Three-Dimensional Computed Tomographic Angiography (3DCTA) for the Diagnosis and Endovascular Treatment of a Ruptured Intercostal Artery Aneurysm Complicated By Neurofibromatosis Type 1
A 52-year-old man with neurofibromatosis type 1 (NF1) presented with sudden dyspnea and chest pain because of a spontaneous massive hemothorax. Three-dimensional computed tomographic angiography (3DCTA) revealed an intercostal artery aneurysm. We performed endovascular treatment using coils for aneurysmal embolization. The patient was discharged from the hospital without any complications and remains free of symptoms after 19 months.
Introduction
Neurofibromatosis type 1 (NF1), also known as Von
Recklinghausen’s disease, is a hereditary autosomal dominant disorder characterized mainly by café au lait spots and cutaneous neurofibromas. NF1 may also involve vascular, bone, or ocular lesions. The incidence of concomitant vascular disease is only 3.6%, and arterial aneurysm, rupture, stenosis, and arteriovenous fistula have been reported [1]. These arterial lesions are caused by arterial fragility [2]. Spontaneous rupture of a major artery is extremely uncommon. Here, we report an NF1 patient who had spontaneous rupture of an intercostal artery with massive hemothorax.
Patient Presentation
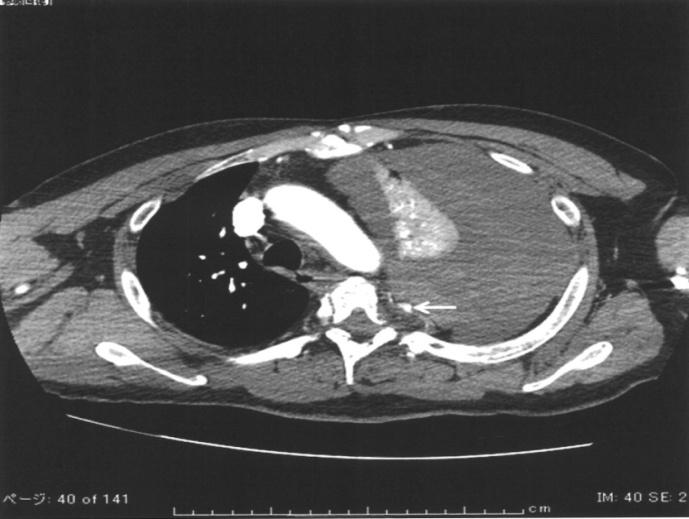
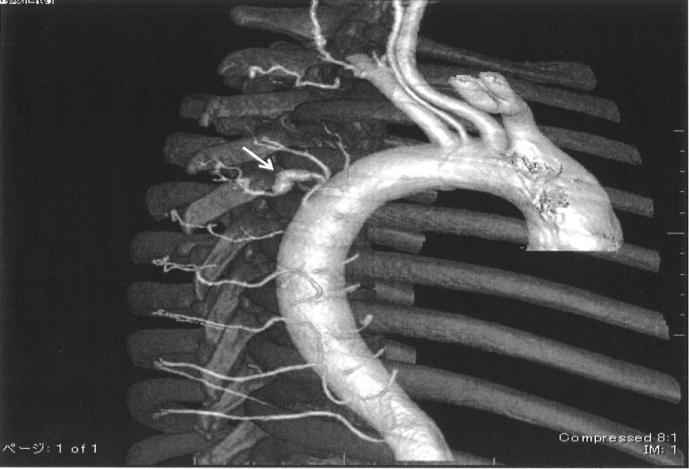
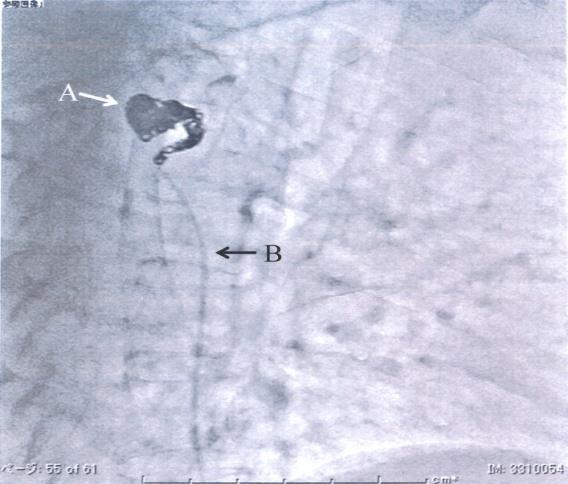
Patient consent was obtained. A 52-year-old man was transported by ambulance for reasons of general malaise. He had many café au lait spots on his skin. He was diagnosed as having NF1 by skin biopsy of a café au lait spot. Circulation and breathing were stable. The hemoglobin level was 16.9 g/dL. The hematocrit level was 46.4%. On the second day of hospitalization, he suddenly complained of chest pain and dyspnea. Contrast-enhanced computed tomography (CECT) revealed left massive pleural effusion, mediastinal right shift, left pulmonary passive atelectasis, and left fifth intercostal artery aneurysm (Figure 1). Three-dimensional computed tomographic angiography (3DCTA) revealed a saccular aneurysm at the left fifth intercostal artery (Figure 2). The size of the aneurysm was 8 mm × 4 mm × 3 mm. The pleural effusion did not have a contrast effect on imaging. The hemoglobin level was 9.1 g/dL, and hematocrit was 25.8%. He was in clinical shock. Left chest drainage was performed. Approximately 2800 mL of blood was removed from the left thorax, blood transfusion was performed. The discharge liquid was blood, but sustained bleeding did not occur after drainage. His circulation and respiration improved after these procedures. We concluded that the bleeding was controlled. We decided to perform embolization of the aneurysm. Using the Seldinger technique and the right femoral approach, a 6Fr introducer sheath (Radifocus Introducer II H, Terumo Corporation, Tokyo, Japan) and a 4.2Fr guiding catheter (Goodtec catheter GCB4-APR2, Goodman, Nagoya, Aichi, Japan) were inserted. A 1.7Fr microcatheter (Excelsior SL- 10, Stryker, Tokyo, Japan) over a microguidewire (Chikai AIN-CKI-200-RC, Asahi Intecc, Seto, Aichi, Japan) was advanced through the guiding catheter into the left fifth intercostal artery. We performed embolization of the aneurysm and the proximal artery with coils. We used seven coils (ED coil14 standard, Kaneka Medix, Osaka, Japan) as follows: two coils (8 mm-20 cm), two coils (5 mm-15 cm), two coils (4 mm-12 cm), and one coil (3 mm- 12 cm). Selective arteriography to the left fifth intercostal artery was performed after embolization. The aneurysmal cavity and the proximal portion of the aneurysm were filled with coils. There was no extravasation around the aneurysm and no blood flow to the distal artery (Figure 3). Re-rupture did not occur during the embolization procedure. The patient was discharge 16 days after embolization. At 19 months, there were no symptoms or signs of recurrence.
Discussion
Chest vascular lesions of NF1 patients may occur in the intercostal artery, subclavian artery, internal thoracic artery, vertebral artery, brachial artery, and thyrocervical artery. Aneurysm rupture, blood vessel tearing, or ruptures of the tumor vessel are the main causes of hemothorax in these patients. Because the blood vessel tissue is fragile in NF1, thoracotomy (open surgery or video-assisted thoracic surgery [3]) and a direct approach to diseased vessels are often difficult. Similarly, ablation of the bleeding area may not be tolerated. Endovascular treatment (EVT) techniques have improved recently [4, 5, 6]. Although EVT carries a risk of rupture, the risk of EVT is less than those of thoracotomy and ligation of fragile vessels. It is important to carefully advance the guidewire and avoid over-packing the aneurysm with coils. It was reported that liquid embolic agents, such as N-butyl-cyanoacrylate or gelatin, are better than solid coils [7]. Complications, such as paraplegia due to embolization of the Adamkiewicz artery, may occur [6]. We think that liquid embolic agents have a higher risk of embolism than coils, and may result in recanalization. When we performed coil embolization, to prevent the embolism of any vessel other than the target vessel, we used large coils at first and then small coils. There are many reports of successful coil embolization of intercostal artery aneurysms in NF1 patients [4, 5, 6], including our report, and we concluded that our strategy was technically feasible and effective. Because we had little clinical experience of NF1, we performed a biopsy for a definitive diagnosis of NF1. However, NF1 can be diagnosed by a simple physical examination and interview. In our case, the diagnosis of intercostal artery aneurysm, the decision of the position, the decision of the size, and the decision of the form were possible for clear imaging by 3DCTA before the operation. Furthermore, 3DCTA was useful for guidance to the target artery during EVT [8]. We should consider the possibility of aneurysm rupture when we encounter a spontaneous hemothorax in NF1.
Conflicts of Interest
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for- profit sectors.
Acknowledgements
We thank Muneo Hiromoto, RT, Kazuko Takemitsu, RN, and Mie Yamanaka, RN for their help with coil embolization. We thank Yuya Nakamura, RT for his help with 3D-CT angiography.
References
-
Brasfield RD, Gupta TKD (1972) Von Recklinghausen's disease: a clinicopathological study. Ann Surg 175(1): 86-104.
-
Leier CV, De Wan CJ, Anatasia LF (1972) Fatal hemorrhage as a complication of neurofibromatosis. Vasc Surg 6(2): 98-101.
-
Miyazaki T, Tsuchiya T, Tagawa T, Yamasaki N, Nagayasu T (2011) Spontaneous hemothorax associated with von Recklinghausen’s disease: report of a case. Annals of Thoracic and Cardiovascular Surgery 17(3): 301-303.
-
Dominguez J, Sancho C, Escalante E, Morera JR, Moya JA, et al. (2002) Percutaneous treatment of a ruptured intercostal aneurysm presenting as massive hemothorax in a patient with type I neurofibromatosis. J Thorac Cardiovasc Surg 124(6): 1230-1232.
-
Arai K, Sanada J, Kurozumi A, Watanabe T, Matsui O (2007) Spontaneous hemothorax in neurofibromatosis treated with percutaneous embolization. Cardiovasc Intervent Radiol 30(3): 477- 479.
-
Aizawa K, Iwashita C, Saito T, Misawa Y (2010) Spontaneous rupture of an intercostal artery in a patient with neurofibromatosis type 1. Interact Cardiovasc Thorac Surg 10(1): 128-130.
-
Keeling AN, Costello R, Lee MJ (2008) Rasmussen's aneurysm: a forgotten entity? Cardiovasc Intervent Radiol 31(1): 196-200.
-
Nakamoto K, Hashiyada H, Toshiyuki F, Takeshige M, Yoshida K, et al. (2015) Visualization of Vascular Anastomosis as Responsible Sites of Hemoptysis by Three-Dimensional Angiography for the Guidance of Endovascular Treatment. Int J Radiol Imaging Technol 1(1).
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage