditional Therapies
Due to their unique mechanism of action that selectively starves cancer by targeting tumor bioenergetics, HeSPs represents a truly novel approach to cancer therapy. Unlike chemotherapies, which are toxic to all cells and cause many undesirable symptoms such as hair loss, infection, anemia, neuropathy, and chemo brain, HeSPs are unlikely to display such symptoms as healthy cells are not affected. Targeted therapies depend on the presence of targetable mutations, and in many lung cancer patients, these targets do not exist. Even in patients whose cancer displays these mutations, targeted therapy usually only works for a relatively short period of time. However, HeSPs due not depend on targetable mutations as they target the sum of many genetic alternations, thereby allowing them to be used regardless of cancer type. Immunotherapy is an emerging treatment modality with great success seen in a number of cancer models, however only 15-20% of patients usually respond, and it depends on certain immune markers and checkpoints that not all cancers display. CAR T-cell therapies, as discussed above, are largely unsuccessful in the treatment of solid tumors like lung cancer [74].
Moreover, all these mentioned treatment modalities have been shown to lead to treatment resistance and eventual therapeutic failure. However, preclinical studies have shown that HeSPs may be able to prevent and overcome drug resistance by targeting OXPHOS and improving the tumor microenvironment [75]. Therefore, HeSPs have the potential to be combined with existing treatment modalities to improve outcomes.
Commercialization Efforts
The global lung cancer therapeutic market is immense, projected at $44.7 Billion by 2027 with a CAGR of 14.2 [76]. North America currently holds the largest share of this market, although this is projected to change. An aging population with a history of smoking is a major contributor to the lung cancer burden in North America.
However, this market share is likely to change as Asia Pacific is projected to grow with the fastest CAGR. More recent smoking habits and accumulation of wealth in developing countries will lead to both a demand for and the ability to buy lung cancer therapeutics. India and China are projected to make up the majority of this demand [77].
Major Companies
Major biotechnology companies dominating the lung cancer market include Merck, Bristol Myers Squibb, and Roche [76]. The dominance of Merck and Bristol Myers Squibb can be attributed in large part to their early development of key immunotherapy medications, namely Immune Checkpoint Inhibitors (ICIs). Merck currently produced the most successful and best-selling cancer drug in the world, Keytruda®, a PD-1 targeting antibody. Bristol Myers Squibb was the company to work on Immune Checkpoint Inhibitors and received the first FDA approval for use in melanoma in 2011 [77].
Roche’s dominance depends on Avastin®, (generic: bevacizumab), an anti-VEGF (vascular endothelial growth factor) antibody that interferes with tumor angiogenesis, a tumor’s ability to create new blood vessels to supply it with needed nutrients. Avastin effectively disrupts the tumor microenvironment and has been effective for a number of cancers, including lung cancers. The FDA approved Avastin for use in NSCLC patient who no longer responds to chemotherapies or targeted therapies in 2006 [78].
However, the patents for Avastin will expire in 2019 in the US and 2022 in Europe [79]. This means that competing drug companies are rapidly developing biosimilars that will likely diminish Avastin’s market dominance. Zirabev® (bevacizumab-bvzr) made by Pfizer received FDA approval in 2019 as a biosimilar VEGF-inhibitor, with Avastin as the reference drug. Zirabev® is currently indicated for many types of non-small cell lung cancers [80].
Major Research Institutions
MD Anderson: The University of Texas MD Anderson Cancer Center is one of the largest and most influential cancer research centers in the US and worldwide. MD Anderson is located in Houston, Texas and its mission statement is to “eliminate cancer in Texas, the nation, and worldwide” [81]. It is attempting to do this by integrating research with patient care, emphasizing both training of future physicians and scientists, and taking measures to prevent cancer on a societal level. Huntsman Cancer Institute: The Huntsman Cancer Institute is another major research institution in both cancer research and cancer treatment. It is located in Salt Lake City, Utah, and is an NCI-designated cancer research facility. Huntsman Cancer Institut e is dedicated to both basic and translational research, connecting doctors, patients, and researchers [82]. Dana-Farber Cancer Institute: The Dana-Farber Cancer Institute, located in Boston, Massachusetts is similarly involved in both research breakthroughs and patient care. Dana-Farber collaborates heavily with Harvard Medical School and the Harvard Comprehensive Cancer Center. Dana- Farber is currently hosting a number of influential clinical trials for Non-small cell lung cancers [83].
Major Players
Dr. James P. Allison, PhD: The Department of Immunology at MD Anderson has been extremely influential and is headed by Dr. James Allison, the Nobel-winning scientist who first discovered immune checkpoint blockage immunotherapies. Dr. Allison is the Chair of the Department of Immunology, Distinguished Chair for Cancer Research and Director of the Parker Institute for Cancer Research. His work has not only been influential in the early discovery of immunotherapies but rather also in their subsequent clinical development and current efforts to dramatically increase patient response rates to immunotherapy drugs [81]. Mr. Robert M. Davis: Robert M. Davis is the Chief Executive Officer and President of Merck. As the head of a large pharmaceutical company that holds a significant share of the global lung cancer market, he is a major player in this field. He is the ultimate person responsible for Merck’s developmental programs and which drug candidates it wants to pursue. He is also responsible for Merck’s acquisition of innovation through acquiring smaller biotech companies [84]. Dr. Karen E. Knudsen, MDA, PhD: Dr. Karen E. Knudsen is also a major field in cancer, including lung cancer, as the CEO of the American Cancer Society. The American Cancer Society is among the most important and influential organizations supporting, encouraging, and lobbying for cancer research. She is also on the board of advisors for the National Cancer Institute as well as the external advisory board of 12 NCI- designated cancer centers [85].
Conclusion
Lung cancer remains a formidable disease that significantly impacts many people. Despite the approval of innovative treatments, the 5-year survival rate remains dismally low at under 25%. Clearly, new innovations and discoveries in cancer treatment are needed to significantly improve outcomes for patients.
In the 1980s, targeted therapies were heralded as the “magic bullet” of cancer therapy due to their targeted mechanisms of action. However, the use of targeted therapies almost always leads to resistance to these drugs and eventual therapeutic failure. Cancer is able to adapt and overcome targeted therapies due to the selection pressures that targeted specific mutations and proteins pose.
Much of the current landscape of cancer research is dedicated to the discovery of new cancer targets and the development of targeted therapies based on these. While the approval of each new targeted therapy represents millions of dollars and years of research, these drugs are only likely to add months to the life of lung cancer patients. Long-term remission remains elusive with the use of traditional targeted therapies and chemotherapies.
Immunotherapies dramatically changed the landscape of cancer therapy by harnessing the body’s own immune cells to fight cancer. This approach led to long-term remission for some patients, with many fewer side effects than targeted therapies or chemotherapies. Furthermore, immunotherapies have now been approved for many subtypes of cancer. A lot of research is being done to expand the indication of immunotherapies and develop new strategies to target the immune system.
However, even this approach faces obstacles. CAR-T cell therapy, an immunotherapy, that uses a patient’s own genetically engineered T cells, faces insurmountable obstacles in its use against solid tumors. Recently, Keytruda, the world’s best-selling cancer drug and immunotherapy, lost its indication for small cell lung cancer.
Thus, we believe that innovative new cancer treatments stemming from basic research are needed to advance the lung cancer therapeutic landscape. It is likely that the future ‘cures’ for cancer are yet unknown, and that much basic scientific research is needed to discover the cancer cures of the future.
References
-
Schabath MB, Cote ML (2019) Cancer Progress and Priorities: Lung Cancer. Cancer Epidemiol Biomarkers Prev 28(10): 1563-1579.
-
(2019b) What Causes Lung Cancer?. American Cancer Society.
-
(2019a) Signs and Symptoms of Lung Cancer. American Cancer Society.
-
(2021a) Lung Cancer Survival Rates. American Cancer Society.
-
(2021) What are the Risk Factors for Lung Cancer?. Centers for Disease Control and Prevention.
-
(2010) How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Centers for Disease Control and Prevention (US).
-
Knoch J, Kamenisch Y, Kubisch C, Berneburg M (2012) Rare hereditary diseases with defects in DNA-repair. Eur J Dermatol 22(4): 443-455.
-
(2021b) Tests for Lung Cancer. American Cancer Society.
-
Zhang YL, Yuan JQ, Wang KF, Fu XH, Han XR, et al. (2016) The prevalence of EGFR mutation in patients with non- small cell lung cancer: a systematic review and meta- analysis. Oncotarget 7(48): 78985-78993.
-
Dela Cruz, CS, Tanoue LT, Matthay RA (2011) Lung Cancer: Epidemiology, Etiology, and Prevention. Clinics Chest Med 32(4): 605-644.
-
Scagliotti G, Novello S (2003) Adjuvant chemotherapy after complete resection for early stage NSCLC. Lung Cancer 42(S1): S47-S51.
-
Parashar B, Arora S, Wernicke AG (2013) Radiation therapy for early stage lung cancer. Semin Intervent Radiol 30(2): 185-190.
-
Brown S, Banfill K, Aznar MC, Whitehurst P, Faivre Finn C (2019) The Evolving Role of Radiotherapy in Non-Small Cell Lung Cancer. Br J Radiol 92(1104): 20190524.
-
Bakiu E, Telhaj E, Kozma E, Ruçi F, Malkaj P (2013) Comparison of 3D CRT and IMRT Tratment Plans. Acta inform Med 21(3): 211-212.
-
Saadeddin A (2012) Radiotherapy for NSCLC: Review of conventional and new treatment techniques. Journal of Infection and Public Health 5(S1): S45-S49.
-
Timmerman R, McGarry R, Yiannoutsos C, Papiez L, Tudor K, et al. (2006) Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inoperable early-stage lung cancer. J Clin Oncol 24(30): 4833-4839.
-
Soliman H, Das S, Larson DA, Sahgal A (2016) Stereotactic radiosurgery (SRS) in the modern management of patients with brain metastases. Oncotarget 7(11): 12318-12330.
-
Löbrich M, Kiefer J (2006. Assessing the likelihood of severe side effects in radiotherapy. International Journal of Cancer 118(11): 2652-2656.
-
Rossi A, Di Maio M (2016) Platinum-based chemotherapy in advanced non-small-cell lung cancer: optimal number of treatment cycles. Expert Rev Anticancer Ther 16(6): 653-660.
-
Yang S, Zhang Z, Wang Q (2019) Emerging therapies for small cell lung cancer. Journal of Hematology & Oncology 12(1): 47-47.
-
Rollins KD, Lindley C (2005) Pemetrexed: A multitargeted antifolate. Clin Ther 27(9): 1343-1382.
-
Belani CP (1998) Paclitaxel/Carboplatin in the Treatment of Non-Small-Cell Lung Cancer. Oncology (Williston Park) 12(1 S2): 74-79.
-
Schiller JH, Harrington D, Belani CP, Langer C, Sandler A, et al. (2002) Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med 346(2): 92-98.
-
Ramalingam S, Belani CP (2002) Taxanes for advanced non-small cell lung cancer. Expert Opin Pharmacother 3(12): 1693-1709.
-
Hanna N, Shepherd FA, Fossella FV, Pereira JR, De Marinis F, et al. (2004) Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J Clin Oncol 22(9): 1589-1597.
-
Conklin KA (2004) Chemotherapy-Associated Oxidative Stress: Impact on Chemotherapeutic Effectiveness. Integrative Cancer Therapies 3(4): 294-300.
-
Aslam MS, Naveed S, Ahmed A, Abbas Z, Gull I, et al. (2014) Side Effects of Chemotherapy in Cancer Patients and Evaluation of Patients Opinion about Starvation Based Differential Chemotherapy. Journal of Cancer Therapy 5(8): 817-822.
-
Cui H, Arnst K, Miller DD, Li W (2020) Recent Advances in Elucidating Paclitaxel Resistance Mechanisms in Non- small Cell Lung Cancer and Strategies to Overcome Drug Resistance. Curr Med Chem 27(39): 6573-6595.
-
(2020) Targeted Therapy to Treat Cancer. National Cancer Institute.
-
Wu J, Savooji J, Liu D (2016) Second and third-generation ALK inhibitors for non-small cell lung cancer. J Hemat Oncol 9(1): 19.
-
Kwak EL, Bang YJ, Camidge DR, Shaw AT, Solomon B, et al. (2010) Anaplastic Lymphoma Kinase Inhibition in Non-Small-Cell Lung Cancer. N Engl J Med 363(18): 1693-1703.
-
Awad MM, Shaw AT (2014) ALK Inhibitors in Non- Small Cell Lung Cancer: Crizotinib and Beyond. Clin Adv Hematol Oncol 12(7): 429-439.
-
Shaw AT, Kim DW, Nakagawa K, Seto T, Crinó L, et al. (2013) Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med 368(25): 2385- 2394.
-
Kinoshita K, Asoh K, Furuichi N, Ito T, Kawada H, et al. (2012) Design and synthesis of a highly selective, orally active and potent anaplastic lymphoma kinase inhibitor (CH5424802). Bio org Med Chem 20(3): 1271-1280.
-
Sakamoto H, Tsukaguchi T, Hiroshima S, Kodama T, Kobayashi T, et al. (2011) CH5424802, a selective ALK inhibitor capable of blocking the resistant gatekeeper mutant. Cancer Cell 19(5): 679-690.
-
Gadgeel SM, Gandhi L, Riely GJ, Chiappori AA, West HL, et al. (2014) Safety and activity of alectinib against systemic disease and brain metastases in patients with crizotinib-resistant ALK-rearranged non-small-cell lung cancer (AF-002JG): results from the dose-finding portion of a phase 1/2 study. Lancet Oncol 15(10): 1119-1128.
-
Infarinato NR, Park JH, Krytska K, Ryles HT, Sano R, et al. (2016) The ALK/ROS1 Inhibitor PF-06463922 Overcomes Primary Resistance to Crizotinib in ALK- Driven Neuroblastoma. Cancer Discov 6(1): 96-107.
-
Tucker ER, Danielson LS, Innocenti P, Chesler L (2015) Tackling Crizotinib Resistance: The Pathway from Drug Discovery to the Pediatric Clinic. Cancer Res 75(14): 2770-2774.
-
Zou HY, Friboulet L, Kodack DP, Engstrom LD, Li Q, et al. (2015) PF-06463922, an ALK/ROS1 Inhibitor, Overcomes Resistance to First and Second Generation ALK Inhibitors in Preclinical Models. Cancer Cell 28(1): 70-81.
-
Wei P, Qiu M, Lee N, Cao J, Wang H, et al. (2015) Abstract 764: Rational combination of PF-06463922 (next- generation ALK inhibitor) with PI3K pathway inhibitors overcomes ALKi resistance in EML4-ALK+ NSCLC models. Cancer Research 75(S 15): 764-764.
-
Gerber DE (2008) EGFR Inhibition in the Treatment of Non-Small Cell Lung Cancer. Drug Dev Res 69(6): 359- 372.
-
Schreiber AB, Winkler ME, Derynck R (1986) Transforming growth factor-alpha: a more potent angiogenic mediator than epidermal growth factor. Science 232(4755): 1250-1253.
-
Garcia J, Hurwitz HI, Sandler AB, Miles D, Coleman RL, et al. (2020) Bevacizumab (Avastin®) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treatment Reviews 86: 102017.
-
(2003) Tarceva Small Molecule EGFR-Tyrosine Kinase Inhibitor for Cancer. Clinical Trials Arena.
-
Duffy AM, David BH, Harmey JH (2013) Vascular Endothelial Growth Factor (VEGF) and Its Role in Non- Endothelial Cells: Autocrine Signalling by VEGF. Madame Curie Bioscience Database.
-
Tabernero J (2007) The role of VEGF and EGFR inhibition: implications for combining anti-VEGF and anti-EGFR agents. Mol Cancer Res 5(3): 203-220.
-
(2017) KRAS Gene. Medline Plus.
-
Sheridan C (2021) Oncologists greet Lumakras: the world’s first KRAS inhibitor. Nat Biotechnol 39(9): 1032- 1034.
-
Nasser NJ, Gorenberg M, Agbarya A (2020) First line Immunotherapy for Non-Small Cell Lung Cancer. Pharmaceuticals 13(11): 373.
-
(2021) Leading cancer drugs worldwide by revenue in 2020. Statista.
-
(2018) Press release: The Nobel Prize in Physiology or Medicine. The Nobel Assembly at Karolinska Institute.
-
Ribas A, Wolchok Jedd D (2018) Cancer immunotherapy using checkpoint blockade. Science 359(6382): 1350- 1355.
-
Fellner C (2012) Ipilimumab (yervoy) prolongs survival in advanced melanoma: serious side effects and a hefty price tag may limit its use. A peer-reviewed journal for formulary management 37(9): 503-530.
-
(2022b) Side effects may occur while taking KEYTRUDA. Merck.
-
Ascierto PA, Del Vecchio M, Mackiewicz A, Robert C, Chiarion-Sileni V, et al. (2020) Overall Survival at 5 Years of Follow-Up in a Phase III Trial Comparing Ipilimumab 10 Mg/Kg with 3 Mg/Kg in Patients with Advanced Melanoma. J Immunother Cancer 8(1): e000391.
-
Valero C, Lee M, Hoen D, Zehir A, Berger MF, et al. (2021) Response Rates to Anti-PD-1 Immunotherapy in Microsatellite-Stable Solid Tumors With 10 or More Mutations per Megabase. JAMA Oncol 7(5): 739-743.
-
Spencer CN, McQuade JL, Gopalakrishnan V, McCulloch JA, Vetizou M, et al. (2021) Dietary fiber and probiotics influence the gut microbiome and melanoma immunotherapy response. Science 374(6575): 1632- 1640.
-
Sharma P, Allison JP (2015) The future of immune checkpoint therapy. Science 348(6230): 56-61.
-
(2021) Merck Provides Update on KEYTRUDA® (pembrolizumab) Indication in Metastatic Small Cell Lung Cancer in the US. Merck.
-
(2017) Bristol-Myers Squibb and Ono Pharmaceutical Company Enter Settlement and License Agreement with Merck to Resolve PD-1 Antibody Patent Litigation. Bristol Myers Squibb.
-
(2017) Merck Announces Settlement and License Agreement Resolving KEYTRUDA® (pembrolizumab) Patent Litigation. Merck.
-
(2021) Japanese Nobel laureate settles with Ono Pharma over Opdivo suit. Nikkei Asia.
-
Normile D (2020) Nobel laureate Tasuku Honjo to sue Japanese drug firm for 22 billion yen.
-
Oliveres H, Caglevic C, Passiglia F, Taverna S, Smits E, et al. (2018) Vaccine and immune cell therapy in non-small cell lung cancer. Journal of Thoracic Disease 10(S13): S1602-S1614.
-
Giaccone G, Bazhenova LA, Nemunaitis J, Tan M, Juhasz E, et al. (2015) A phase III study of belagenpumatucel-L, an allogeneic tumour cell vaccine, as maintenance therapy for non-small cell lung cancer. Eur J Cancer 51(16): 2321-2329.
-
Saavedra D, Crombet T (2017) CIMAvax-EGF: A New Therapeutic Vaccine for Advanced Non-Small Cell Lung Cancer Patients. Front Immunol 8: 269.
-
Wei Q, Fang ZY, Zhang ZM, Zhang, TF (2021) Therapeutic tumor vaccines a rising star to benefit cancer patients. WArtificial Intelligence in Cancer 2(3): 25-41.
-
Vansteenkiste JF, Cho BC, Vanakesa T, De Pas T, Zielinski M, et al. (2016) Efficacy of the MAGE-A3 cancer immunotherapeutic as adjuvant therapy in patients with resected MAGE-A3-positive non-small-cell lung cancer (MAGRIT): a randomised, double-blind, placebo- controlled, phase 3 trial. The Lancet Oncology 17(6): 822-835.
-
Weng TY, Yen MC, Huang CT, Hung JJ, Chen YL, et al. (2014) DNA vaccine elicits an efficient antitumor response by targeting the mutant Kras in a transgenic mouse lung cancer model. Gene Ther 21(10): 888-896.
-
Remy-Ziller C, Thioudellet C, Hortelano J, Gantzer M, Nourtier V, et al. (2018) Sequential administration of MVA-based vaccines and PD-1/PD-L1-blocking antibodies confers measurable benefits on tumor growth and survival: Preclinical studies with MVA-βGal and MVA-MUC1 (TG4010) in a murine tumor model. Human Vaccines & Immunotherapeutics 14(1): 140-145.
-
Shah NN, Fry TJ (2019) Mechanisms of resistance to CAR T cell therapy. Nat Rev Clin Oncol 16(6): 372-385.
-
Hou AJ, Chen LC, Chen YY (2021) Navigating CAR-T cells through the solid-tumour microenvironment. Nat Rev Drug Discov 20(7): 531-550.
-
Li H, Huang Y, Jiang DQ, Cui LZ, He Z, et al. (2018) Antitumor activity of EGFR-specific CAR T cells against non-small-cell lung cancer cells in vitro and in mice. Cell Death & Disease 9(2): 177.
-
Meeks JJ, Al-Ahmadie H, Faltas BM, Taylor JA, Flaig TW (2020) Genomic heterogeneity in bladder cancer: challenges and possible solutions to improve outcomes. Nat Rev Urol 17(5): 259-270.
-
(2021) Lung Cancer Market Value Forecasted To Reach US$ 44,728.5 Million By 2027 Covering COVID-19 ERA: Acumen Research and Consulting.
-
Terry M (2017) 3 Top Drugmakers Leading Lung Cancer R&D Right Now. BioSpace.
-
Cameron F, Whiteside G, Perry C (2011) Ipilimumab: First Global Approval. Drugs 71(8): 1093-1104.
-
Cohen MH, Gootenberg J, Keegan P, Pazdur R (2007) FDA Drug Approval Summary: Bevacizumab (Avastin) Plus Carboplatin and Paclitaxel as First-Line Treatment of Advanced/Metastatic Recurrent Nonsquamous Non- Small Cell Lung Cancer. Oncologist 12(6): 713-718.
-
(2019) Patent expiry dates for biologicals: 2018 update. Generics and Biosimilars Initiative Journal 8(1): 24-31.
-
(2019) Pfizer Receives U.S. FDA Approval for Its Oncology Biosimilar, ZIRABEV™ (bevacizumab-bvzr). Pfizer.
-
(2022b) About MD Anderson. Cancer Center.
-
(2022) Cancer Research: University of Utah Huntsman Cancer Institute.
-
(2022) About Dana-Farber Cancer Institute. Dana- Farber Cancer Institute.
-
Robert M Davis (2022a) Merck.
-
Karen E Knudsen, MBA, PhD (2022) American Cancer Society.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer