A Rare Case of Coronary Artery Fistula on Vieussens Arterial Ring
Coronary artery fistulas represent an abnormal communication between coronary circulation and heart chambers or any segment of pulmonary or systemic circulation, without an intervening capillary network. Seldom, this connection can arise on a conotruncal anastomotic variant linking the anterior descending artery and the right coronary artery or a conus artery originating from the right coronary sinus, known as Vieussens’ arterial ring. Here we discuss a case of a 73-yearold man undergoing a coronary CT angiography because of recurrent chest pain and cardiovascular risk factors; the exam showed multiple aneurismatic sacs on a Vieussens arterial ring, associated with a fistulous connection between one of the aneurysms and the main pulmonary artery, highlighted by an hyper dense jet of contrast medium within its lumen. We spotted also enlarged right and left pulmonary arteries and right ventricular dilatation, with a mild hemodynamic overload on echocardiographic evaluation. A coronary angiography confirmed the findings shown by CT scan. After a multidisciplinary discussion, the interventional cardiology team decided to close the fistulous connection. Therefore, in a subsequent procedure the malformation was treated by catheterizing the branch stemming from the anterior descending artery and placing embolization coils in the first aneurysmatic sac and in the vessel itself; the same treatment was performed on the branch originating from the right coronary sinus. Final angiographic control showed complete exclusion of the saccular aneurysms from the circulation and closure of the associated fistula. There was no peri or post-procedural complication.
Introduction
Coronary artery fistulas represent an abnormal communication between coronary circulation and heart chambers or any segment of pulmonary or systemic circulation, without an intervening capillary network. Such anomaly was first reported in 1865 by Krauseand accounts for 0.2-0.4% of congenital heart diseases; in fact, about 90% of coronary fistulas derives from congenital disorders due to lack of regression of fetal cardiovascular connections [1, 2]. Seldom, they may be caused by coronary stenting, by-pass procedures or thoracic radiotherapy; rare vasculitis-related cases have been reported, as well as fistulas occurring in late phase of myocardial infarction.
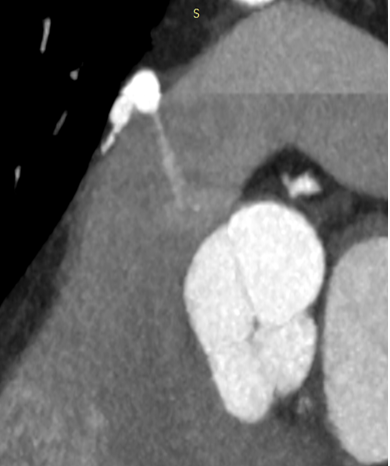
Right coronary artery is involved in roughly 50% of cases, while left coronary artery is affected in 42% and both vessels supply the fistula in 5% of cases; 90% of these anomalies drain into a low-pressure compartment, such as right chambers, superior vena cava, coronary sinus, pulmonary artery or left atrium [3]. Here we report a rare case of a coronary artery fistula between a conotruncal anastomotic variant, the Vieussens ring, and main pulmonary artery (Figure 1,2).

Case Report
A 73-year-old male patient was referred to our Centre by his cardiologist to undergo a coronary-CTA because of recurrent chest pain and dyspnea occurred in the last 6 months, both at rest and on exertion, lasting from a few minutes to 2 hours. The patient was diabetic, hypertensive and current smoker and had a 4-cm abdominal aortic aneurysm which was kept under surveillance with scheduled US and CTA examinations; he was also affected by benign prostatic hyperplasia associated with bladder wall hypertrophy and had once undergone a head CT demonstrating lacunar infarcts in keeping with chronic vasculopathy.
Ergometric test and echocardiography had not been performed, and his ECG tracing was normal. Coronary CTA was carried out with a last-generation scanner providing Z-axis coverage of 16 cm, allowing an axial “single beat” acquisition, from 40% to 80% of cardiac cycle, after administering sublingual trinitrine and 50 ml of Iomeprol 400 IV with a 5 ml/sec injection rate. Both coronary arteries displayed regular origin and course, with multiple partially-calcified, eccentric atherosclerotic plaques, which did not cause any significant stenosis. We detected a large vessel arising from the right coronary sinus, above the right coronary arteries ostium, which coursed anteriorly to the main pulmonary artery and fed a large, winding vascular malformation with many aneurysmal pouches, the largest of 11-mm diameter; the malformation was in communication with the supravalvular pulmonary artery, which had an intraluminal hyper dense jet of contrast medium. The anomalous vascular net continued then in a collateral vessel originating from the proximal anterior descending artery. We spotted also enlargement of right and left pulmonary arteries and moderate right ventricular dilatation (Figure 3).
The findings were in keeping with a conotruncal anastomotic Vieussens ring associated with a systemic- to-pulmonary shunting. After discussing the case with interventional cardiologists in the multidisciplinary team, the patient was advised to undergo an echocardiography to evaluate right heart overload and a coronary angiography. The echocardiogram showed concentric remodeling of the left ventricle, with no segmental wall motion anomalies and a preserved ejection fraction (60%); the right ventricle was minimally enlarged, with normal-sized atria and a mildly increased pulmonary artery pressure (27 mmHg). Coronary angiography confirmed the presence of non- hemodynamically significant stenosis and a large vascular malformation, with multiple saccular aneurysms, fed by a branch of the anterior descending artery and associated with a jet of contrast medium towards the pulmonary artery lumen. Selective catheterization of the vessel branching from right coronary sinus showed by CTA displayed further aneurysmatic pouches (Figure 4-6).

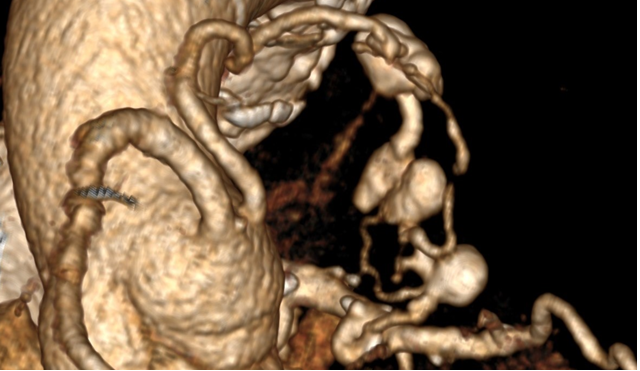
Figures 4-6: CTA volume rendering showing the complex course of the malformation, forming an incomplete ring anteriorly to the main pulmonary artery and connecting the right coronary sinus with the proximal segment of the anterior descending artery; these findings are in keeping with a conotruncal anastomosis known as Vieussens’ arterial ring.
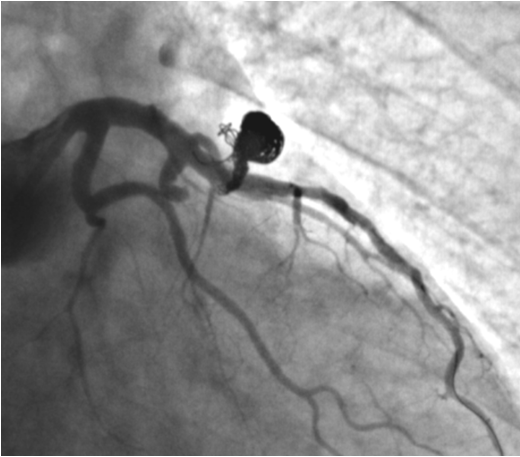
In a subsequent procedure a few days later the malformation was treated by catheterizing the branch stemming from the anterior descending artery and placing embolization coils in the first aneurysmatic sac and in the vessel itself; the same treatment was performed on the branch originating from the right coronary sinus. Final angiographic control showed complete closure of Vieussens arterial ring and the associated fistula, and the saccular aneurysms were properly excluded from circulation.
There was no peri or post-procedural complication (Figures 7 & 8).
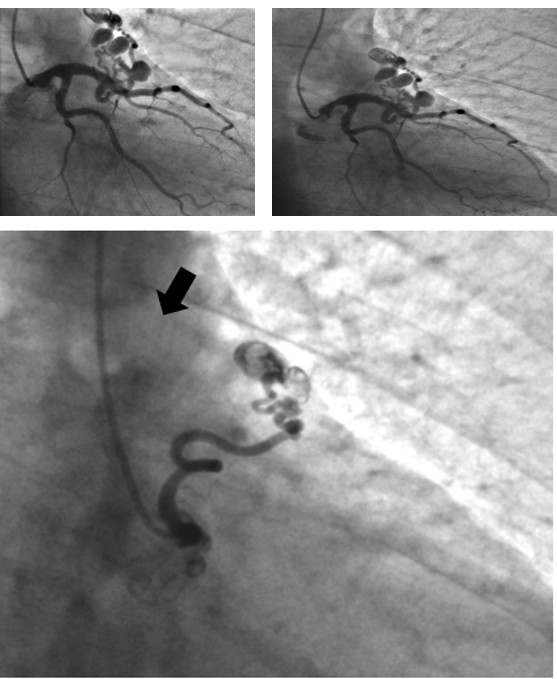
Figures 7-8: Coronary angiography with catheterization of main left coronary artery depicting part of the anastomotic ring; note the jet of contrast medium arising from one of the aneurysms (blue arrow), confirming the abnormal connection with main pulmonary artery. Although the remaining part of the malformation arising from right coronary sinus could not be opacified, note that the most distal aneurysmatic pouch is not entirely filled with contrast and seems to be “washed” by non- opacified blood (black arrow).
Discussion
The pulmonary conus artery is the first artery that originates from the right coronary artery (RCA); in 30-50% of cases this artery can originate in an independent ostium in the right sinus of Valsalva located anterior and superior to the ostium of the RCA. The conus artery irrigates the pulmonary infundibulum and the supraventricular crest but sometimes this artery runs on the left and forms an anastomosis with a branch of the left anterior descending artery (LAD) producing the so-called “arterial circle of Vieussens” or “Vieussens’ arterial ring” (VAR) [2, 3] (Figure 9).
Although in anatomical studies the prevalence of VAR in general population seems to be 48%, the detection rate by imaging methods is low (approximately 3.19%) [3].
According to Dogan et al.3 the Vieussens’ arterial ring can be classified in some variants as summarized in Table 1.
| Type | Explanation |
|---|---|
| 1A | VAR with no accompanying pathology |
| 1B | VAR with accompanying vascular pathology (aneurysm, fistula) |
| 2 | VAR-like dual LAD duplication |
| 3 | VAR with single coronary artery anomaly |
LAD: left anterior descendent; VAR: Vieussens arterial ring Table I: Classification of VAR variants.
The coronary artery fistulas (CAFs) are abnormal vascular communication between a coronary artery and the lumen of a cardiac chamber, the coronary sinus or superior vena cava, or a pulmonary artery or pulmonary vein close to the heart. More than 90% of CAFs are congenital; according to Hackensellner’s involution-persistence hypothesis, among the six branches of the truncus, only two branches persist and form the coronary arteries, and all the others degenerate. When the branch that should degenerate in the pulmonary sinus continues and connects to the branch from the aortic sinus, a fistula is formed. Only 10% of CAFs are acquired and they usually result from iatrogenic events such as coronary stent placement, coronary bypass surgery, trauma and chest irradiation [4, 5] (Figure 10).
Most adult patients are asymptomatic; the clinical manifestations depend on the severity of the left-to- right shunt1 and usually are dyspnea, orthopnea, angina, endocarditis, arrhythmias, stroke and myocardial ischemia.
Potential complications in large left-to-right shunts are pulmonary hypertension, congestive heart failure, rupture or thrombosis of the fistula or associated arterial aneurysm [6]. The selective invasive coronary angiography is the reference standard for CAFs evaluation, enabling the therapeutic embolization of the fistula; however, it is invasive, and it could be difficult to well-visualize the drainage site at conventional angiography when a CAF drain into low-pressure chambers of the heart because of significant dilution of the contrast medium.
The CT angiography has high temporal and spatial resolution and yields excellent anatomic information, enabling the correct treatment planning. A scan range that covers the aortic arch level beyond the carina is recommended because most of the drainage sites are located above the carina level. Other imaging modalities useful in the evaluation of CAFs and consequent hemodynamic changes are transthoracic or transesophageal echocardiography, whose main limitation is the operator dependency, and the MR angiography that nevertheless has lower spatial resolution and long acquisition time [2]. CAFs can be classified according to their etiology, origin, drainage site, complexity, the number of fistulous tracts and the presence of accompanying anomalies, as summarized in Table 2.
| Classification | Description |
|---|---|
| Based on CAF etiology | Congenital |
| Acquired: iatrogenic, disease-related (AMI, cardiomyopathy, Kawasaki disease, tumor), trauma-related, radiation injury | |
| Based on CAF origin | RCA |
| LCA: LAD and its branches, LCX and its branches, ramus intermedius | |
| RCA and LCA | |
| Based on drainage site | Coronary cameral fistula |
| Coronary arteriovenous fistula | |
| Based on number of fistulous tracts | Single or multiple |
| Based on CAF morphology and complexity | Simple CAF: has a single origin and drains through a single vascular course |
| Complex CAF: involves entangled blood vessels with multiple fistulous structures | |
| Based on presence of accompanying anomaly | Isolated CAF |
| CAF accompanied by ventricular septa defect, patent ductus arteriosus, tetralogy of Fallot |
Table 2: CAF classifications based on Various Factors.
The management of CAF is controversial. The antiplatelet therapy and the prophylactic precautions against bacterial endocarditis are recommended. The choose of management strategy, that include surgical ligation and percutaneous trans catheter closure of the fistula, depends on the size of the fistula, presence of symptoms, coronary arteries’ anatomy, patient’s age and presence of associated cardiovascular abnormalities. The main indications for percutaneous trans catheter closure of the fistula are the proximal location of the fistulous tract, single drain site, termination of the fistula away from the normal coronary arteries and older patient age [1, 2].
The indications for surgical ligation include large CAF characterized by high fistula flow, multiple communications or terminations, very tortuous pathways, significant aneurysmal formation, need for simultaneous distal bypass, or presence of large vascular branches that can be accidentally embolized [7, 8].
In our case, the patient was diagnosed with a conotruncal VAR anastomosis IB type with multiple aneurysms along the course and a single fistulous tract draining in the pulmonary artery. It was treated by performing a percutaneous transcatheter closure of the fistula.
Conclusion
The VAR-like conotruncal anastomoses are rare variants of the coronary circulation that can be associated with aneurysms and fistulas along their course. The CT angiography enables the morphological evaluation of coronary arteries and the appropriate diagnostic-therapeutic care pathway, while the selective invasive coronary angiography is the reference standard for the accurate evaluation of anatomy and flow dynamic within the vessel, enabling the closure of the fistulous tract. It is essential to make an in-depth study of coronary artery morphology and a multidisciplinary clinical and anamnestic evaluation of the patient, in order to choose whether to treat the malformation and which treatment is appropriate for the patient.
References
-
Krause W (1865) Uber den ursprung einer accessorischen a. coronaria aus der a. pulmonalis. Z Ratl Med 24:225-227.
-
Yun G, Nam TH, Chun EJ (2018) Coronary Artery Fistulas: Pathophysiology, Imaging Findings, and Management. Radio Graphics 38(3): 688-703.
-
Zenooz NA, Habibi R, Mammen L, Finn JP, Gilkeson RC (2009) Coronary artery fistulas: CT findings. RadioGraphics 29(3): 781-789.
-
Dogan N, Dursun A, Ozkan H (2019) Vieussens’ arterial ring: a rare coronary variant anatomy. Diagn Interv Radiol 25(2): 109-113.
-
Ade Augustin J, Marcos-Alberca P, Hernandez- Antolin R, Vilacosta I, Perez de Isla L, et al. Collateral circulation from the conus coronary artery to the anterior descending coronary artery: assessment using multislice coronary computed tomography. Rev Esp Cardiol 63(3): 347-351.
-
Kim MS, Jung JI, Chun HJ (2010) Coronary to pulmonary artery fistula: morphologic features at multidetector CT. Int J Cardiovasc Imaging 26(Suppl 2): 273-280.
-
Gowda RM, Vasavada BC, Khan IA (2006) Coronary artery fistulas: clinical and therapeutic considerations. International Journal of Cardiology 107(1): 7-10.
-
Said SAM, van der Werf T (2006) Dutch survey of coronary artery fistulas in adults: congenital solitary fistulas. Int J Cardiol 106(3): 323-332.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage