Rare Case: Hidatid Cyst of Heart and CT Images
30 year old female had severe coughing and arrhythmia. Radiological assessment including Computerized Tomography were carried out. We diagnosed it as hydatid cysts involvement of pulmonary artery, heart and lung. Conclusion: Hydatid disease primarily affects the liver and typically demonstrates well-known, characteristic imaging findings. However, there are many potential local complications, and secondary involvement due to hematogenous dissemination may be seen in almost any anatomic location. The imaging method used depends on the involved organ and the growth stage of the cyst.
Introduction
Hydatid disease (HD) is a parasitic and endemic in many parts of the world. HD can involve almost anywhere in the body and demonstrates a variety of imaging features that vary according to growth stage [1]. Chest radiography, ultrasonography (US), computed tomography (CT), magnetic resonance (MR) imaging, and even urography can use for diagnosis. Radiologic findings range from purely cystic lesions to a completely solid appearance. Calcification is more common in HD of the liver. HD can become wide in compressible organs. Hydatid cysts (HCs) can be multiple. The imaging method used depends on the involved organ and the growth stage of the cyst. US most clearly demonstrates the hydatid sands in purely cystic lesions, as well as floating membranes, daughter cysts, and vesicles. CT is best for detecting calcification and revealing the internal cystic structure posterior to calcification. MR imaging is especially helpful in detecting HCs of the central nervous system. Radiologic Findings HCs are classified into four types on the basis of their appearance [1]. Type I: Simple Cyst appear as a well-defined anechoic mass with or without hydatid sand and septa. Unilocular cysts are considered to be an initial stage in the development of the parasitetidosis as opposed to nonparasitic cysts in the liver and lungs. Type II: Cyst with Daughter Cyst(s) and Matrix Daughter cysts are seen inside the mother cyst. Floating membranes or vesicles can also be seen in the cyst. Sometimes multiple cysts and echogenic areas that are enclosed together within a single capsule give rise to a “racemose” or “wheel spoke” appearance. Consolidation of the daughter cysts may produce echogenic solid lesions. At CT, type II HCs can be visualized in three stages depending on the age, number, and arrangement of the daughter cysts. Type IIA lesions contain round daughter cysts arranged at the periphery. The average CT attenuation of the mother cyst is higher than that of daughter cysts. Type IIB lesions contain larger, irregularly shaped daughter cysts that occupy almost the entire volume of the mother cyst. The high-attenuation fluid that surrounds the daughter cysts within the mother cyst looks like septa, creating a “rosette” appearance. Type IIC lesions appear at CT as relatively high-attenuation round or oval masses with scattered calcifications and occasional daughter cysts. These findings represent the degeneration of old cyst with amorphous and tenacious content. Type III: Calcified Cyst Type III lesions are dead cysts with total calcification. They demonstrate strong posterior shadowing at ultrasonography (US) and manifest as round, hyper attenuating areas at CT. Type IV: Complicated HC include rupture and super infection and may be seen in both type I and type II HCs. Rupture occurs in 50%–90% of cases. Cyst rupture is mainly due to the degeneration of parasitic membranes as a result of age, chemical reactions, or a host defense mechanism .HC rupture may be contained, communicating, or direct. In contained rupture, undulating membrane resulting from separation of the endocyst from the pericyst is seen at both US and CT and manifests as postural changes. A “snowstorm” pattern has been described at US [1].
Case Report
Our patient is a young woman which has cyst hidatic disease. Our patient had severe coughing and arrhythmia. CT shows cistic lesions in inferior heart wall and lung parenchym. Type of cysts were found to be compatible type 1 hydatid cysts. Numerous cyst hydatid lesions were observed in the lungs in CT images and these lesions were observed to be of type 1 character. In some of the hydatid cysts in the lung, air fluid level was observed and these cysts were thought to have been opened in the bronchioles Figure
- In addition, a hydatid cyst of a similar nature was observed in the heart and pericardium Figure
- On CT, cyst hydatid cysts were observed to have low densities and type 1 character. The most interesting one, and the more uncommon one, is that the hydatid cyst has infected the left pulmonary artery Figure
- Possible source of lesions in the lung.
This case is a rare hydatid cyst with heart, lung and pulmonary artery,
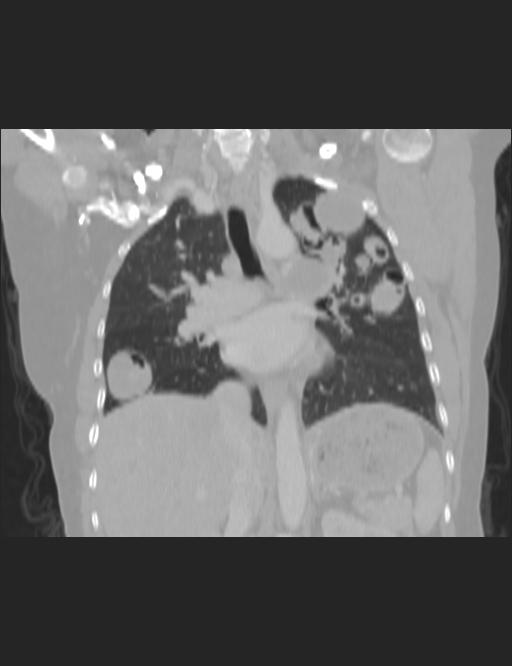
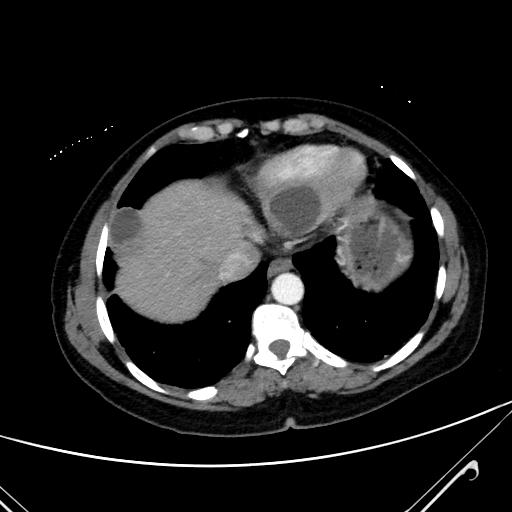
Figure 2a: Tip 1 cyst hidatic of heart and pericardium in axial intravenous non-ionic contrast-enhanced mediastinal window thorax CT (arrow).
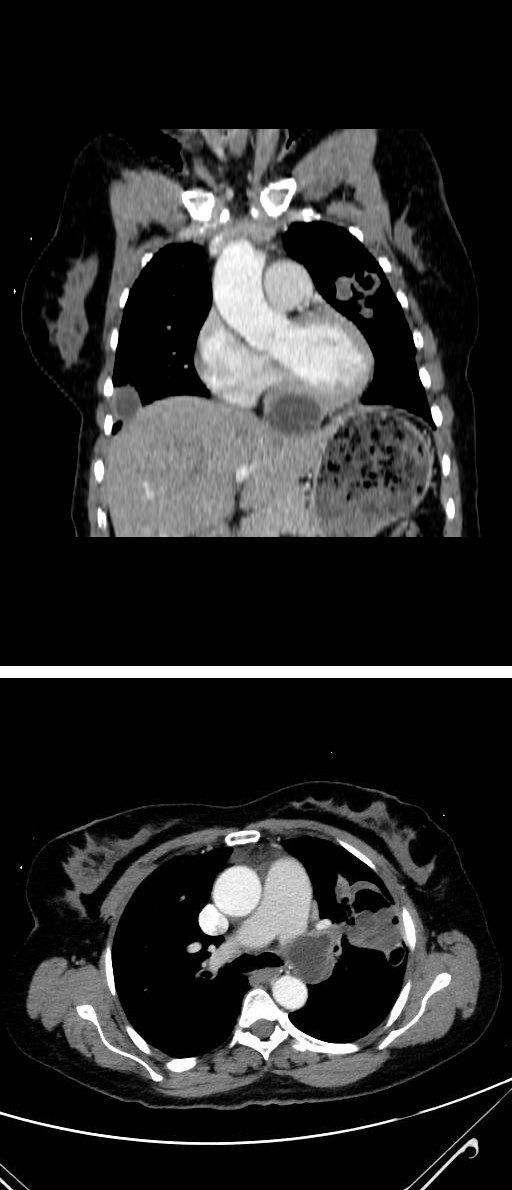
Figure 2b: Tip 1 cyst hidatic of heart and pericardium in coronal intravenous non-ionic contrast-enhanced mediastinal window thorax CT (arrow).
Conclusions
Hydatid disease primarily affects the liver and typically demonstrates well-known, characteristic imaging findings. However, there are many potential local complications, and secondary involvement due to hematogenous dissemination may be seen in almost any anatomic location. Familiarity with atypical manifestations of hydatid disease may be helpful in making a prompt, accurate diagnosis [2]. The lung is the second most common site of hematogenous spread in adults and probably the most common site in children (15%– 25% of cases). Heart HD is very rare (0.02%–2% of cases) and may be due to hematogenous spread or rupture of a lung HC [1]. Despite the characteristic imaging findings, HD in unusual anatomic locations may make differential diagnosis difficult, even in patients from endemic regions [2]. The value of our case is that the cysts of the hydatid disease keep the heart, lung and pulmonary arteries together. In addition, we see once again the superiority of multislice CT in both anatomical detail and diagnostic accuracy.
References
-
Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, et al. (2003) Hydatid disease from head to toe. Radiographics 23(2): 475-494.
-
Pedrosa I, Saíz A, Arrazola J, Ferreirós J, Pedrosa CS (2000) Hydatid disease: radiologic and pathologic features and complications. Radiographics 20(3): 795-817.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage