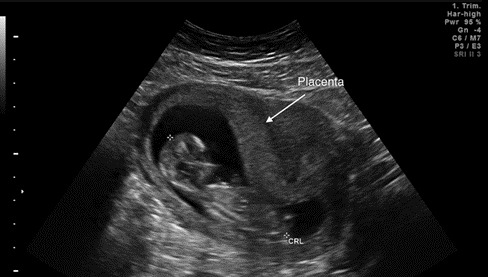
The Placenta: Anatomy, Pathophysiology, Pathological and Ultrasonograpic Findings
Introduction: The placenta is an organ that connects the developing fetus to the mother to serve the major purpose of respiration, excretion and nutrition for the fetus. It is very important for the proper development of the embryo, cushions it from mechanical shocks a major role in assisting the physiological changes that occur during pregnancy. A thorough examination of the placenta plays an important role in providing significant clinical information that may affect the welfare of the fetus and the mother but sadly, it is less evaluated during routine obstetric ultrasound scan. Objective: This study discussed in simplified details, the developmental anatomy of the placenta, related ultrasonography of the appearance of the typical placenta which provides necessary clinical information and help. predict adverse fetal outcomes. Also discussed were some pathological findings that can be seen in routine ultrasound scan with the hematological complications of placenta previa as a focus. Methodology: The research was designed from search engines with reference to valid studies from academic sources including ResearchGate, PubMed and Google Scholar. We also evaluated various related titles, abstracts and full reports for eligibility. Conclusion: The placenta is a very important organ in the development of the fetus but easily overlooked during routine ultrasound and a proper check of the health can avert morbidity and mortality of the fetus.
Introduction
The placenta, in simple terms, is an organ that develops in the uterus and connects the developing fetus to the mother during pregnancy. Its etymology is derived from Latin placenta (flat cake). During intrauterine life it serves to function as a means of communication with regards to physiological exchange between the mother and the fetus according to Harland Mossman, a comparative placentologist. These functions principally include nutrition, respiration and excretion to the growing baby. It is to note that this definition does not clearly state all the functions carried out by the placenta which includes its endocrine function, immunity function to mention but a few.
This article emphasized the development and anatomy of the placenta with respect to its relative ultrasonography during its normal development and in different pathological cases such as: morphology, abnormal size, location, adherence and tumors which can be benign or cancerous.
Anatomy of Normal Placenta
Development and Structure of the Human Placenta
The human placenta and its associated extra- embryonic membranes are formed from the zygote at beginning of intra-uterine life. The two main tissue sources are the trophectoderm that forms the outer boundary of the blastocyst, and the underlying extra embryonic mesoderm. The human placenta forms from the trophectoderm the outer covering of the pre-implantation embryo which forms at approximately five days post fertilization. At this stage the pre-implantation embryo (termed a blastocyst) is segregated into two lineages: inner cell mass (ICM) and the trophectoderm (TE) [1].
During the earliest stages of implantation, the polar TE (the part of the TE that lines the pre-embryoblast) attaches to the endometrium of the uterine cavity of the mother. This part of the TE called the trophoblast develops into the placental epithelium and about the 6th to 7th day post fertilization; the trophoblast forms an invasive population of extra-villous trophoblast cells which fuses to form a primary syncytium. This is called the pre-lacunar phase of placental development [1]. At the 8th day of development the blastocyst is partially embedded in the endometrial stroma. Trophoblast is differentiated into two layers: an inner layer of non-nucleated cells, the cytotrophoblast; and an outer multi-nucleated zone the syncytiotrophoblast.
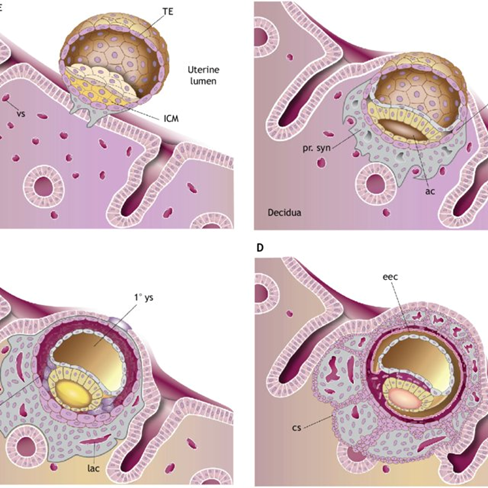
Figure 1: Diagram showing the formation of cytotrophoblast cells depicting the early steps in placenta formation following blastocyst implantation. (A,B) The pre-lacunar stages. (C) The lacunar stage. (D) The primary villous stage. 1° ys, primary yolk sac; ac, amniotic cavity; cs, cytotrophoblastic shell; eec, extra-embryonic coelom; exm, extra-embryonic mesoderm; GE, glandular epithelium; ICM, inner cell mass; lac, lacunae; LE, luminal epithelium; mn. tr, mononuclear trophoblast; pr. syn, primary syncytium; TE, trophectoderm; vs, blood vessels. Source: Development of the human placenta-Scientific Figure on ResearchGate. Available from: https://www.researchgate. net/figure/The-early-stages-of-human-placental-development-Diagram-depicting-the-early-steps-in_fig1_337580682 In the process of implantation, the primary syncytium also known as the syncytiotrophoblasts begins to invade the specialized connective tissue of the endometrium known as the decidua and by the 9th day post fertilization implantation of blastocyst into the endometrium occurs. The stromal core of the placenta, which is derived from the extra embryonic mesoderm (a derivative of trophoblast) gives rise to the fibroblast, a host of resident macrophages and a collection of vascular network.
During the period 9th to 14th day post fertilization (the first menstrual period), the blastocyst is fully embedded in the decidua and is covered by the endometrium. Vacuoles appear and form lacunar in the syncytium that enlarges and merge, separating it into a system of trabaculae. This is known as the Lacunar stag. The syncytial mass also erodes into the decidual glands, allowing secretions to bathe the syncytium [2].
The cytotrophoblast are not in direct contact with maternal tissue but rapidly divide to generate projections that penetrate the syncytiotrophoblast to form primary villi (a cytotrophoblast core with an outer layer of syncytiotrophoblast; this is the Villus stage of development (Figure 1). The basic structural unit of the placenta is the chorionic villus. The villus tree is formed by further proliferation and branching and the lacunar becomes the intervillous space. Cytotrophoblast cells eventually penetrate the syncytiotrophoblast layer and fuse laterally to surround the conceptus in a continuous cytotrophoblast cell between the villous and the decidua. This gives rise to a three-layered covering of the blastocyst: the inner chorionic plate in contact with the original cavity; the villi separated by the intervillous space; and the cytotrophoblast cell in contact with the decidua. After the 12th week of gestation, the intervillous blood flow is completely formed and a Utero- placental circulation with slow flow becomes functional.
The matured placenta is a roughly discoid shaped tissue that is rich in blood vessels making it appear dark red just before birth. It comprises of parenchymal tissues, umbilical cord and membranes. Structurally it has a dimension which includes a diameter measuring about 22cm, weight of about 0.5kg, and thickness of 2.5cm [3].
The placental parenchyma connects the vasculature of the developing fetus with the mother to regulate physiological processes including nutrition, waste removal, hormonal regulation and immune system [4]. The placenta surface includes the chorionic plate which serves as the umbilical cord attachment and a basal plate which lies adjacent to the maternal endometrium. A cavity exits between the chorionic and basal plate known as the intervillous space (Figure 2). It receives 30-40 deeply separated fetal villous sheets.
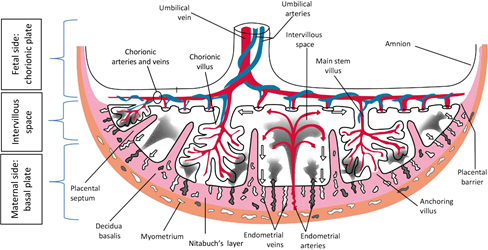
Figure 2: Drawing of the fetal side and maternal side of the placenta in the second half of pregnancy. Fetal side: Chorionic plate that contains the amnion and main stem villi (chorionic villi). Maternal side: Basal plate that contains placental septa and decidua basalis. Red, fetal veins: Umbilical vein, chorionic veins and venules; maternal arteries: endometrial arteries. Blue, fetal arteries: Umbilical arteries, chorionic arteries and arterioles. Pink, decidua basalis, Nitabuch’s layer, placental septa. Brown, myometrium Source: Jansen CHJR, et al. Development of placental abnormalities in location and anatomy A narrative review. Acta Obstet Gynecol Scand. 2020; 99: 983– 993. https://doi.org/10.1111/aogs.13834.
The umbilical cord is a bundle of blood vessels, it’s enclosed into a tubular sheath of amnion which is protected by a gelatinous substance called Wharton’s jelly. It measures about 0.8cm-2.0cm in diameter, 30cm-100cm in length and an average length of 55cm [1, 4]. It consists of an umbilical vein, carrying oxygen rich blood as well as nutrient rich blood to the fetus and two umbilical arteries which conveys deoxygenated blood away from it. About 35ml/min of blood flows through the umbilical cord at 40 weeks of gestation [4].
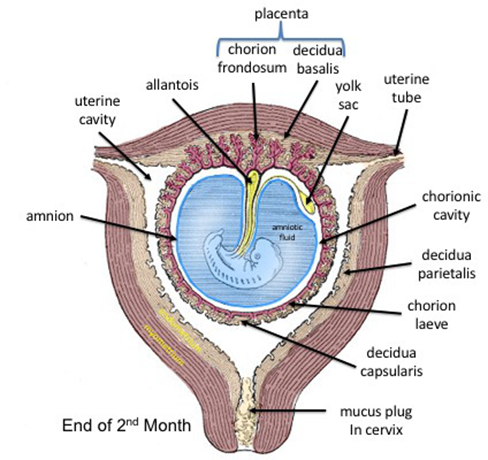
The placental membranes comprise of the amnion and chorion (Figure 3). The amnion is one of the two placental membranes which engulf the fetus during intra-uterine development. It can be visualized in ultrasound from 7th – 8th week of gestation. The chorion which is the outermost membrane around the embryo is bilayered and consists of an outer layer of extra-embryonic mesoderm (trophectoderm) and an inner epiblast derived extra-embryonic mesoderm. It is formed by the 8th day post fertilization. The amnion and chorion fuse between the 14th and 16th week of gestation [5].
Ultrasound of the Normal Placenta
Ultrasonography scan (US) is the initial imaging test done during pregnancy that assesses the health and development of the placenta in most clinical conditions. It uses sound waves to create an image of how the fetus and its placenta is developing in the uterus. The information gotten can be used to calculate fetal age using the starting day of the last normal menstrual period (LNMP), fertilization or conception. Although, examination of the placenta has received less attention than the fetus during routine scans which in part may be due to the varying speed of change of placenta maturation in different pregnancies [6, 7].
Regardless, detailed assessment of the placenta at ultrasonography, provides a foremost role in the evaluation of normal and abnormal pregnancies. As gestation progresses, the placenta increases in length for the first trimester, increases in size and thickness in second and third trimester respectively. With each developmental stage (Table 1), it becomes more echogenic (Figure 4).
| Parameters | Assessment |
|---|---|
| Morphology | Thickness, surface area, difference in diameters and shape |
| Location | Anterior, posterior, fundal or lateral |
| Anatomy | Placenta lobes and cotyledons, placenta anomalies, placenta cord insertion and placenta membranes |
| Implantation | Placenta grading, placenta distance from cervix and placenta blood flow |
Table 1: A methodical sonographic assessment of the placenta should include; [6].
![Figure 4: Ultrasound Images depicting the major stages of placental development. Source: Branco AC, et al. Placental Calcification: Long-standing Questions and New Biomedical Research Directions. In: Aikawa E, (eds) Cardiovascular Calcification and Bone Mineralization. Contemporary Cardiology, Humana, Cham. https://doi. org/10.1007/978-3-030-46725-8_13 The placenta may be visualized as early as 6 weeks of gestation (4 weeks after fertilization) on transvaginal ultrasound when an intrauterine pregnancy may not yet be obvious on transabdominal scan. The image gotten for this procedure shows the chorionic cavity and the echogenic chorionic villi that are implanting. It also illustrates a yolk sac and an umbilical cord. In the beginning stages of the first trimester, the average diameter of the gestational sac increases approximately 1millimeters per day. Although, there’s an increased risk of embryonic death if the diameter of the gestational sac increases beyond 6millimeters from a normal range of 3 to 5millimeters [7,8]. By the end of the 5th week, the average diameter of the gestational sac grows from 16 to 23millimeters. An anembryonic pregnancy should be suspected if a transvaginal ultrasound does not detect an embryo at 16millimeters gestational sac size.](/fulltextimages/10492/fig_4.png)
Figure 4: Ultrasound Images depicting the major stages of placental development. Source: Branco AC, et al. Placental Calcification: Long-standing Questions and New Biomedical Research Directions. In: Aikawa E, (eds) Cardiovascular Calcification and Bone Mineralization. Contemporary Cardiology, Humana, Cham. https://doi. org/10.1007/978-3-030-46725-8_13 The placenta may be visualized as early as 6 weeks of gestation (4 weeks after fertilization) on transvaginal ultrasound when an intrauterine pregnancy may not yet be obvious on transabdominal scan. The image gotten for this procedure shows the chorionic cavity and the echogenic chorionic villi that are implanting. It also illustrates a yolk sac and an umbilical cord. In the beginning stages of the first trimester, the average diameter of the gestational sac increases approximately 1millimeters per day. Although, there’s an increased risk of embryonic death if the diameter of the gestational sac increases beyond 6millimeters from a normal range of 3 to 5millimeters [7, 8]. By the end of the 5th week, the average diameter of the gestational sac grows from 16 to 23millimeters. An anembryonic pregnancy should be suspected if a transvaginal ultrasound does not detect an embryo at 16millimeters gestational sac size.
From the 10th week, transabdominal ultrasound is used for assessment with placenta appearing as a thickened echogenic rim of tissue that covers the amniotic sac (Figure 4) [9]. The intervillous blood flow in the placenta can be demonstrated using the Doppler US by the 12th and 13th week [9]. In addition, chorion and amnion fusion takes place between the 12th and 16th week of pregnancy. The placenta is fully developed during the end of the 1st trimester of pregnancy. Specifically, in the 14th to 15th of gestation, the placenta appears as a prominent hyperechoic area which is referred to as the retroplacental clear space (Figure 5 & 6) [10]. The region behind the placenta known as the hypoechoic area is composed of decidua, myometrium, and uterine vessels.

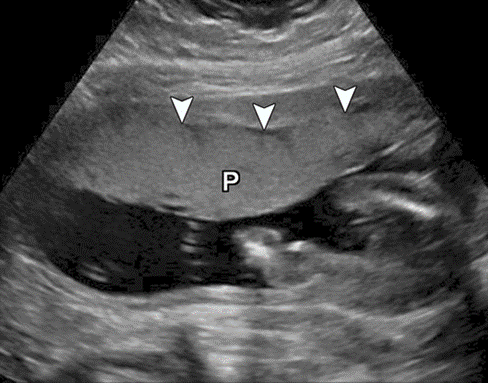
During the second trimester, the ultrasound of the normal placenta reveals a diameter of about 15 to 20centimeters and an average thickness of 2 to 4centimeters at this period that grows spontaneously with gestational age [11]. Also, the insertion of the umbilical cord is mostly central but not in all cases as marginal and velamentous insertion also seldom occurs. The placenta extends to the lateral walls of the uterus from the anterior or posterior walls with a discoid shape, rounded margins and uniform echogenicity. With increasing maturation, internal ill-defined hypoechoic areas known as placental lakes may be seen and the placenta appears more homogenous and hyperechoic in the second and third trimesters (Figures 7 & 8) [12].
![Figure 8: Ultrasound imaging of the Placenta at 35 weeks gestational age. Source: Ozcan T, et al. Pressman, Imaging of the Placenta, Ultrasound Clinics, Volume 3, Issue 1, 2008, Pages 13-22, ISSN 1556-858X, https://doi.org/10.1016/j. cult.2007.12.007. (https://www.sciencedirect.com/ science/article/pii/S1556858X07001429) Developmental changes in the placenta during gestation can be related to the growth and development of the fetus as earlier stated. These changes occur in three major anatomical regions: the amnion chorion plate, the placental body, and the basal layers [13]. Most importantly during maturation in the third trimester, the placenta develops calcifications which is of high significance in a process known as placental grading which is a test of fetal wellbeing (Figure 4).](/fulltextimages/10492/fig_8.png)
Figure 8: Ultrasound imaging of the Placenta at 35 weeks gestational age. Source: Ozcan T, et al. Pressman, Imaging of the Placenta, Ultrasound Clinics, Volume 3, Issue 1, 2008, Pages 13-22, ISSN 1556-858X, https://doi.org/10.1016/j. cult.2007.12.007. (https://www.sciencedirect.com/ science/article/pii/S1556858X07001429) Developmental changes in the placenta during gestation can be related to the growth and development of the fetus as earlier stated. These changes occur in three major anatomical regions: the amnion chorion plate, the placental body, and the basal layers [13]. Most importantly during maturation in the third trimester, the placenta develops calcifications which is of high significance in a process known as placental grading which is a test of fetal wellbeing (Figure 4).
Placental grading as described by Grannum, et al. consists of four stages (grades 0-3) of placental development that they used to relate placental maturation to fetal pulmonary maturity [14]. Placenta ultrasound grading is characterized as follows [15]:
Grade 0: Typically occurs during late first trimester to early second month (10-17 weeks)
- Amnion chorion plate- continuous, well defined and indentation-free.
- Placental body- there’s absence of any echogenic areas with no significant changes.
- Basal layer- there’s absence of basal layer echogenicities. Grade 1: This stage extends from the middle of the second trimester to the beginning of the third trimester (18-29 weeks).
- Amnion chorion plate- well-defined unbroken line due to subtle indentations.
- Placental body- there’s loss of homogeneity due to presence of scattered echogenic appearing within the placenta.
- Basal layer- there’s absence of basal layer echogenicities.
Grade 2: This stage signifies the late third trimester (30 weeks to birth) and is characterized by major modifications in the three layers.
- Amnion chorion plate-presence of more and larger indentations than grade 1.
- Placental body- It is partially divided by the emergence of linear echogenic densities.
- Basal layer- Basal calcifications which are linear small echoes are arranged in a linear fashion along the placenta-decidua junction i.e., their long axis lies parallel to the basal layer. Grade 3: This stage represents the late period of 39 weeks of pregnancy to periods of prolonged gestation before birth.
- Amnion chorion plate- development of multiple depressions which now extend to the basal layer and this may represent the inter cotyledon septa.
- Placental body- complete indentations divides the placenta into compartments known as the cotyledons. The central portion of these compartments show echo- spared or fallout areas.
- Basal layer- dense and echogenic masses persist and become larger and denser.
In this respect, placental grading has only a few usefulness. Also, a relationship between grade 3 placental maturation and subsequent obstetric problems, has been reported by other investigators in particular intrauterine growth retardation and fetal distress during labour [16, 17].
Pathology of the Placenta: Ultrasound Findings
Placental pathology entails abnormalities that affect the placenta during the gestation which can jeopardize the health of the fetus and the mother. Having a good understanding and knowledge proffers insights into both acute and chronic events and how best to approach them. In terms of anatomy and location, the fertilized ovum normally implants and develops in the uterine fundus but the most common placental anomalies are several problems with placentation which are shown in the figure below [18]:
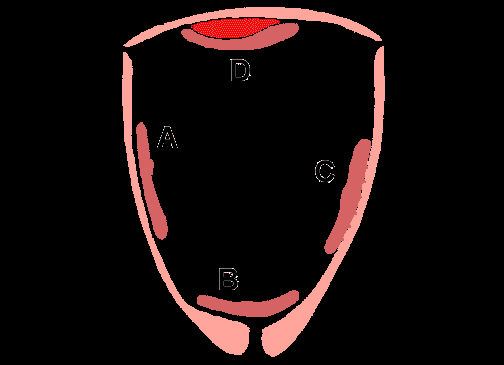
A. Normal Placenta: This depicts the normal implantation of the embryo and placement of placenta to ensure the proper growth of the embryo.
B. Placental Previa: This is caused by a very low-lying placenta or a placenta tissue that implants over the internal os and in the process causes occlusion and a less functional placenta results (Figures 9 & 10) [19]. A placenta is termed low lying when the placental edge does not cover the internal os but is within 2 cm of it. The Incidence of placenta previa is approximately 5 per 1000 deliveries worldwide [20]. While in Nigeria, most studies report a low incidence of placenta previa due to the socio- cultural and economic factors in this environment that do not allow most women to seek medical attention even when in dire need [21, 22]. A clinical manifestation of the disorder is a painless vaginal bleeding after 20 weeks of pregnancy. Possible risk factors for placenta previa includes: smoking, multifetal pregnancy, myomectomy, older maternal age and history of cesarean delivery, and previous abortion. Accompanying this disorder are several complications that includes: severe hemorrhage of the cervix during the process of child birth or labor due to disruption of the placenta as the cervix dilates which will result in anemia, preterm premature rupture of the membranes and vasa previa amongst others. Due to these severe complications, four categories of placenta previa are distinguished [23]:

Type 1: Low Lying/Implantation Placenta. Edge of the implanted placenta margin dips into the lower uterine segment within 2 to 3.5cm of internal cervical os. Type 2: Marginal Placenta. The placenta does not totally occlude the internal cervical os but cover about 2cm of its surface.
Type 3: Partial Previa. In this type of placenta previa, a fully dilated internal cervical os is not covered by the placenta but when the placenta covers the internal os when closed. Type 4: Complete Previa. This is the most critical form of placenta previa as the internal os becomes fully occluded even when fully dilated.
C. Placenta Accreta: This defect is caused by a lack of formation of a normal decidual plate. Thus, the chorionic villi may penetrate deep into myometrium of the uterus which results in difficulty of the placenta to separate normally during childbirth. Severe blood loss results. D. Abruptio Placenta: this disorder is caused by premature separation of the placenta prior to labor. The vasculature of the fetus is disrupted to a large extent due to the formation of a retroplacental blood clot that increases in size depending on the severity of the separation. This leads severe bleeding resulting in anemia of the mother and requires an immediate emergency intervention.
Other abnormalities of the placenta that are of utmost clinical importance include: abnormally invasive placentas, low-lying placenta and preeclampsia.
Conclusion
The placenta plays a major role in growth and development of the fetus. The fetus is totally reliant on the placenta for survival. Therefore, placenta-related pathologic disorders may result to complications that may have a direct impact on fetal morbidity and mortality. The best way to evaluate occurrence or non-occurrence of these pathological disorders is to ensure that a thorough examination of the placenta is done when administering routine antenatal care. Radiologists and other professionals involved in antenatal prenatal ultrasound should familiarize themselves with the various pathologic disorders of the placenta. This is necessary in order to ensure referral for fast and appropriate maternal and fetal care.
Acknowledgment
We acknowledge the immense contribution of our research assistants in the successful completion of the work. Similarly, we express our sincere gratitude to the physicians for the participation in the study. We appreciated Mr Kayode for his assistance in typing and statistical analysis Competing Interest: The authors declared no competing interest.
Funding: None
Ethical Approval: Not required
References
-
Turco MY, Moffet A (2019) Development of human placenta. Development 146(22).
-
Knöfler M, Haider S, Saleh L, Pollheimer J, Gamage TKJB, et al. (2019) Human placenta and trophoblast development: key molecular mechanisms and model systems. Cell Mol Life Sci 76(18): 3479-3496.
-
Jauniaux E, Ramsay B, Campbell S (1994) Ultrasonographic investigation of placental morphologic characteristics and size during the second trimester of pregnancy. Am J Obstet Gynecol 170(1 Pt 1): 130-137.
-
Kiserud T, Acharya G (2004) The fetal circulation. Prenat Diagn 24(13): 1049-1059.
-
Bibbo C, Little SE, Bsat J, Botka KA, Benson CB, et al. (2016) Chorioamniotic Separation Found on Obstetric Ultrasound and Perinatal Outcome. AJP Rep 6(3): e337- 343.
-
Abramowicz JS, Sheiner E (2008) Ultrasound of the Placenta: A Systematic Approach Part I: Imaging. Placenta 2(3): 225-250.
-
Abramowicz JS, Sheiner E (2007) In utero imaging of the placenta: importance for diseases of pregnancy. Placenta A: S14-22.
-
Kurtz AB, Needleman L, Pennell RG, Baltarowich O, Vilaro M, et al. (1992) Can detection of yolk sac in the first trimester be used to predict the outcome of pregnancy: a prospective sonographic study. AJR 158(4): 843-847.
-
Kanne JP, Lalani TA, Fligner CL (2005) The placenta revisited: radiologic-pathologic correlation. Curr Probl Diagn Radiol 34(6): 238-255.
-
Brownbill P, Mahendran D, Owen D, Swanson P, Thornburg KL, et al. (2000) Denudations as paracellular routes for alphafetoprotein and creatinine across the human syncytiotrophoblast. Am J Physiol Regul Integr Comp Physiol 278(3): R677-683.
-
Elsayes KM, Trout AT, Friedkin AM, Liu PS, Bude RO, et al. (2009) Imaging of the placenta: a multimodality pictorial review. Radiographics 29(5):1371-1391.
-
Jansen CHJR, Kleinrouweler CE, Kastelein AW, Ruiter L, Leeuwen EV, et al. (2020) Follow-up ultrasound in second-trimester low- positioned anterior and posterior placentae: prospective cohort study. Ultrasound Obstet Gynecol 56(5): 725-731.
-
Heller HT, Mullen KM, Gordon RW, Reiss RE, Benson CB (2014) Outcomes of pregnancies with a low-lying placenta diagnosed on second- trimester sonography. J Ultrasound Med 33(4): 691-696.
-
Grannum PA, Berkowitz RL, Hobbins JC (1979) The ultrasonic changes in the maturing placenta and their relation to fetal pulmonary maturity. AmJ Obstet Gynecol 133(8): 915-922.
-
Zaidi SF, Moshiri M, Osman S, Robinson TJ, Siebert JR, et al. (2016) Comprehensive Imaging Review of Abnormalities of the Placenta. Ultrasound 32(1): 25-42.
-
Fadl S, Moshiri M, Fligner CL, Katz DS, Dighe M (2017) Placental Imaging: Normal Appearance with Review of Pathologic Findings. Radiographics 37(3): 979-998.
-
Radswiki T, Qureshi P (2010) Placenta accreta. Radiopaedia.
-
Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, et al. (2006) Maternal morbidity associated with multiple repeat cesarean deliveries. Obstet Gynecol 107(6): 1226-1232.
-
Jansen CHJR, Kastelein AW, Kleinrouweler CE, Leeuwen EV, Jong KHD, et al. Development of placental abnormalities in location and anatomy. Acta Obstet Gynecol Scand 99(8): 983-993.
-
Cresswell JA, Ronsmans C, Calvert C, Filippi V (2013) Prevalence of placenta praevia by world region: A systematic review and meta-analysis. Trop Med Int Health 18(6): 712-724.
-
Burodo AT, Shehu CE (2013) Placenta praevia at Usmanu Danfodiyo University Teaching Hospital, Sokoto: A 5-year review. Sahel Med J 16(2): 56-59.
-
Nwobodo EI (2006) Obstetric emergencies as seen in a tertiary health institution in North-Western Nigeria: Maternal and fetal outcome. Niger Med Practit 49(3): 54-55.
-
Matsuzaki S, Kimura T (2019) Vasa Previa. N Engl J Med 380(3): 274.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage