The Ground Glass of the Pulmonary-Kidney Syndrome Case Report
The pulmonary-Kidney syndrome encompasses genetic and autoimmune diseases that involve tissue structures of the same origin. Radiological findings are usually found with alveolar opacities and ground glass. We present a related clinical case and the diagnostic approach of the most frequent differential diagnoses of these findings.
Introduction
The diseases that affect the lung and the kidney at the same time can be of genetic or autoimmune origin. The pulmonary-kidney syndrome was initially associated with the pathologist Ernest Goodpasture in 1919, due to his findings in autopsies in the epidemic influenza [1]. Taking into account that the etiological diagnosis is vasculitis, an annual incidence of 20 / million inhabitants is estimated [2]. Within the autoimmune spectrum, it is important to know epidemiologically which are the most frequent and which imaging spectrum they develop, in order to have an etiological approach from the diagnostic images of the thorax [3, 4]. We presented a case of a patient with pulmonary-kidney syndrome due to vasculitis and the imaging approach of this diagnostic challenge.
Clinical Case
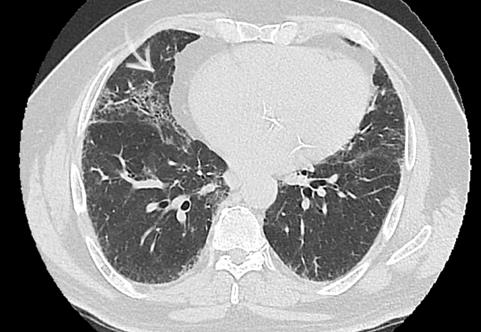
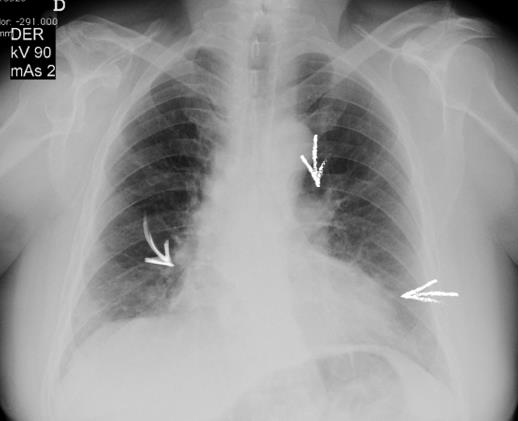
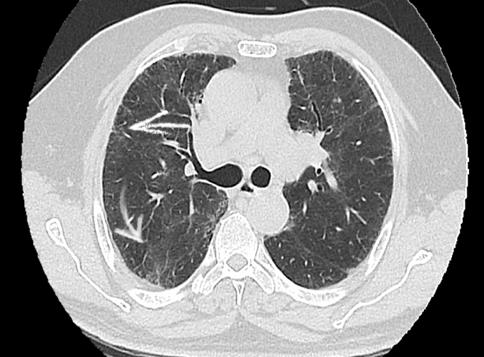
A 66-year-old patient diagnosed with controlled hypertension without renal disease who presented a 5- month course consisting of impairment of his functional class from I / V to III / V with dyspnea as the main symptom. Dyspnea is exacerbated during the last 15 days with dry cough without expectoration, so consult the emergency department. At admission, the patient had a laboratory test of interest: hemoglobin without alterations with leukocytosis without neutrophilia, the uroanalysis presented incipient proteinuria. Creatinine values of 1.58 without alterations in nitrogen. The patient was taken to the radiology department where a chest x- ray and a high-resolution tomography (Figures 1-4). The patient presented clinical deterioration with sudden renal alteration despite medical management. Within a few days, it was determined that the patient had positive anti myeloperoxidase by indirect immunofluorescence compatible with microscopic polyangiitis. He is given medical treatment with clinical improvement and early hospital discharge.

Discussion
The kidneys and lungs share special diseases due to their high perfusion and similarity in the structure of the basement membrane and microtubules [3]. The distribution of kidney or lung disease depends on each etiology. It is very important to know the clinical progression, the distribution of the age group in terms of the social and demographic variables, the comorbidities that worsen the clinical picture and the chronological imaging findings (Table 1). The radiological approach in radiography and tomography is very difficult because most of the findings focus on alveolar and ground glass opacities as in the case of our patient. Therefore, it is always essential to know as a radiologist the clinical history and the reduced spectrum of autoimmune diseases that can develop this lung-kidney syndrome. In the case of the patient, the nonspecific findings were tomographically reported and on the other hand his renal injury progressed without apparent cause. Epidemiologically, the most frequent etiology in these cases of kidney lung syndrome is microscopic polyangiitis, as it was in our patient [4]. However, the radiologist must be more analytical and evaluate the associated findings, as in the case of Goodpasture syndrome, which is the main differential diagnosis [5]. However, it occurs more in young people and smokers [3, 4].
Granulomatosis with polyangiitis, presents with additional deterioration of the upper airway (90%), subglottic stenosis and nodules or lung masses of peripheral distribution. Eosinophilic Granulomatosis with Polyangiitis presents with peripheral neuropathy, in young patients, and with asthma up to 90% [6]. Systemic lupus erythematosus (SLE) is more common in women and presents pleuritis and pulmonary embolism up to 50%
[7], unlike IgG4-Related Sclerosing Disease, where pancreatic abnormality is characteristic. Systemic sclerosis presents with dermatological alterations [8], the Erdheim-Chester Disease with metaphyseal cortical alterations of the legs, while the sarcoidosis debuts with nephrocalcinosis and a characteristic pattern in the tomography without ground glass generally (Table 1).
pulmonary-kidney involvement. It is important to always look for the clinical context of the patient and always ask if there is renal involvement at the time of assessing the finding of ground glass. Frequently the clinician looks for the radiologist to ask about the relevance of this finding in the tomography. It is important that the radiologist evaluate the post-test probability of the findings of the ground-glass opacities, which increases in the context of a patient with acute renal impairment directing a diagnostic approach to pulmonary-kidney syndrome.
The clinical relevance of ground glass in this type of patient speaks of the progression of the disease with dual Social and demographic distribution / Comorbidities Syndrome Clinical progression Rapidly progressive glomerulonephritis Goodpasture Young / Smoker
40-60%. Alveolar
hemorrhage
40-65 years old / Granulomatosis
Upper airway deterioration 90%. Glomerulonephritis
Treatment with corticosteroids, proteinuria> 1g /
with polyangiitis (before wegener)
85%.
day. Previous kidney injury.
Eosinophilic Granulomatosis
Peripheral neuropathy 75%, glomerulonephritis
3rd decade of life 90% / Asthma 90%.
with Polyangiitis (before churg
Eosinophilia
25%.
strauss) Arthritis, rash, gloerulonephritis (50%), pleuritis and Systemic lupus erythematosus Women / Immunosuppression (SLE) pericarditis.
Scleroderma, Thickening of the skin Interstitial lung
50% have renal impairment but Systemic sclerosis renal failure is disease 75%.
incomun Pulmonary hypertension 50%.
Autoimmune
pancreatitis (>patients), renal injury 35%, biliary IgG4-Related
67 yeras old (25- 93). Inflammatory
Sclerosing
disorder 77%, lymph nodes 33%, Disease
bowel disease.
retroperitoneum and mediastinum.
Imaging findings Physiopathology
Rx: Solitary, multifocal or diffuse alveolar opacities. CT:
Glomerular
basement menbrane antibodies (GBM) ground glass, thickening of interlobular septa, consolidation Nodules or lung masses, generally peripheral, ground glass, nodules cavitated in 50%, Antineutrophil cytoplasmatic antibodies ( c- subglottic stenosis, and alteration of the posterior membrane of the trachea.
ANCA)
Ground glass, consolidative airspace opacities, pulmonary Antineutrophil
cytoplasmatic antibodies (c- nodules, interlobular septal thickening.
ANCA)
Pleuritis 50%. Pulmonary
ANA or anti-
embolism, opportunistic dsDNA pneumonia.
Non-specific interstitial pneumonia (NINE). Peripheral
Deposits of collagen in soft
and peribronchovascular fibrosis. Ground glass, traction tissues and vasculature [9].
bronchiectasias.
Pancreatic thickening and hypoenhancemen, pulmonary alterations 13%: peribronchial inflammation, discrete nodules, Infiltration of plasma cells and reticulation or septal thickening, or consolidation. Renal involvement is common positive T lymphocytes for igG4. IgG4 levels and involves the cortex. The most common appearance is elevated 86%.
discrete nodules or wedge- shaped lesions that are T2
hypointense and
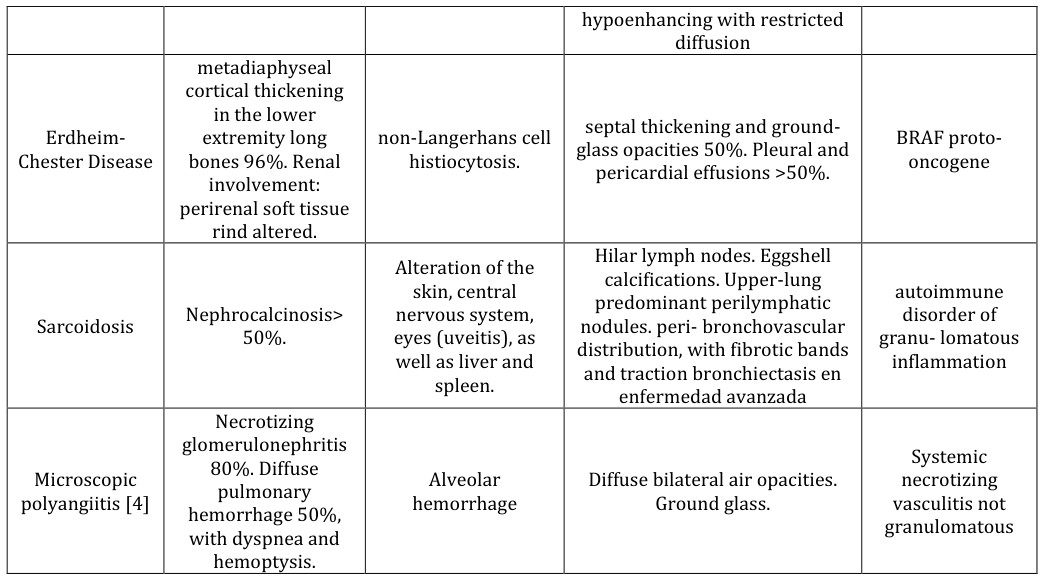
- hypoenhancing with restricted diffusion metadiaphyseal cortical thickening in the lower extremity long bones 96%. Renal septal thickening and groundglass opacities 50%. Pleural and
- Erdheim-
- Chester Disease non-Langerhans cell histiocytosis. pericardial effusions >50%. involvement: perirenal soft tissue rind altered.
- Hilar lymph nodes. Eggshell
- Alteration of the calcifications. Upper-lung predominant perilymphatic nodules. peri- bronchovascular distribution, with fibrotic bands skin, central nervous system, eyes (uveitis), as
- Sarcoidosis
- Nephrocalcinosis>
- 50%. well as liver and and traction bronchiectasis en spleen. enfermedad avanzada
- Necrotizing glomerulonephritis
- 80%. Diffuse
- Microscopic polyangiitis [4]
- Alveolar hemorrhage
- Diffuse bilateral air opacities. pulmonary hemorrhage 50%, with dyspnea and
- Ground glass. hemoptysis.
Table 1: Distribution of autoimmune diseases that present lung-kidney disorders [3].
Vasculitis of small vessels is the main cause of the alteration of the kidney and the lung in this type of patients, where at least twenty different varieties are described. The most important manifestation is the renal alteration that may be incipient, associated with pulmonary manifestations, where up to 50% of the cases do not present alterations in the chest X-ray. When radiographic alterations occur, images of alveolar occupation without alteration of diaphragmatic cost angles are evident [2]. In spite of this, in the high- resolution tomography, the pattern in ground glass without interlobulillar thickening, which can guide the diagnosis with diffuse alveolar hemorrhage, is acutely evidenced that associated with the renal alteration is highly suggestive of a pulmonary-kidney syndrome caused by Vasculitis. Microscopic polyangiitis presents with segmental focal glomerulonephritis in addition to the imaging findings already described [10]. As a final recommendation it can be described that whenever we are confronted with this non-specific finding in tomography with important clinical deterioration of the patient, we must ask ourselves and follow up the renal function to be able to evaluate if it is a pulmonary kidney syndrome in the context of these vasculitis.
2. Bruselle GG (2007) Pulmonary-renal syndromes. Acta
Clin Belg 62(2): 88-96.
3. Hammer MM, Shetty AS, Sheybani EF, Bhalla S (2017)
Diseases and Syndromes That Affect the Lungs and the Kidneys: A Radiologic Review. Curr Probl Diagn Radiol 46(3): 216-224.
4. Feragalli B, Mantini C, Sperandeo M, Galluzzo M,
Belcaro G, et al. (2016) The lung in systemic vasculitis: radiological patterns and differential diagnosis. Br J Radiol 89(1061): 20150992.
5. Mohammad AJ, Mortensen KH, Babar J, Smith R, Jones
RB, et al. (2017) Pulmonary Involvement in Antineutrophil Cytoplasmic Antibodies (ANCA)- associated Vasculitis: The Influence of ANCA Subtype. J Rheumatol 44(10): 1458-1467.
6. Flores-Suárez LF, Alba MA, Mateos-Toledo H, Ruiz N
(2017) Pulmonary Involvement in Systemic Vasculitis. Curr Rheumatol Rep 19(9): 56.
7. Lichtenberger JP, Digumarthy SR, Abbott GF, Shepard
JA, Sharma A (2014) Diffuse pulmonary hemorrhage: clues to the diagnosis. Curr Probl Diagn Radiol 43(3): 128-139.
8. Castañer E, Alguersuari A, Gallardo X, Andreu M,
Pallardó Y, et al. (2010) When to suspect pulmonary vasculitis: radiologic and clinical clues. Radiographics 30(1): 33-53.
9. Colby TV, Fukuoka J, Ewaskow SP, Helmers R, Leslie
KO (2001) Pathologic approach to pulmonary hemorrhage. Ann Diagn Pathol 5(5): 309-319.
10. Hié M, Costedoat-Chalumeau N, Saadoun D, Azoulay E
(2013) [The pulmonary-renal syndrome: a diagnostic and therapeutic emergency for the internist and the intensivist]. Rev Med Interne 34(11): 679-686.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage