Insidious Fournier Gangrene: When the Radiologist Shows the Way to the Surgeon
Fournier’s gangrene is a rare and fulminant necrotizing fasciitis of the urogenital and perineal areas, most of the time from a polymicrobial origin. This condition needs immediate surgical drainage as well as broad-spectrum antibiotics. We present here a patient with Fournier’s gangrene that required intensive care management. Then, we describe the role of medical imaging for the diagnosis and the staging of this life threatening disease.
Case Report
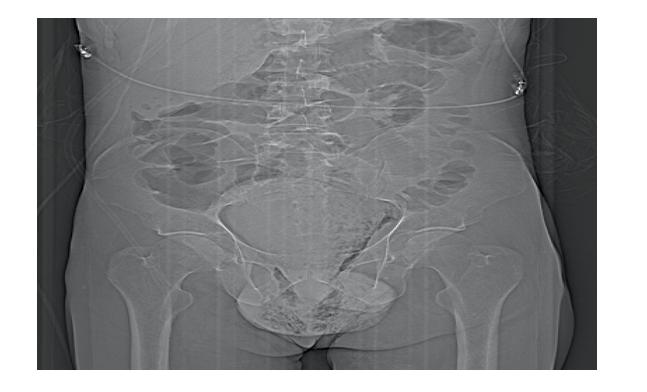
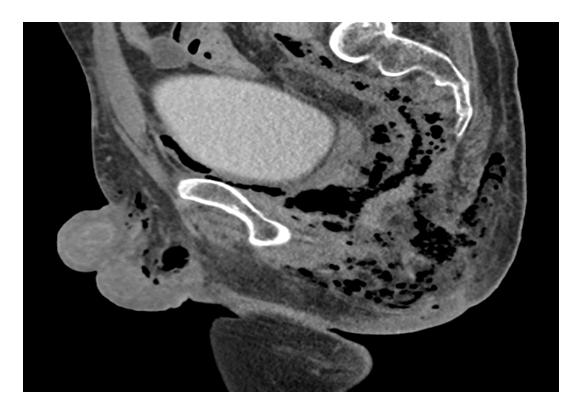
A 40-year-old man was addressed to the emergency department for acute dyspnea and fever. His vital parameters were altered including tachycardia, tachypnea and low blood pressure. Abdominal and cardiorespiratory examinations were of no interest. Laboratory tests showed hyperleukocytosis, altered ionogram, elevation of D-dimer, acidosis and rhabdomyolisis. Transthoracic echocardiography, urinary analysis and lower-limbs venous Doppler were all banal. Computed tomography pulmonary angiography was performed and confirmed bilateral sub-segmental pulmonary embolisms (not shown). The patient was therefore managed in the Intensive Care Unit. Due to the increase of the biological inflammatory markers and the discovery of an indurated collection in the perineal region with purulent discharge, a contrast-enhanced abdominal CT was required. Gas dissection of the peri-anal, scrotal and pre-sacral spaces led to the diagnosis of Fournier gangrene (Figures 1 & 2). There was a horseshoe-shaped perianal abscess (Figure Image Article
3). The management consisted in urgent surgical drainage and debridement of the collections, parenteral broad- spectrum antibiotherapy (microbiologic samples identified a Streptococcus anginosus) and supportive cares. The patient got out of the hospital after a month. Resorption of the collections was on the way to completion at abdominal CT performed 6 weeks later.

Discussion
Fournier gangrene is a rare surgical emergency. Nothing should delay the surgical management if the diagnosis is clinically proved. Progression of this necrotizing fasciitis is very fast (several centimeters per hour). As in this case report, imaging is essential to ascertain the diagnosis and to assess the anatomical extent.
Abdomen radiography can be useful to spot - often before clinical evidence - the presence of soft tissue gas in the perineal or the scrotal regions, which occur in 90% of the patient. It could also detect scrotal soft tissue swelling.
Ultrasonography can show an edematous and thickened scrotal wall containing hyperechoic foci that generate a “dirty shadowing” appearance. That is caused by the presence of gas in the scrotal wall. US is also able to confirm good testicular vascularization and to exclude other diagnosis like acute epididymitis, testicular torsion or inguino-scrotal strangulated hernia.
Abdominal CT is the more reliable and more specific imaging test in this pathology. Its features in Fournier’s gangrene include soft tissue and fascia thickening (mostly asymmetric), fat stranding, subcutaneous emphysema and delimitation of pus collections. Sometimes, CT may also be able to find an underlying cause to fasciitis (perianal abscess, colonic perforation, tubo-ovarian abscess…). There is a strong correlation between the extent of fascial thickening and fat stranding seen on CT and the involved tissue during surgery. CT is also used for follow-up of this condition.
Fournier gangrene is rare but associated with high mortality and morbidity rates and very fast progression. Radiologist should be aware of its modus operandi to precise the diagnosis, define the extension of the disease and call the surgeon without further delay.
Reference
1. Levenson RB, Singh AK, Novelline RA (2008) Fournier
Gangrene: Role of Imaging. Radiographics 28(2): 519- 528.
References
-
Levenson RB, Singh AK, Novelline RA (2008) Fournier Gangrene: Role of Imaging. Radiographics 28(2): 519- 528.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage