MRI Imaging of Spinal Intramedullary Tuberculoma
Spinal cord tuberculoma is a rare entity with cerebral to cord ratio 42:1, and is induced by haematogenous dissemination or through CSF infection. It is a treatable entity so holds importance in diagnosis. We present a case of a 21 year old male presented with weakness, numbness and paresthesias in bilateral upper limbs with characteristic MR imaging findings of tuberculoma in the cord in healing calcified granulomatous stage.
Case Report
A 21 year old male presented with weakness, numbness and paresthesias in bilateral upper limbs 1 year back, Diagnosis was established as spinal cord tuberculoma in inflammatory stage then by imaging and CSF biochemical analysis at PGI Chandigarh. Now patient came to our institute for follow up MRI scan. MRI scan which sows well defined lesion in cervicomedullay junction with heterogeneous signal intensity with peripheral hypointense rim of calcification seen and there is subtle post gadolinium enhancement in Saggital T2W, STIR, T1W and POST CONTRAST Images (Figures 1A-C & 1F) axial T2W (Figure 1D) Coronal STIR and POST CONTRAST (Figures 1E, 1F) (Lesion is indicated by arrows). Healing Calcified granular stage of tuberculoma was given as diagnosis.
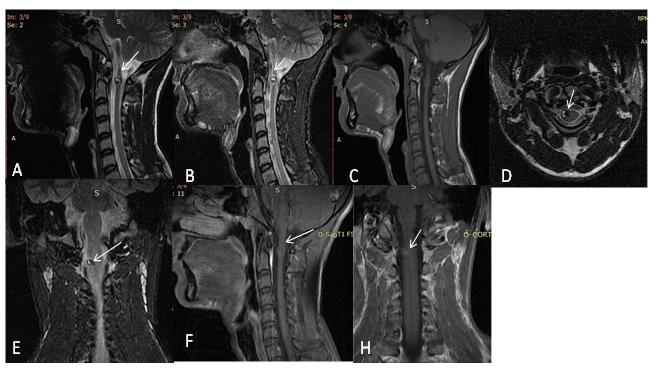
Figures 1(A-H): Patient is a diagnosed case of spinal cord tuberculoma came for follow up MRI scan which sows well defined lesion in cervicomedullay junction with heterogeneous signal intensity with peripheral hypointense rim of calcification seen and there is subtle post gadolinium enhancement in Saggital T2W, STIR, T1W and POST CONTRAST Images (A-C, F) axial T2W (D) Coronal STIR and POST CONTRAST (E, F) (Lesion is indicated by arrows). Healing Calcified granular stage of tuberculoma was given as diagnosis.
Discussion
Spinal cord tuberculoma is a rare entity with cerebral to cord ratio 42:1, and is induced by haematogenous dissemination or through CSF infection. It is a treatable entity [1, 2]. Mycobacterium tuberculosis can involve the neural and perineural tissues may occur anywhere within the CNS. Tuberculomas may be intradural extramedullary, intramedullary or extradural [4].
Clinical Presentation
Patient usually presents with pain in the back, numbness, paresthesias and muscular atrophy [3, 5]. Key Imaging Diagnostic Clues: Depends on the stage of tuberculoma [1, 2, 4, 6]. a) Early stage shows infective reactions, cord oedema and poor capsule formation, there is enhancement post- contrast.
b) Late stage shows capsule formation, reduced oedema and may show target sign on T2W images, rim or nodular calcification may also be seen.
Parsons and Pallis in their study in 1965 divided IDEM Tuberculomas into 2 groups. The first group comprises hard round lesions, which are 2 to 3cm in diameter having thin capsule and calcification. The second group there is diffuse avascular grayish tuberculous granulation tissue encasing the cord. Our patient belongs to the second group.
Conclusion
Spinal cord tuberculoma like TB elsewhere in the body is treatable so clinical suspicion and Imaging diagnoses hold utmost importance. MR imaging is useful technique in the diagnoses of it but features vary with the stage of the disease [4].
References
-
Lu M (2010) Imaging diagnosis of spinal intramedullary tuberculoma: case reports and literature review. J Spinal Cord Med 33(2): 159-162.
-
Ramdurg SR, Gupta DK, Suri A, Sharma BS, Mahapatra AK (2009) Spinal intramedullary tuberculosis: a series of 15 cases. Clin Neurol Neurosurg 111(2): 115-118.
-
Sharma MC, Arora R, Deol PS, Mahapatra AK, Sinha AK, et al. (2002) Intramedullary tuberculoma of the spinal cord: a series of 10 cases. Clin Neurol Neurosurg 104(4): 279-284.
-
Chang KH, Han MH, Roh JK, Kim IO, Han MC, et al. (1990) Gd-DTPA enhanced MR imaging in intracranial tuberculosis. Neuroradiology 32(1): 19- 25.
-
Nussbaum ES, Rockswold GL, Bergman TA, Erickson DL, Seljeskog EL (1995) Spinal tuberculosis: a diagnostic and management challenge. J Neurosurg 83(2): 243-247.
-
Gupta VK, Sharma BS, Khosla VK (1995) Intramedullary tuberculoma: report of two cases with MRI findings. Surg Neurol 44(3): 241-243.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage