Abdominopelvic Actinomycosis: Radiographic Features
Actinomycosis is a chronic granulomatous disease caused by Actinomyces israelii bacteria. The abdominopelvic disease accounts for only 20% of its clinical presentation. Both clinical presentation and imaging findings of this entity are nonspecific and frequently misdiagnosed by many clinicians. Although several cases of abdominal and pelvic actinomycosis have been reported in the literature, only a few described their radiographic features. We present ultrasound and computed tomography findings of histologically proven abdominal actinomycosis in a 25-year-old African female.
Case Report
A 25-year-old African female not known to have any medical illnesses presented herself to the emergency department with a chief complaint of right lower quadrant pain, night sweats, and fatigue for two weeks. Her pain was a moderate, continuous, dull aching localized to the right lower abdomen, which was getting worse over the last two days. Physical examination showed normal vital signs and tenderness to palpation in the right lower quadrant and groin exaggerated by hip extension. Her initial laboratory results showed a slightly elevated leukocytic count of 13.0 x 109/L (normal range 4.00-11.0 x 109/L) and low hemoglobin (HB) level measured 9 g/dL (normal range 12.0 to 15.5 g/dL). The patient referred to the radiology department for further evaluation. Ultrasound of abdomen and pelvis was initially performed, which demonstrated a complex heterogeneous mass at the right iliac fossa involving the right iliopsoas muscle. The iliopsoas muscle was enlarged and showed increased flow on color Doppler images (Figure 1).
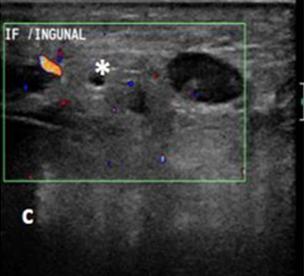

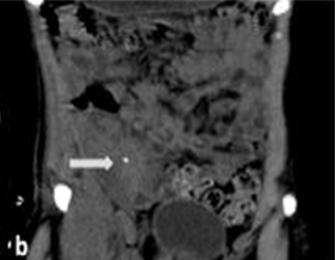
Figure 1: Ultrasound of a 25-year-old female with abdominal actinomycosis. Findings: (a,b): Longitudinal and transverse transabdominal B-mode ultrasound images through the right iliac fossa and inguinal region demonstrate complex heterogeneous collection involving the right iliopsoas muscle (asterisks). (c): Transverse transabdominal color Doppler ultrasound image of the same area shows increased regional flow (asterisks). Technique: US (Philips iU22), linear transducer, 12 MHz. Subsequent unenhanced computed tomography (CT) scan of the abdomen and pelvis revealed an ill-defined, inflammatory soft-tissue mass in the right lower quadrant involving the cecum and invading the adjacent iliopsoas and lower anterior abdominal wall muscles. The mass

showed central calcific density. There was associated retroperitoneal lymphadenopathy (Figure 2). The initial differential diagnosis based on the clinical and imaging findings included inflammatory appendicular mass, inflammatory bowel disease, and tuberculosis.

The patient underwent surgery and tissue samples were obtained from the retroperitoneal lymph nodes. The samples were sent for histopathological evaluation which revealed bacterial filamentous colonies surrounded by neutrophils with suppurative inflammation and focal granulomatous and prominent exanthematous reaction diagnostic for actinomycosis (Figure 3).
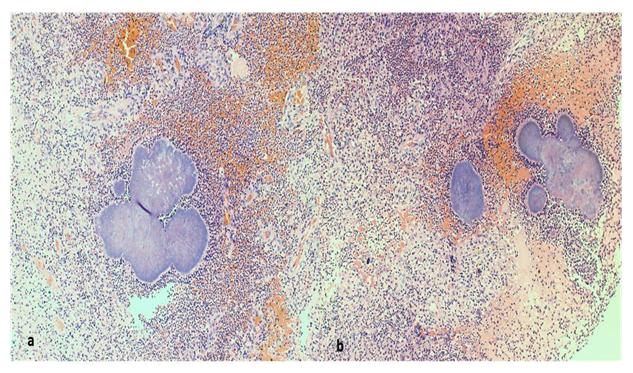
Findings: (a,b): Retroperitoneal lymph nodes show bacterial filamentous colonies surrounded by neutrophils with suppurative inflammation and focal granulomatous and prominent exanthematous reaction hematoxylin and eosin (H&E), high power (10x). After which the patient was initiated on a four-week regimen of penicillin G, intravenously prior to the transition to oral antibiotics. She showed significant clinical improvement, so no additional imaging was required.
$$ \| $$
Discussion
Etiology & Demographics
Actinomycosis is a rare chronic granulomatous infection, which can mimic other inflammatory diseases. Actinomyces israelii is a gram-positive anaerobic organism which is considered to be a normal endogenous flora of the oral cavity, gastrointestinal and genital tracts [1]. The abdominopelvic region is involved in 20% of actinomycosis cases, third in rank following the cervicofacial (50%-65%) and thoracic regions (15%- 30%) [2]. It is approximately three times more common in males than in females, even though it is linked to several cases in association with the use of intrauterine contraceptive devices (IUCDs) [3].
$$ \| $$ Abdominal actinomycosis usually happens after disruption of the mucosal barrier following appendicitis, diverticulitis, surgical procedure or penetrating trauma [3]. Many abdominal organs can be involved including the gastrointestinal tract, ovaries, and liver, yet the ileocecal region and its surrounding structures are most commonly affected by this infection (Table 1) [4, 5].
Clinical & Imaging Findings
Both clinical presentation and imaging findings of this entity are nonspecific and frequently misdiagnosed by many clinicians. Most patients present with nonspecific constitutional symptoms such as chronic low-grade fever, weight loss, and night sweats, which can remain undetected for months to years [6]. The imaging findings of abdominal actinomycosis are also nonspecific, yet the important radiologic feature of abdominopelvic actinomycosis is the aggressive infiltrative nature and its tendency to cross natural anatomic barriers.
The barium study is not frequently used in diagnosing these cases due to its inability to asses for extraluminal involvement. The radiographic findings include mural invasion with stricture formation, mass effect with luminal narrowing, and thickened mucosal folds. Ultrasound might be used in the initial assessment as in our case which demonstrates mixed echogenicity complex mass. On the other hand, CT scan is the most useful modality for determining the anatomic location and the extent of disease. The most frequently reported features are concentric enhancing bowel wall thickening, peritoneal masses, and inflammatory fat infiltration that has a tendency to cross the soft tissue planes associated with abscesses. Regional lymphadenopathy and ascites are minimal or absent [7, 8]. In a recent retrospective study, Lee, et al. analyzed CT scans in 18 patients with pathologically proven abdominopelvic actinomycosis, the majority of them were diagnosed postoperatively. The sigmoid colon was most commonly affected (50%), bowel wall thickening was seen in all patients and (17/18) patients showed pelvic or peritoneal masses [9]. Unfortunately, in our study and other studies from literature most actinomycosis cases are diagnosed postoperatively. The most important CT clue for the correct diagnosis in our study was a large inflammatory infiltrative mass at the ileocecal junction. The definite diagnosis is based on the histopathological identification of the actinomycotic granule or culture of the Actinomyces or both. However, the success rate of recovery of bacteria by culture is less than 50% and the granules are often scarce in the specimens [7].
Treatment & Prognosis
The mainstay treatment for abdominal actinomycosis is a high dose of intravenous penicillin G followed by oral antibiotics. The prognosis is good, though some cases may require treatment for up to 18 months. Surgery is required only in complicated cases [10, 11].
| Actinomyces israelii | |
| Incidence | Rare |
| Gender ratio | Male to female 3:1 |
| Age predilection | No |
| Risk factors | Appendicitis, diverticulitis, surgical procedure or penetrating trauma. |
| Treatment | Intravenous penicillin G followed by oral antibiotics |
| Prognosis | Good |
| Findings on imaging | Concentric enhancing bowel wall thickening, peritoneal masses, and inflammatory fat infiltration that have a tendency to cross the soft tissue plane associated with abscesses. |
Table 1: Summary table
Differential Diagnoses
The main differential considerations towards a large inflammatory infiltrative mass at the right iliac fossa are intestinal TB, Crohn disease, and malignant tumors (Table 2).
| Entity | Barium study findings | Computed tomography findings | ||||||
|---|---|---|---|---|---|---|---|---|
| Abdominal actinomycosis | Mural invasion with stricture formation, mass effect with narrowing of the lumen, and thickened mucosal folds. | Concentric enhancing bowel wall thickening, peritoneal masses, and inflammatory fat infiltration that has a tendency to cross the soft tissue planes associated with abscesses. Regional lymphadenopathy and ascites are minimal or absent. | ||||||
| Intestinal tuberculosis | Short, concentric and smooth stricture with significant pre- stenotic dilatation. | Mural thickening with contiguous ileocecal involvement, hypodense lymph nodes with peripheral enhancement. |
Table 2: Differential table. Intestinal Tuberculosis: Abdominal tuberculosis accounts for 11-16% of extrapulmonary tuberculosis.
| Crohn disease | Long, eccentric stricture with sacculations at the anti-mesenteric border and without significant pre-stenotic dilatation. Aphthous ulcers and skip lesions. | Mural thickening with stratification and vascular engorgement of the mesentery seen with active inflammation. Mesenteric fibrofatty proliferation, fistulae, and anorectal disease are frequently seen. |
| Complicated Colonic Cancer | A short segment of irregular narrowing with an abrupt transition (apple core sign). | Marked asymmetric wall thickening with loss of stratified enhancement that involves a short segment of the colon. The presence of pericolic lymphadenopathy. |
| Carcinoid | Solitary or multifocal, smooth, rounded nodules or mucosal elevations in the distal ileum. A fixed, rigid, curved segment of small intestine might be seen. | Asymmetric or concentric mural thickening of the small intestine and a desmoplastic submucosal fibrosis. Calcification and mesenteric lymph node metastases are usually seen. |
Table 3: Differential table. Intestinal Tuberculosis: Abdominal tuberculosis accounts for 11-16% of extrapulmonary tuberculosis.
Table 2: Differential table. Intestinal Tuberculosis: Abdominal tuberculosis accounts for 11-16% of extrapulmonary tuberculosis. It can involve the intestine, peritoneum, lymph nodes, or solid abdominal organs. Terminal ileum and ileocecal junction are the most commonly involved sites. Strictures are the most common finding in intestinal TB and are typically short, concentric and smooth in outline with significant pre-stenotic dilatation. At CT scans mural thickening with contiguous ileocecal involvement is the most frequent finding. The presence of hypodense lymph nodes with peripheral enhancement in the mesentery and retroperitoneum are helpful to reach a diagnosis [12, 13]. Crohn disease: As with intestinal TB, the ileocecal region is the most commonly affected site, yet isolated involvement of ileocecal junction not seen in Crohn disease. Strictures are usually long, eccentric with sacculations at the anti-mesenteric border and without significant pre-stenotic dilatation. At barium study aphthous ulcers and skip lesions are pathognomonic. At computed tomography mural thickening with stratification and vascular engorgement of the mesentery are seen with active inflammation. Mesenteric fibrofatty proliferation, fistulae, and anorectal disease are frequently encountered findings [12, 13]. Complicated colonic cancer: A perforation complicates colonic CA in 2.5-10% of patients. If perforation or abscess is present in patients with colon cancer, CT finding of severe pericolic fat stranding is seen similar to any other benign inflammatory conditions. The presence of marked asymmetric wall thickening with loss of stratified enhancement that involves a short segment of the colon with an abrupt transition from a normal to an abnormal bowel wall favors the diagnosis of an underlying malignancy. The presence of pericolic lymphadenopathy more commonly detected in colon cancer [14]. Carcinoid: The small intestine is the most common location for gastrointestinal carcinoids followed by the rectum, and the appendix. Small solitary carcinoid is typically not detected on CT scans instead, it may manifest as asymmetric or concentric mural thickening of small intestine secondary to an infiltrating tumor and a desmoplastic submucosal fibrosis. Calcification is detected in 70% of mesenteric lymph node metastases. Fluoroscopic barium evaluation of the small bowel reveals solitary or multifocal, smooth, rounded nodules or mucosal elevations in the distal ileum. A fixed, rigid, curved segment of small intestine might be seen. The appendiceal carcinoid may manifest as appendicitis or a focal soft-tissue mass within the appendix on CT scans [15].
Teaching Point
Abdominal actinomycosis is a rare infection, yet to avoid unnecessary surgical intervention in these patients it should be included in the differential diagnosis of a patient who presents with certain radiographic features. The most commonly reported CT findings are concentric enhancing bowel wall thickening, peritoneal masses, and an inflammatory fat infiltration that has a tendency to cross the soft tissue planes associated with abscesses.
References
-
Russo TA. Agents of actinomycosis (2010) _In:_ Mandell GL, Bennett JE, Dolin R (Eds.) Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. 7th (Edn.), Philadelphia, Churchill Livingstone, pp: 3209-3219.
-
Bennhoff DF (1984) Actinomycosis: diagnostic and therapeutic considerations and a review of 32 cases. Laryngoscope 94(9): 1198-1217.
-
Garner JP, Macdonald M, Kumar PK (2007) Abdominal actinomycosis. Int J Surg 5(6): 441-448.
-
Berardi RS (1979) Abdominal actinomycosis. Surg Gynecol Obstet 149(2): 257-266.
-
Schmidt P, Koltai JL, Weltzein A (1999) Actinomycosis of the appendix in childhood. Pediatr Surg Int 15(1): 63-65.
-
Pusiol T, Morichetti D, Pedrazzani C, Ricci F (2011) Abdominal-pelvic actinomycosis mimicking malignant neoplasm. Infect Dis Obstet Gynecol 2011: 747059.
-
Ha HK, Lee HJ, Kim H, Ro HJ, Park YH, et al. (1993) Abdominal actinomycosis: CT findings in 10 patients. AJR Am J Roentgenol 161(4): 791-794.
-
Cintron JR, Del Pino A, Duarte B, Wood D, et al. (1996) Abdominal actinomycosis. Dis Colon Rectum 39(1): 105-108.
-
Lee IJ, Ha HK, Park CM, Kim JK, Kim JH, et al. (2001) Abdominopelvic actinomycosis involving the gastrointestinal tract: CT features. Radiology 220(1): 76-80.
-
Sung HY, Lee IS, Kim SI, Jung SE, Kim SW, et al. (2011) Clinical Features of Abdominal Actinomycosis: A 15- year Experience of A Single Institute. J Korean Med Sci 26(7): 932-937.
-
Smith AJ, Hall V, Thakker B, Gemmell CG (2005) Antimicrobial susceptibility testing of Actinomyces species with 12 antimicrobial agents. J Antimicrob Chemother 56(2): 407-409.
-
Pulimood AB, Amarapurkar DN, Ghoshal U, Phillip M, Pai CG, et al. (2011) Differentiation of Crohn’s disease from intestinal tuberculosis in India in 2010. World J Gastroenterol 17(4): 433-443.
-
Sharma R, Madhusudhan KS, Ahuja V (2016) Intestinal tuberculosis versus Crohn's disease: Clinical and radiological recommendations. Indian J Radiol Imaging 26(2): 161-172.
-
Kim SW, Shin HC, Kim IY, Kim YT, Kim CJ, et al. (2010) CT findings of colonic complications associated with colon cancer. Korean J Radiol 11(2): 211-221.
-
Levy AD, Sobin LH (2007) Gastrointestinal Carcinoids: Imaging Features with Clinicopathologic Comparison. Radiographics 27(1): 237-257.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage