Spontaneous Achilles tendon Rupture in Calcaneus Osteomyelitis
Background: Achilles tendon is the most common injured tendon in the lower limb. Spontaneous rupture is attributed to some intrinsic and extrinsic factors in which medications side effect (e.g. corticosteroids and quinolones) is the most common reported cause in the literature. Case presentation: we present a case of 76-year-old female known case of uncontrolled type II diabetes and hypertrophic right Charcot foot. She was diagnosed with chronic foot osteomyelitis for which she received long course of ceftriaxone. Six month following completing the antibiotic course, she presented with fever and malaise with decreased right foot range of motion in the absence of traumatic event. Upon requesting multiple imaging modalities, she was diagnosed with acute Achilles tendon rupture in the setting of acute on top of chronic calcaneus osteomyelitis. Conclusion: AT rupture in the setting of osteomyelitis is a rare entity and has not been reported previously in the literature. This case will bring the attention in evaluating the tendons thoroughly in cases of osteomyelitis.
Introduction
Achilles tendon (AT) is the thickest and strongest tendon in the body that contributes to knee flexion, foot plantar flexion, and hind-foot inversion [1]. It is formed by the confluence of gastrocnemius and soleus tendons where they converge into the AT approximately 5 to 6 cm from its insertion at the calcaneal tuberosity [2]. The tendon rotates 90 degrees around a vertical axis, generating an effective elastic recoil that allows it to withstand forces up to 12 times body weight. Although this is energy efficient, it also creates stress riser 2 to 5 cm proximal to its distal insertion. This area of the tendon coincides with the vascular watershed, which is compromised in 75% of AT ruptures [3].
AT rupture accounts for 20% of all large tendon ruptures and is the most common tendon injured in the lower limb [1, 2]. Spontaneous rupture of AT is rare and has been reported in patients on quinolone therapy and in patients receiving long-term steroid therapy for autoimmune diseases; such as rheumatoid arteritis and systemic lupus erythematous [4]. To the best of our knowledge, concomitant spontaneous AT rupture in the setting of osteomyelitis haven’t been reported previously.
A 76-year-old female known case of uncontrolled type II diabetes mellitus, stage IVa chronic kidney disease and chronic hypertrophic right Charcot foot following up routinely in podiatrist clinic. She complains of limited mobilization with decreased sensation in the feet. She is known to have chronic right foot osteomyelitis for which she received and completed a long course of ceftriaxone. Six months later, she presented to the emergency department with 5 days history of fever and malaise with no foot pain. She has limited range of motion of the right foot, which has worsened in the past 3 days. No traumatic event was reported.
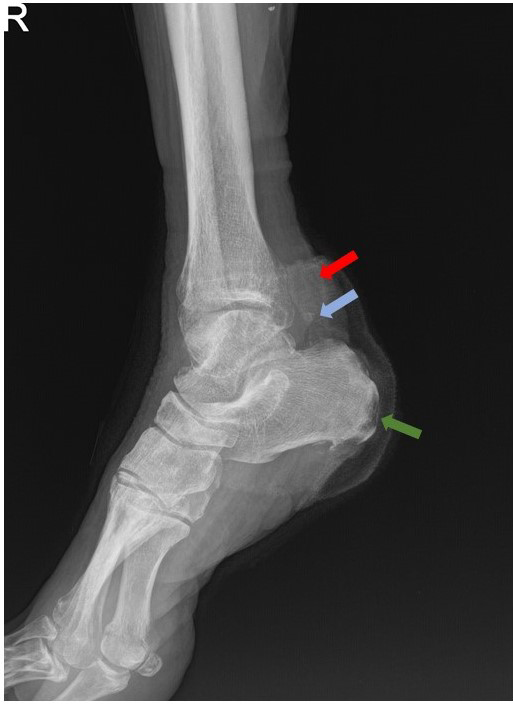
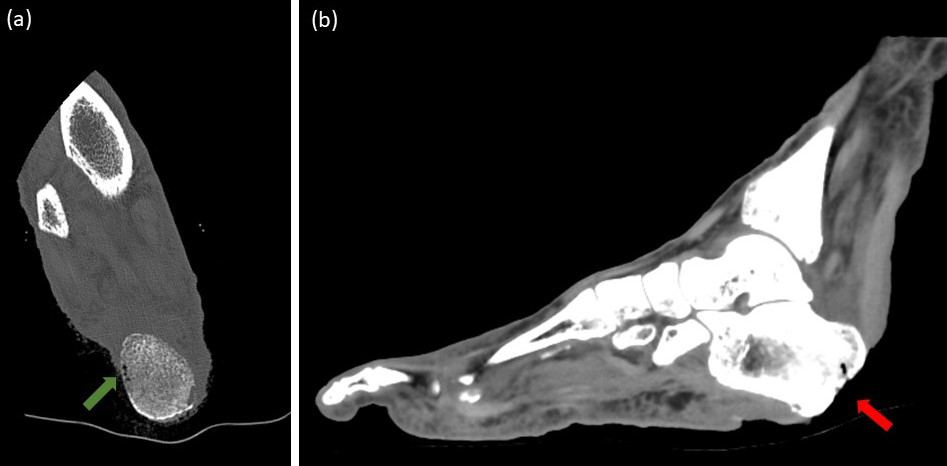
Right foot radiograph was requested and showed no fracture or acute findings (Figure 1). CT scan of the right foot was done on the same day to look for subtle fractures and showed focal area of gas in the calcaneus concerning for osteonecrosis (Figure 2).
The patient was admitted to the ward and MRI of the right foot was requested and showed acute on top of chronic calcaneus osteomyelitis with acute AT rupture (Figure 3). The patient was opted for below knee amputation due to recurrent episodes of osteomyelitis that resulted in osteonecrosis. Post-operative radiograph is shown (Figure 4).
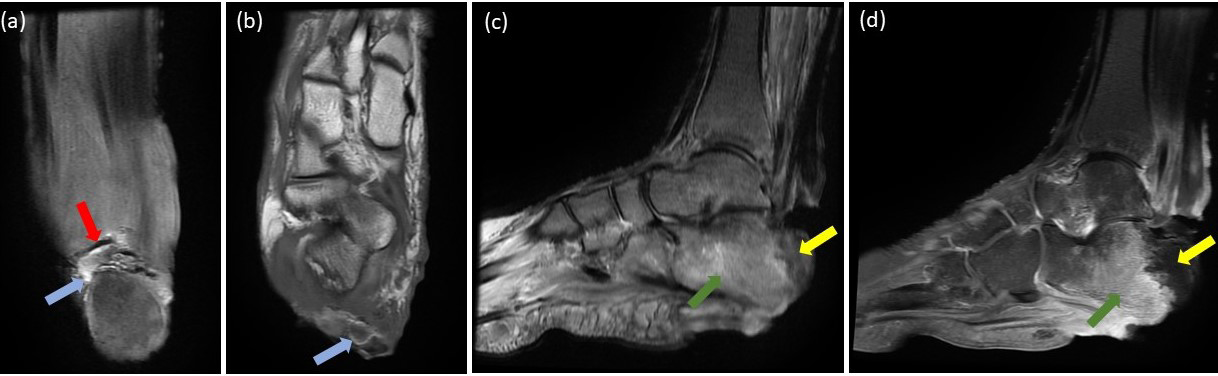
Figure 3: MRI of the right ankle. Coronal T1 fat saturation (a) and axial T1 (b) images demonstrate AT fibers disruption (red arrow) with intervening high signal intensity (blue arrow); representing AT tear with acute hematoma. Sagittal STIR (c) and T1 post contrast (d) images demonstrate bone marrow edema in the posterior calcaneal process (green arrow). The posterior calcaneal tuberosity show low STIR signal intensity with no enhancement in T1 post contrast image; representing osteonecrosis (yellow arrow).

Discussion
In view of widespread presentation of osteomyelitis in clinical practice, this novel case presentation has important implications. The occurrence of spontaneous AT rupture in acute on top of chronic osteomyelitis expands the understanding of its etiology which was previously reported only with long-term steroid and quinolone therapy.
According to the systematic review by Magnan, et al. [5], spontaneous AT rupture is associated with an array of risk factors, both intrinsic and extrinsic. Intrinsic risk factors include age, body weight, systemic diseases, tendon temperature, previous injuries, anatomical variants, genetic predisposition and blood alterations. Extrinsic risk factors include overload and pharmacological agents such as corticosteroids and fluoroquinolones.
Most of AT injury due to the known risk factors occur in the vascular-shed area which is located 5 cm proximal to tendon insertion in the calcaneus [6, 7]. In our case, AT tear was at its footprint in the calcaneus, which is most likely caused by direct effect of osteomyelitis. Essentially, Osteomyelitis is known to affect the bone, periosteum and the surrounding soft tissue [8, 9], but direct affection of the tendon with secondary tendon tear have not been reported previously.
Type II diabetic patients are four to five times more likely to have tendinopathy and tendon tear than non-diabetics. This is explained by disturbance in tendon homeostasis, which can include functional changes such as restriction of range of motion. Structural changes are also reported such as tendon thickening secondary to loss of collagen organization and formation of dystrophic calcification within the tendon substance [10]. Wu et al. reported a case of spontaneous AT rupture in a patient with uncontrolled type II diabetes [11]. Unlike our case, the site of AT rupture was located at the vascular-shed area, which was attributed to connective tissue elastosis and chronic acidosis.
Our patient is known to have uncontrolled type II diabetes mellitus with hypertrophic Charcot foot, in which an extent of AT tendinopathy is expected to be found in such patients. Though being the site of AT rupture is at the footprint, this makes osteomyelitis as a most likely attributer rather than degenerative tendinopathy, whereupon the latter affects the vascular-shed area rather that the footprint.
Conclusion
In conclusion, AT rupture in the setting of osteomyelitis expands the understanding of its attributable factors. Careful attention when viewing diagnostic studies are recommended to evaluate the adjacent tendinous structures in cases of osteomyelitis. We intended to publish this case to increase the awareness of this rare entity among clinicians and radiologists.
Consent for Publication
Consent for publication was obtained from the subject for this case report and all imaging studies.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
This case report received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
-
Khurana R, Torzillo PJ, Horsley M, Mahoney J (2002) Spontaneous bilateral rupture of the Achilles tendon in a patient with chronic obstructive pulmonary disease. Respirology 7(2): 161-163.
-
Kotnis RA, Halstead JC, Hormbrey PJ (1999) Atraumatic bilateral Achilles tendon rupture: an association of systemic steroid treatment. J Accid Emerg Med 16: 378- 379.
-
Mehra A MR, Case R, Croucher C (2004) Bilateral simultaneous spontaneous rupture of the Achilles tendon. Hosp Med 65(5): 308-309.
-
Saltzman CL, Tearse DS (1998) Achilles tendon injuries. J Am Acad Orthop Surg 6(5): 316-325.
-
Magnan B, Bondi M, Pierantoni S, Samaila E (2014) The pathogenesis of Achilles tendinopathy: a systematic review. Foot Ankle Surg 20(3): 154-159.
-
Kawtharani F, Masrouha, KZ, Afeiche N (2016) Bilateral Achilles Tendon Ruptures Associated With Ciprofloxacin Use in the Setting of Minimal Change Disease: Case Report and Review of the Literature. J Foot Ankle Surg 55(2): 276-278.
-
Yasui Y, Tonogai I, Rosenbaum AJ, Shimozono Y, Kawano H, et al. (2017) The Risk of Achilles Tendon Rupture in the Patients with Achilles Tendinopathy: Healthcare Database Analysis in the United States. Biomed Res Int.
-
Maffulli N, Kenward MG, Testa V, Capasso G, Regine R, et al. (2003) Clinical diagnosis of Achilles tendinopathy with tendinosis. Clin J Sport Med 13(1): 11-15.
-
Konter JAD, Knol A, Olsson S, Meyboom RH, Koning GHD (1994) Tendinitis of the Achilles tendon caused by pefloxacin and other fluoroquinolone derivatives. Ned Tijdschr Geneeskd 138(10): 528-531.
-
Nichols AEC, Oh I, Loiselle AE (2020) Effects of Type II Diabetes Mellitus on Tendon Homeostasis and Healing. J Orthop Res 38(1): 13-22.
-
Wu YC, Wang HH, Chang CK, Hsu YC, Huang GS (2012) Spontaneous Achilles tendon rupture in a diabetic neuropathy patient on long-term hemodialysis. QJM 105(12): 1221-1222.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage