Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
Penile squamous cell cancer (pSCC) is a rare tumor usually associated with an aggressive clinical course. We examined molecular landscape of 23 pSCC cases and correlated the results with HPV status and survival. All the tumors were tested for p16 immunohistochemical stain and human papilloma virus (HPV), high risk RNA in-situ hybridization studies. Fourteen of twenty-three patients (61%) harbored telomerase reverse transcriptase-promoter (TERT-p) alterations. All fourteen mutations occurred in HPV-independent tumors. Patients with TERT-p mutations did not impact OS (21 months vs. 33 months; Hazard ratio 1.129; p value 0.814) or CSS (16.5 months vs. 14 months. NOTCH1 mutation was detected in 5 tumors (22%) that were HPV-independent. Both the OS and CSS were significantly better in tumors harboring this mutation (75 months vs. 16 months; Hazard ratio 4.473; p value 0.0172 and 16 months vs. 6.5 months. All 5 NOTCH1 mutated tumors had TERT-p alterations. Fourteen (61%) patients had mutations involving TP53 gene. Although there was no difference in OS (21 months vs. 14 months; Hazard ratio 1.404; p value 0.53) between the patients with TP53 mutations compared to those without; the CSS was significantly better (17 months vs. 13 months; Hazard ratio 4.028; p value 0.0046). Twelve of the patients with TP53 mutations had alterations involving TERT-p and all the patients with NOTCH1 mutations had TP53 mutations in their tumors. In the present cohort, tumors with TERT-p and NOTCH1 mutations were HPV independent.
Abbreviations
pSCC: Penile Squamous Cell Cancer; HPV: Human Papilloma Virus; TERT-p: Telomerase Reverse Transcriptase- promoter; FFPE: Formalin Fixed Paraffin-embedded; IHC:
immunohistochemical; ISH: In-situ Hybridization; NGS: Next Generation Sequencing; OS: Overall Survival; CSS: Cancer Specific Survival; TCGA: Trans Cancer Genome Atlas; TMB: Tumor Mutational Burden; PeINs: Penile Intraepithelial Neoplasms; CLL: Chronic Lymphocytic Lymphoma.
Introduction
Penile squamous cell carcinoma (pSCC) is an uncommon but aggressive malignant neoplasm. It is estimated to have affected 2,050 males and caused 470 deaths in United States in 2023 [1]. pSCC can be broadly divided into human papilloma virus (HPV)-associated and HPV-independent. Approximately 30-50% of pSCC are associated with HPV infection [2]. There are differences as well as overlaps between the genomic landscape of HPV-associated and HPV- independent pSCCs, including more frequent mutations involving the TP53 gene in HPV-independent tumors [2, 3]. Therefore, it is important to study the genomic landscape of pSCCs to have a better understanding of the pathogenesis of HPV-associated and HPV-independent tumors and to identify prognostic and potential targetable biomarkers for therapy selection. Testing for genomic alterations is essential for selecting the most appropriate therapy for these patients which can be in the form of targeted therapies, immunotherapies, or clinical trials [4, 5, 6]. Herein we sought to study the molecular landscape of 23 patients of pSCC and correlate the results with HPV status and survival.
Materials and Methods
Patient and Cancer Characteristics
The institutional review board of our hospital approved this study. The study group consisted of 23 patients diagnosed with pSCC who had undergone treatment and for whom formalin fixed paraffin-embedded (FFPE) tissue blocks were available for additional analysis. Information regarding demographics, histopathological findings and clinical follow up was obtained from the medical records. The data extracted included age of the patient at diagnosis, histopathology of tumor, tumor grade, tumor stage, lymph node status, metastases, and survival.
p16ink4a Immunohistochemical Staining
Whole sections of the tumors from all 23 patients of pSCC were stained with p16 ink4a immunohistochemical (IHC) stain using mouse monoclonal antibody (Clone E6H4, prediluted) on the Ventana Benchmark Ultra using the optiview kit. Positive control included HPV-associated squamous cell carcinoma and negative control included benign tonsil tissue. The IHC staining for p16ink4a was interpreted as positive when a continuous strong nuclear and/or cytoplasmic staining of more than 70% of the tumor cells was present.
HPV RNA ISH Testing
High-risk HPV RNA in-situ hybridization (ISH) (subtypes 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82)) was performed on all 23 cases using the automated platform (Leicabond) using RNA scope kit with manufacturer’s instructions. Control tissue used were the cell lines that were formalin fixed, paraffin embedded, comprising of high-density cell line cores with a range of HPV high risk gene copy numbers besides tissue sections from known HPV-associated oropharyngeal SCCs and benign tonsil tissue. A positive HPV RNA ISH test result was defined as positive if any of the malignant cells showed brown punctate dot-like nuclear and/or cytoplasmatic positivity. A negative HPV RNA ISH test result was defined as negative if none of the malignant cells showed brown punctate dot-like nuclear and/or cytoplasmatic positivity.
Next Generation Sequencing (NGS) Assay
All 23 cases were subjected to NGS assay. A total of 324 cancer-associated genes were included in the targeted NGS analysis. H&E-stained section of the tissue block from every tumor was reviewed by a pathologist and used to assess adequacy (preferably more than 20% of tumor content). The assay employed a single DNA extraction method from FFPE tumor tissue sections. 50−1,000 ng of DNA underwent whole-genome shotgun library construction and hybridization-based capture of all coding exons from 309 cancer-related genes, including one promoter region, one non-coding (ncRNA), and select intronic regions from 34 commonly rearranged genes, 21 of which also included the coding exons [7].
Survival Analysis
Overall survival (OS) was defined as time between date of diagnosis to death or last follow-up and cancer specific survival (CSS) was defined as time between date of diagnosis to death due to penile cancer. The association of TERT- promoter, NOTCH1, TP53 and CDKN2A mutational status and categorical variables was examined using Fisher’s exact test; Kaplan-Meier plot (with Log-Rank p) and univariate cox proportional model and was applied to predict OS and CSS.
Results
Demographics, Clinicopathological Features
There were 23 patients of pSCC with age ranging from 28 years to 81 years (median age of 63 years). There were two patients with pT1 stage, three with pT2, fifteen with pT3 and only one with pT4 stage. In two patients the primary stage could not be determined as they presented with inguinal lymph node metastases. The nodal staging was as follows: pN0 = 1; pN1 = 4; pN2 = 2; pN3 = 15. Clinically lymph node metastasis was not suspected in one patient and therefore was never sampled. Two tumors were well differentiated, sixteen were moderately differentiated, and five were poorly differentiated. Eight tumors were p16 ink4a positive while fifteen were negative. Seven of these tumors were HPV-associated and sixteen were HPV-independent. Eight patients developed metastasis to distant organs (bone n = 4; lungs n = 3; appendix n = 1) on follow up.
Follow-up and Survival
Twenty-one patients (91%) received adjuvant therapy (chemotherapy n=13, and combined radiation and chemotherapy n= 8). Total follow up duration ranged from 5 months to 81 months with a median of 17 months. Fifteen patients (65%) died during follow-up of which thirteen (56.5%) died of disease.
HPV Testing
Seven tumors were positive for both p16 ink4a and high- risk HPV subtypes (16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82). One tumor which was positive for p16 ink4a was negative for HR HPV subtype. Remaining fifteen tumors were negative for both p16 ink4a and HR HPV subtype.
Molecular Findings
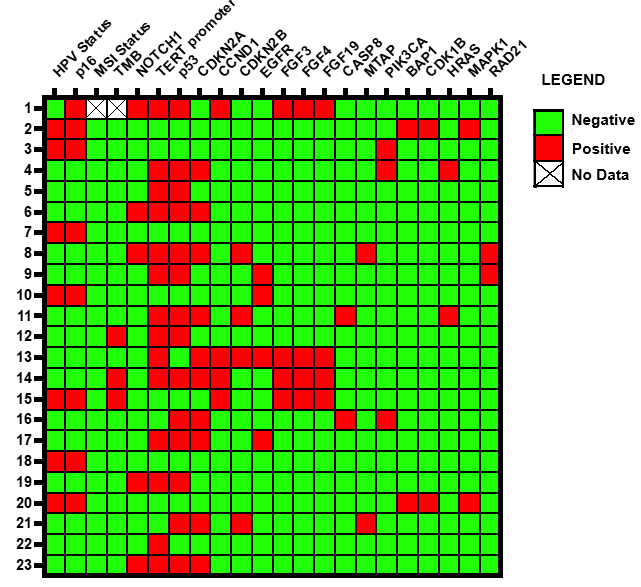
There were eighteen distinct pathogenic genomic alterations identified (Figure 1). Alterations in TP53 and telomerase reverse transcriptase-promoter (TERT-p) regions were most common and were present in 14 of 23 (61%) tumors. Mutations in TERT-p region involved the following: -124 C>T (n=9, 64%) and -146 C>T (n=4, 29%) and -138 C>T (n=1, 7%). All these mutations were mutually exclusive. Alterations involving CDKN2A (n=10; 43%), and NOTCH1 (n= 5; 22%) were present as well. Various histopathological parameters with the above-mentioned genomic alterations are described in Table 1. Twenty-two of twenty-three tumors (96%) had at least one pathogenic somatic driver mutation in the Hippo, Cell cycle, RTK/RAS, NOTCH, Nrf2, p53 and PI3K pathways curated by the trans cancer genome atlas (TCGA). Alterations in the Hippo, RTK/RAS and Cell Cycle pathways accounted for over 41% of all the alterations in our cohort. Mutations involving EGFR and PIK3CA genes were present in 4 (17%) and 3 (13%) cases respectively.
| Parameter | TERT-p Mutated (n=14) | TERT-p Wild Type (n=9) | NOTCH1 Mutated (n=5) | NOTCH1 Wild Type (n=18) | TP53 Mutated (n=14) | TP53 Wild Type (n=9) | CDKN2A Mutated (n=10) | CDKN2A Wild Type (n=13) |
|---|---|---|---|---|---|---|---|---|
| Stage | ||||||||
| pTX | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 1 |
| pT1 | 0 | 2 | 0 | 2 | 0 | 2 | 0 | 2 |
| pT2 | 2 | 1 | 1 | 2 | 3 | 0 | 2 | 1 |
| pT3 | 11 | 4 | 4 | 11 | 10 | 5 | 7 | 8 |
| pT4 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 |
| Lymph Node Status | ||||||||
| Nx/N0 | 1 | 1 | 0 | 2 | 0 | 2 | 0 | 2 |
| N1 | 4 | 0 | 1 | 3 | 3 | 1 | 3 | 1 |
| N2 | 0 | 2 | 0 | 2 | 1 | 1 | 1 | 1 |
| N3 | 9 | 6 | 4 | 11 | 10 | 5 | 6 | 9 |
| Metastatic | ||||||||
| M0 | 8 | 8 | 3 | 13 | 8 | 8 | 7 | 9 |
| M1 | 6 | 1 | 2 | 5 | 6 | 1 | 3 | 4 |
| Differentiation | ||||||||
| Well differentiated | 2 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Moderately differentiated | 8 | 8 | 2 | 14 | 9 | 7 | 9 | 7 |
| Poorly differentiated | 4 | 1 | 2 | 3 | 4 | 1 | 0 | 5 |
| HPV Status | ||||||||
| HPV-associated | 0 | 7 | 0 | 7 | 0 | 7 | 0 | 7 |
| HPV-independent | 14 | 2 | 5 | 11 | 14 | 2 | 10 | 6 |
Table 1: Histopathological Parameters in relation to TERT-p, NOTCH1, TP53 and CDKN2A Alterations.
Association of Tumor Mutational Burden (TMB) and TERT-p, NOTCH1, TP53 and CDKN2A Alterations with HPV Status
Tumor mutational burden (TMB) was high (≥10 mutations/ megabase) in three tumors (13%) which were HPV- independent. All twenty-three tumors were microsatellite stable. There were 14 cases with TERT-p mutations, and all of these occurred in HPV-independent setting. Majority (14 of 16; 87%) of HPV-independent tumors had TERT-p mutations. None of the HPV-associated tumors had TERT-p mutations (Table 2). There were 5 patients (22%) with NOTCH1 mutations that were present in HPV-independent tumors. None of the seven HPV-associated tumors harbored NOTCH1 mutations. Activating NOTCH1 mutations were present in two tumors (duplication exons 3-31 and duplication exons 9-33). Inactivating alterations (I567fs*69 frameshift, T805fs*70 frameshift and splice site 2468-1G>A splice site mutation) were present in three tumors.
- HPV/p16 Negative with
- TERT-p Mutations N
- (%)
- HPV/p16 Negative with TERT-p Wild-type
- N (%)
- HPV/p16 Positive with
- TERT-p Mutations N
- (%)
- Study (Total # of Penile SCCs)
- Kim, et al (n=34)
- 13 (38.2%)
- 7 (20.6%)
- 2 (5.9%)
- 12 (35.3%)
- Starita, et al
- (n=69)
- 25 (36.2%)
- 14 (20.3%)
- 12 (17.4%)
- 18 (26%)
- Canto, et al
- (n=30)
- NA
- NA
- 45% of 30
- 55% of 30
- Current Study
- (n=23)
- 14 (87.5%)
- 2 (12.5%)
- 0 (0%)
- 7 (100%)
Table 2: Association of HPV status in invasive penile SCCs with TERT promoter (TERT-p) mutations.
Correlation Between TERT-p, NOTCH1, TP53 and CDKN2A Alterations with Survival
Patients with TERT-p mutations did not demonstrate better OS or CSS compared to those without; median survival time with mutation was 21 months compared to 33 months without mutation (Hazard ratio 1.129 and log rank p value 0.814) for OS; and median survival time with mutation was 16.5 months compared to 14 months without mutation (Hazard ratio 1.470 and log rank p value 0.4536)
for CSS (Figure 2). Patients with TP53 mutations did not demonstrate better OS compared to those without; median survival time with mutation was 21 months compared to 14 months without mutation (Hazard ratio 1.404 and log rank p value 0.53). However, CSS was significantly better in TP53 mutated tumors compared to those without; median survival time with mutation was 17 months compared to 13 months without mutation (Hazard ratio 4.028 and log rank p value 0.0046) (Figure 2).
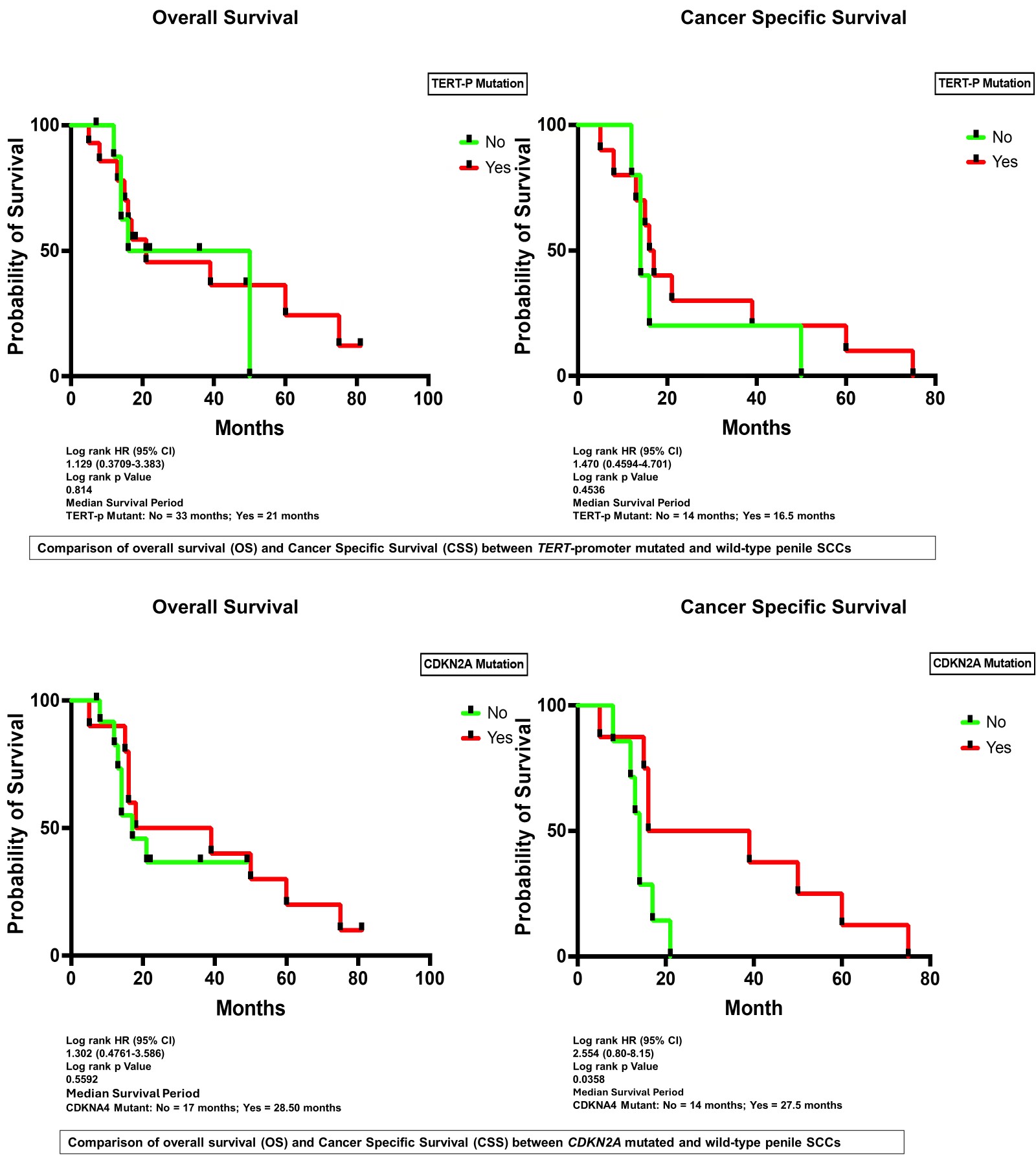
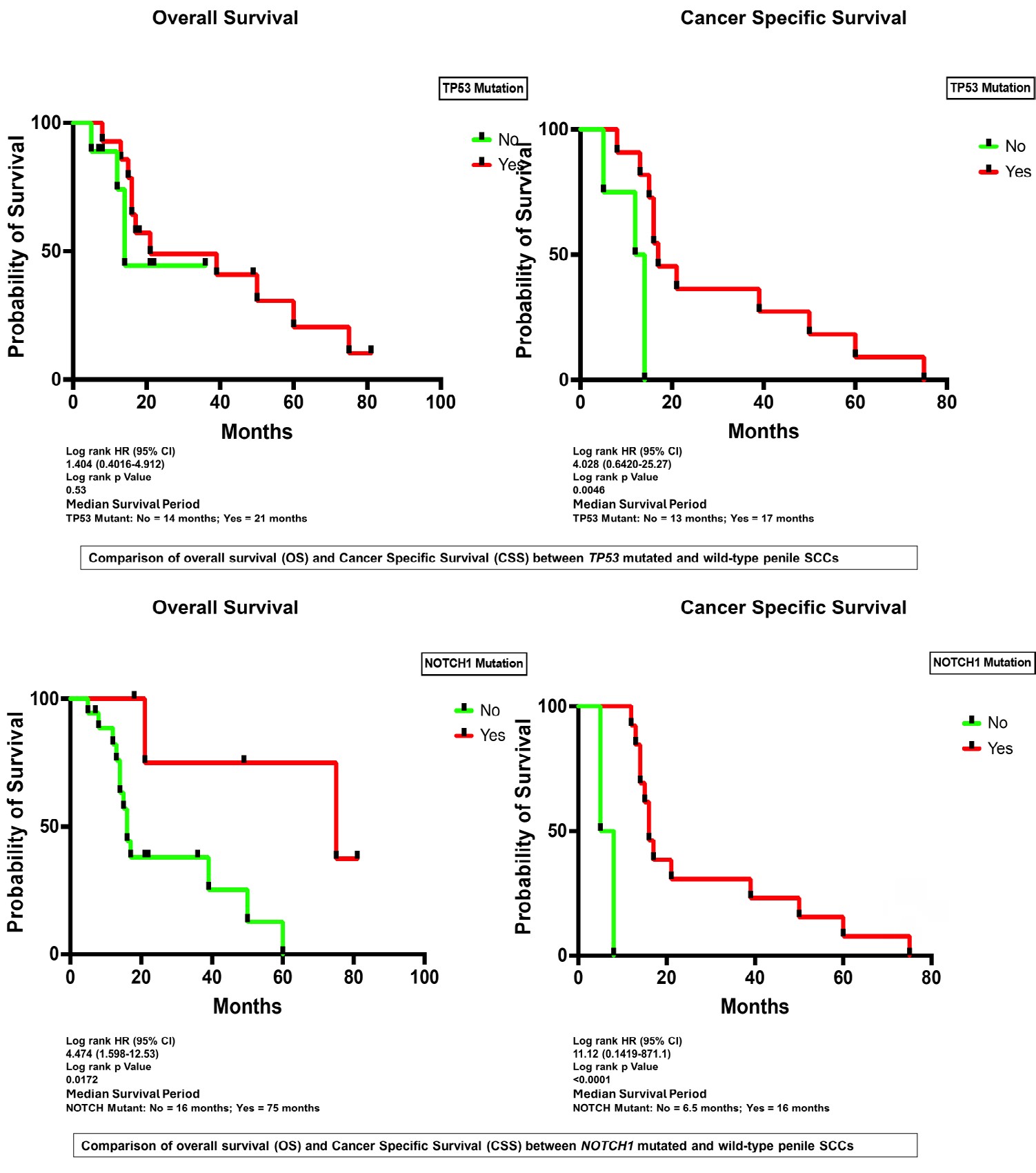
Patients with NOTCH1 mutations demonstrated better OS and CSS compared to those without; median OS time with mutation was 75 months compared to 16 months without mutation (Hazard ratio 4.474 and log rank p value 0.0172); and median CSS time with mutation was 16 months compared to 6.5 months without mutation (Hazard ratio 11.12 and log rank p value <0.0001) (Figure 2). Patients with CDKN2A mutations did not demonstrate better OS compared to those without; median survival time with mutation was 28.5 months compared to 17 months without mutation (Hazard ratio 1.302 and log rank p value 0.5592). However, CSS was significantly better in CDKN2A mutated tumors compared to those without; median survival time with mutation was 27.5 months compared to 14 months without mutation (Hazard ratio 2.554 and log rank p value 0.0358) (Figure 2).
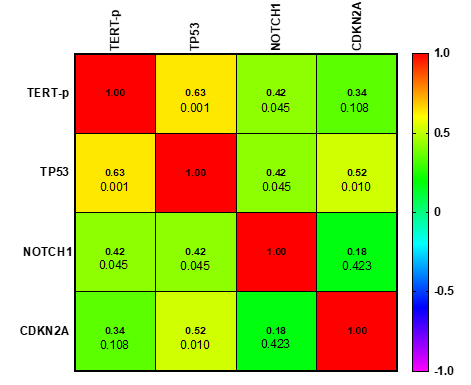
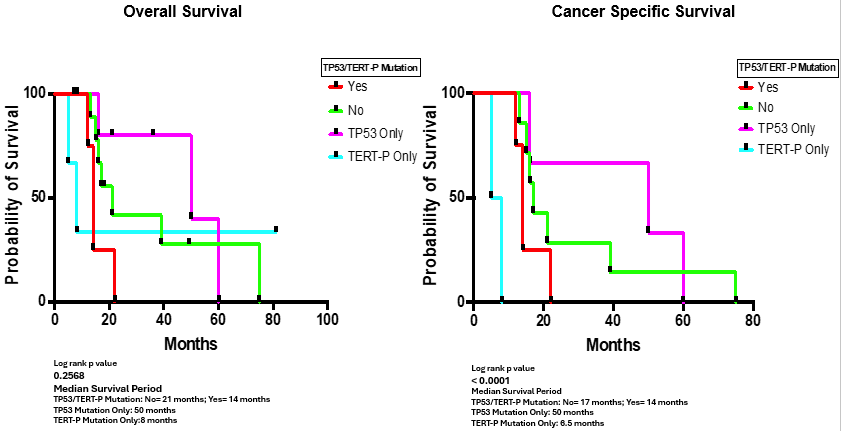
Figure 3 demonstrates the correlation matrix representing the association between co-occurrence of TERT-p, TP53, NOTCH1 and CDN2A alterations. The correlation between TERT-p and TP53 was the highest (r = 0.63). Further analysis of OS and CSS showed poor survival for patients with TERT-p alterations without TP53 mutations when compared to those with TP53 mutations without TERT-p alterations (median survival of 8 months compared to 50 months for OS with p value of 0.2568; median survival of 6.5 months compared to 50 months for CSS with p value of <0.0001) respectively (Figure 4).
Discussion
Telomerase activation is detectable in over 90% of human cancers [8, 9]. It is the most common fundamental step in tumorigenesis. Telomerase reverse transcriptase (TERT), as a catalytic subunit of telomerase, can be upregulated in cancer through several mechanisms including mutations in its promoter region, gene amplification, and rearrangements. Among these, TERT-promoter (TERT-p) mutation is the most common somatic event to achieve TERT upregulation [10]. TERT-p mutations have been reported in many malignant neoplasms [11].
Telomerase activity in squamous cell carcinoma of the penis was described by Alves et al in 2001 in majority (86%, 44 of 51) of their cases [12]. In addition, few more groups have recently reported TERT-p mutations in penile squamous cell carcinomas [13, 14]. In the North Korean cohort TERT-p mutations were present in 18 out of 37 (48.6%) tumors, including three penile intraepithelial neoplasms (PeINs) and was predominantly present in p16 negative tumors [13]. Similarly high rate (43%, 13 of 30) of TERT-p mutations has been described in HPV-independent compared to HPV- associated head and neck cancers (4.3%, 1 of 23) [15].
These findings are in concordance with our study where TERT-p mutations were detected in fourteen of twenty- three pSCCs (60.1%) all of which were HPV-independent. Fourteen of sixteen HPV-independent tumors in our cohort (87.5%) exhibited TERT-p mutations. None of the seven HPV-associated tumors had TERT-p mutations. In a study by Starita et al, TERT-p mutations were present in 37 of 69 (53.6%) pSCCs in their cohort. Although TERT-p mutations were more frequent in HPV-independent (25/39; 64%) tumors, 40% of their HPV-associated tumors (12/30) had TERT-p mutations. In a recent study by Canto et al, 45% of HPV-associated pSCCs in their cohort from Latin America had TERT-p mutations [16].
The reason for this discrepancy is unknown but could be due to small case numbers in various studies. Overall, it appears that TERT-p mutations are not infrequent in pSCCs, occur in both HPV-independent and HPV-associated tumors although more commonly in HPV-independent tumors. Our data supports the concept that mutations of TERT-p in HPV- independent tumors and high-risk HPV E6 protein in HPV- associated tumors, in the absence of TERT-p mutations, are responsible for telomerase activation [17, 18, 19, 20, 21]. Tumors with TERT-p mutations are usually associated with poor prognosis [22, 23, 24, 25, 26, 27]. However, in the study by Kim et al, pSCC patients with TERT-p mutations had longer disease-free survival (DFS) than those without. In our study, there was no significant difference in OS and CSS in patients with pSCC with TERT-p mutations.
TP53 was one of the most commonly (n=14) mutated genes in our cohort. As seen in many previous studies, all mutations involving TP53 gene were present in HPV- independent tumors. There was a strong correlation between TERT-p and TP53 genes. Twelve of 14 TERT-p mutated pSCCs harbored TP53 mutations and vice versa. TP53 mutated pSCCs had significantly better CSS. This finding contradicts many prior studies showing TP53 mutated pSCCs behave more aggressively [28, 29]. The small sample size of our cohort could be the reason for this discrepancy. Patients with TERT-p only mutations without TP53 mutations had less OS and CSS compared to patients with TP53 only mutations without TERT-p mutations.
NOTCH1 usually acts like a tumor suppressor gene in cancers, especially in head and neck and cutaneous squamous cell carcinomas where it can be found in both HPV-associated and HPV-independent cancers [30, 31]. HPV-associated carcinomas have been shown to directly downregulate NOTCH expression to inhibit the NOTCH pathway [27, 32, 33]. Downregulation in the NOTCH pathway may render cells sensitive to PI3K/mTOR inhibition [34].
In the genomic landscape of pSCCs, NOTCH1 alterations have been reported in 51 of 146 cases altogether with an overall frequency of 35% (range 13-50%) by five independent research groups [36, 37, 38, 39]. Our cohort had 5 cases (21.7%) with NOTCH1 alterations, three of which were inactivating. All tumors with NOTCH1 alterations were HPV-independent pSCCs. Ali, et al. [36] found NOTCH1 mutations in 25% (n=5) of their cohort of pSCC. Four of these mutations involved HPV- independent tumors. However, Canto et al found NOTCH1 mutations in 50% (15 of 30) of their HPV-associated tumors. Hence, NOTCH1 mutations are seen in both HPV-associated and HPV-independent pSCCs, although more commonly in HPV-independent tumors.
Tumors with NOTCH1 mutations, such as chronic lymphocytic lymphoma (CLL), breast cancers and esophageal squamous cell cancers are usually reported to carry poor prognosis [40, 41, 42]. However, superior survival has been reported in non-small cell lung cancer with NOTCH1 mutations treated with immune checkpoint blockade . In our cohort, pSSCs with NOTCH1 mutations had significantly better OS and CSS. Overall genomic assessment of tumors in our cohort suggested that all but one (96%) had at least one potential somatic driver alteration in the oncogenic signaling pathways (Hippo, Cell cycle, RTK/RAS, NOTCH, Nrf2, p53 and PI3K pathways) curated by TCGA. Alterations in the Hippo, RTK/RAS and Cell Cycle pathways accounted for over 41% of all the alterations in our cohort. This is noteworthy as pathways such as PI3K, and Hippo involving PIK3CA, and EGFR genes can serve as potential targets for therapy [5]. EGFR protein expression detected by immunohistochemistry is common in pSCC and can serve as a viable target for therapy [6].
Only three HPV-independent tumors (13%) in our cohort had a high TMB (10 or higher). All the twenty-three tumors analyzed were microsatellite stable. Tumors with TMB of 10 or higher are eligible for anti-PD-1 immune check point inhibitor, Pembrolizumab, irrespective of the primary site. It has been reported that up to 20% of patients with pSCC may be eligible for pembrolizumab based on high TMB [5]. Although, a higher percentage of HPV-associated pSCCs are thought to have high TMB, none of our HPV-associated pSCCs had a high TMB.
Conclusion
In summary, we describe molecular alterations in a cohort of 23 cases of pSCC with emphasis on more commonly occurring alterations involving TERT-p, TP53, CDKN2A and NOTCH1 genes and review their correlation with the HPV status and prognosis. We describe the association between co-occurrence of genomic alterations involving TERT-p, TP53, NOTCH1 and CDKN2A genes.
References
-
Rebecca L, Siegel RL, Miller KD, Wagle NS, Jemal A, et al. (2023) Cancer statistics. CA Cancer J Clin 73(1): 17-48.
-
Olesen TB, Sand FL, Rasmussen CL, Albieri V, Toft BG, et al. (2019) Prevalence of human papillomavirus DNA and p16INK4a in penile cancer and penile intraepithelial neoplasia: a systematic review and meta-analysis. Lancet Oncol 20(1): 145-158.
-
Nazha B, Zhuang T, Wu S, Brown JT, Magee D, et al. (2023) Comprehensive genomic profiling of penile squamous cell carcinoma and the impact of human papillomavirus status on immune-checkpoint inhibitor-related biomarkers. Cancer 129(24): 3884-3893.
-
Milbury CA, Creeden J, Yip WK, Smith DL, Pattani V, et al. Clinical and analytical validation of FoundationOne®CDx, a comprehensive genomic profiling assay for solid tumors. PLoS One 17(3): e0264138.
-
Kim NW, Piatyszek MA, Prowse KR, Harley CB, West MD, et al. (1994) Specific association of human telomerase activity with immortal cells and cancer. Science 266(5193): 2011-2015.
-
Shay JW, Bacchetti S (1997) A survey of telomerase activity in human cancer. Eur J Cancer 33(5): 787-791.
-
Colebatch AJ, Dobrovic A, Cooper WA. (2019) _TERT_ gene: its function and dysregulation in cancer. J Clin Pathol 72(4): 281-284.
-
Gaspar TB, Sá A, Lopes JM, Sobrinho-Simões M, Soares P, et al. (2018) Telomere Maintenance Mechanisms in Cancer. Genes (Basel) 9(5): 241.
-
Alves G, Fiedler W, Guenther E, Nascimento P, Campos MM, et al. (2001) Determination of telomerase activity in squamous cell carcinoma of the penis. Int J Oncol 18(1): 67-70.
-
Kim SK, Kim JH, Han JH, Cho NH, Kim SJ, et al. (2021) TERT promoter mutations in penile squamous cell carcinoma: high frequency in non-HPV-related type and association with favorable clinicopathologic features. J Cancer Res Clin Oncol 147(4): 1125-1135.
-
Starita N, Pezzuto F, Sarno S, Losito NS, Perdonà S, et al. (2022) Mutations in the telomerase reverse transcriptase promoter and PIK3CA gene are common events in penile squamous cell carcinoma of Italian and Ugandan patients. Int J Cancer 150(11): 1879-1888.
-
Morris, LGT,Chandramohan R, West L, Zehir A, Chakravarty D, et al. (2017) The Molecular Landscape of Recurrent and Metastatic Head and Neck Cancers: Insights from a Precision Oncology Sequencing Platform. JAMA Oncol 3: 244-255.
-
Canto LM, Silva DJM, Branco CPV, Silva DIM, Nogueira L, et al. (2022) Mutational Signature and Integrative Genomic Analysis of Human Papillomavirus-Associated Penile Squamous Cell Carcinomas from Latin American Patients. Cancers (Basel) 14(14): 3514.
-
Doorslaer VK, Burk RD (2012). Association between hTERT activation by HPV E6 proteins and oncogenic risk. Virology 433(1): 216-219.
-
Liu X, Dakic A, Zhang Y, Dai Y, Chen R, et al. (2009) HPV E6 protein interacts physically and functionally with the cellular telomerase complex. Proc Natl Acad Sci U S A 106(44): 18780-18785.
-
Katzenellenbogen R (2017) Telomerase Induction in HPV Infection and Oncogenesis. Viruses 9(7): 180.
-
Miller J, Dakic A, Chen R, Ceron PN, Dai Y, et al. (2013) HPV16 E7 protein and hTERT proteins defective for telomere maintenance cooperate to immortalize human keratinocytes. PLoS Pathog 9: e1003284.
-
McMurray HR, McCance DJ (2003) Human papillomavirus type 16 E6 activates TERT gene transcription through induction of c-Myc and release of USF-mediated repression. J Virol 77(18): 9852-9861.
-
Lee Y, Park CK, Park SH (2024) Prognostic Impact of _TERT_ Promoter Mutations in Adult-Type Diffuse Gliomas Based on WHO2021 Criteria. Cancers (Basel) 16(11): 2032.
-
Campos MA, Macedo S, Fernandes M, Pestana A, Pardal J, et al. (2019) TERT promoter mutations are associated with poor prognosis in cutaneous squamous cell carcinoma. J Am Acad Dermatol. 80(3): 660-669.e6.
-
Guo Y, Chen Y, Zhang L, Ma L, Jiang K, et al. (2022) TERT Promoter Mutations and Telomerase in Melanoma. J Oncol. 2022: 6300329.
-
Shuai H, Duan X, Zhou JJ, Liu Y, Wu T, et al .(2023) Effect of the TERT mutation on the prognosis of patients with urothelial carcinoma: a systematic review and meta- analysis. BMC Urol 23(1): 177.
-
Rusinek D, Pfeifer A, Cieslicka M, Kowalska M, Pawlaczek A, et al. (2020) _TERT_ Promoter Mutations and Their Impact on Gene Expression Profile in Papillary Thyroid Carcinoma. Cancers (Basel) 12(6): 1597.
-
Rampias T, Sasaki C, Psyrri A (2013) Molecular mechanisms of HPV induced carcinogenesis in head and neck. Oral Oncol 50(5): 356-363.
-
Das T, Zhong R, Spiotto MT (2021) Correction to: Notch Signaling and Human Papillomavirus-Associated Oral Tumorigenesis. Adv Exp Med Biol 1287: C1.
-
Wang NJ, Sanborn Z, Arnett KL, Bayston LJ, Liao W, et al. (2011) Loss-of-function mutations in Notch receptors in cutaneous and lung squamous cell carcinoma. Proc Natl Acad Sci U S A 108(43): 17761-17766.
-
Brimer N, Lyons C, Wallberg AE, Vande Pol SB (2012) Cutaneous papillomavirus E6 oncoproteins associate with MAML1 to repress transactivation and NOTCH signaling. Oncogene 31(43): 4639-4646.
-
Das T, Zhong R, Spiotto MT (2021) Notch Signaling and Human Papillomavirus-Associated Oral Tumorigenesis. Adv Exp Med Biol 1287: 105-122.
-
Ali SM, Pal SK, Wang K, Palma NA, Sanford E, et al. (2016) Comprehensive Genomic Profiling of Advanced Penile Carcinoma Suggests a High Frequency of Clinically Relevant Genomic Alterations. Oncologist 21(1): 33-39.
-
Wang Y, Wang K, Chen Y, Zhou J, Liang Y, et al. (2019) Mutational landscape of penile squamous cell carcinoma in a Chinese population. Int J Cancer 145(5): 1280-1289.
-
Canto LM, Silva DJM, Branco CPV, Silva DIM, Nogueira L, et al. (2022) Mutational Signature and Integrative Genomic Analysis of Human Papillomavirus-Associated Penile Squamous Cell Carcinomas from Latin American Patients. Cancers (Basel) 14(14): 3514.
-
Chahoud J, Netto GFO, McCormick BZ, Rao P, Lu X, et al. (2021) Eterovic AK, Pickering CR, Pettaway CA. Whole- exome Sequencing in Penile Squamous Cell Carcinoma Uncovers Novel Prognostic Categorization and Drug Targets Similar to Head and Neck Squamous Cell Carcinoma. Clin Cancer Res 27(9): 2560-2570.
-
Cao J, Yang CH, Han WQ, Xie Y, Liu ZZ, et al. (2021) Correlation Between the Evolution of Somatic Alterations During Lymphatic Metastasis and Clinical Outcome in Penile Squamous Cell Carcinoma. Front Oncol 11: 641869.
-
Chahoud, J,Pickering CR, Pettaway CA (2019) Genetics and penile cancer: Recent developments and implications. Curr. Opin. Urol 29: 364-370.
-
Chen YL, Lee KT, Wang CY, Shen CH, Chen SC, et al. (2022) Low expression of cytosolic NOTCH1 predicts poor prognosis of breast cancer patients. Am J Cancer Res 12(5): 2084-2101.
-
Willander K, Dutta RK, Ungerbäck J, Gunnarsson R, Juliusson G, et al. (2013) NOTCH1 mutations influence survival in chronic lymphocytic leukemia patients. BMC Cancer 13: 274.
-
Zhou X, Bao W, Zhu X, Wang D, Zeng P, et al. (2024) Molecular characteristics and multivariate survival analysis of 43 patients with locally advanced or metastatic esophageal squamous cell carcinoma. J Thorac Dis 16(3): 1843-1853.
-
Huang Q, Cao H, Yao Q, Zhou X, Li H, et al. (2023) _NOTCH1_ Mutations Predict Superior Outcomes of Immune Checkpoint Blockade in Non-Small Cell Lung Cancer. Immunotargets Ther 12: 165-173.
-
Pagliaro LC, Tekin B, Gupta S, Hernandez HL (2024) Therapeutic Targets in Advanced Penile Cancer: From Bench to Bedside. Cancers (Basel) 16(11): 2086.
-
McDaniel AS, Hovelson DH, Cani AK, Liu CJ, Zhai Y, et al. (2015) Genomic Profiling of Penile Squamous Cell Carcinoma Reveals New Opportunities for Targeted Therapy. Cancer Res 75: 5219-5227.
-
Kashofer K, Winter E, Halbwedl I, Thueringer A, Kreiner M, et al. (2017) HPV-negative penile squamous cell carcinoma: disruptive mutations in the TP53 gene are common. Mod Pathol 30(7): 1013-1020.
-
Stoehr R, Weisser R, Wendler O, Giedl J, Daifalla K, et al. (2018) _P53_ Codon 72 Polymorphism and Risk for Squamous Cell Carcinoma of the Penis: A Caucasian Case-Control Study. J Cancer 9(22): 4234-4241.
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet
- Pediatric Sinonasal Ewing Sarcoma