“Unreported Nuclear Medicine Findings in Congenital Emangiomas Involving Lower Limb (Klippel-Trenaunay Syndrome)”
Hemangioma is a prevalent problem among the vascular abnormalities and is the very common benign tumor of infancy and childhood. It is characterized by rapid growth of endothelial cells that commonly arises in the head and neck region (60%), followed in frequency by the trunk (25%) and extremities (15%) [1]. Two types of congenital hemangiomas exist including rapidly involuting congenital hemangiomas and noninvoluting congenital hemangiomas.
Discussion
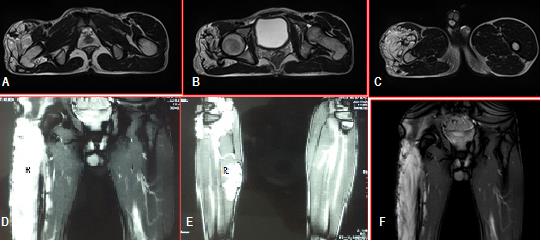
The patient presented with haemangioma of the lower limband was evaluated with three basic diagnostic tests to the check the extent and severity of the issue and appropriate designing of the therapy.In the management of hemangiomas, plain X-rays of the long bones (scanograms) are most helpful to see bone related abnormalities [3]. Lower limb X-Rays of the patient were taken that clearly showed hypertrophy of the right limb that appeared as a white mass as compared to the remaining image.
Magnetic resonance imaging (MRI) helps in accurate visualization of patient’s soft tissues. Hypertrophy of muscle and bone, presence of dilated veins and arteries, and pelvic and abdominal vascular abnormality can be assessed with MRI [12, 16]. It is alsohelpful in differentiating bone, fat, muscle hypertrophy and lymphedema of muscle, fat and bone [3]. MRI is useful in visualizing the extent of lesions along with infiltration of deep body tissues before treatment [13, 14, 17]. In this way, MRI helps in designing therapy for the patient, monitoring patient’s response to therapy, and to determine the disease prognosis [18]. MRI of the patient was done that showed that the patient hashemangiomas in the right leg, appearing white as compared to remaining part of the image.
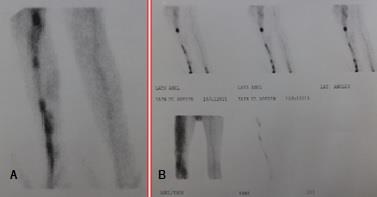
Scintigraphy may be utilized to assess regional blood flow, patency of valves and bone vascularity in KTS [12]. When vein stripping, sclerosis, or ligation, or sclerosis are essential radionuclide venography or contrast venography is done to depict perforators, collaterals, and deep connections of the extremities [19, 20]. Various techniques were developed for better visualization of the deep veins, including retrograde venography, ascending venography, with pericalcaneal, femoral, and peritrochanteric injection of contrast material [21]. Scintivenography of the patient was done that showed increased blood flow and bone vascularity in the right limb of patient along with patent deep valves. KTS disease varies greatly from patient to patient, so every patient needs different treatment on the basis of his or her clinical presentation. For better management of the patient and to achieve the aim of improving patient’s quality of life, a multidisciplinary disease management approach is essential to be followed [12, 22, 23]. Patients of KTS should be treated conservatively, with special emphasis on symptomatic relief. Patients with functional limbs and having little or no edema, ulceration, bleeding, or pain are usually managed conservatively [12, 24]. Elastic compression stockings, elevation of the affected limb or intermittent pneumatic compression pumps are extensively used in managing patients with varicose veins, edema and swelling of the extremities [4, 12]. Compression stockings are highly recommended for all KTS patients, especially when they start walking [12, 23]. Patients with cellulitis or thrombophlebitis should be managed with antibiotics, analgesics, and elevation [24]. Corticosteroids should be used when appropriate. Antibiotics are recommended only in the case of infections [12, 25]. Proper skin care and regular cleansing should be done in patients with minor KTS to prevent the development of sever disabling conditions [12, 23]. Our patient was being considered for surgical procedure for varicose veins in a peripheral setup but with proper investigations it became obvious that KTS is genetic disorder that involves no improvement in patient’s quality of life after surgery. As the disease has no permanent cure so no surgery was advised. Over the counter analgesic and anti-inflammatory products were recommended to treat pain and inflammation. The use of elastic compression stockings and elevation of the right leg were emphasized for treating the varicose veins. Some
life style modifications like the use of heel inserts was promoted that help the patient during walking or standing. It was repeatedly emphasized that the patient should routinely clean the affected area to prevent the growth of microbes. Patient was advised for routine follow ups as it can help in accurate and timely management of patient in the case of any infection or other complexities.

Conclusion
The patient presented to hospital was having Klippel Trenaunay Syndrome with varicose veins. Because of the genetic origin of KTS, no surgery was performed and the patient was recommended to use analgesics and follow other life style modifications for improvement of his quality of life. Therefore in the management of suspected KTS it may be suggested that clinical examination should follow with x-rays and if still found ambiguous either MRI or Scintigram may be of help to rule out KTS.
References
-
Mulliken J B (1988) Diagnosis and natural history of hemangiomas.
-
Krol A, CJ MacArthur (2005) Congenital hemangiomas: rapidly involuting and noninvoluting congenital hemangiomas. Archives of facial plastic surgery 7(5): 307-311.
-
Gloviczki P, and D Driscoll (2007) Klippel–Trenaunay syndrome: current management. Phlebology 22(6): 291-298.
-
Jacob AG, Anila G Jacob, David J Driscoll, William J. Shaughnessy,Anthony W Stanson, Ricky P Clay,et al. (1998) Klippel-Trenaunay syndrome: spectrum and management. in Mayo Clinic Proceedings, Elsevier 73(1): 28-36.
-
Cohen MM (2000) Klippel‐Trenaunay syndrome. American journal of medical genetics 93(3): 171-175.
-
Tian X, M Liu, R Kadaba (2004) Positional cloning of a novel angiogenic factor gene: VG5Q mutations cause susceptibility to KTS. Nature 427(1): 640-645.
-
Oduber C E, C M van der Horst, R C Hennekam (2008) Klippel-Trenaunay syndrome: diagnostic criteria and hypothesis on etiology. Annals of plastic surgery 60(2): 217-223.
-
Zea M I, Mohammad Hanif, Mohammad Habib, Ahmed Ansari et al. (2009) Klippel-Trenaunay Syndrome: a case report with brief review of literature. Journal of dermatological case reports 3(4): 56-59.
-
Weber F P (1906) Angioma-formation in connection with hypertrophy of limbs and hemi-hypertrophy.
-
Breugem C C, Merkus MP, Smitt JH, Legemate DA, van der Horst CM, et al. (2004) Quality of life in patients with vascular malformations of the lower extremity. British journal of plastic surgery 57(8): 754-763.
-
Hannawi S, I Salmi (2013) Klippel Trenaunay Syndrome, Inverse Klippel Trenaunay Syndrome: Hypertrophy of Lower Limbs and Atrophy of the Upper Limbs and Facial Muscles: Case Report and Literature Review. J Clin Exp Dermatol Res. 4(172): 2.
-
Kihiczak G G, Meine JG, Schwartz RA, Janniger CK (2006) Klippel–Trenaunay syndrome: a multisystem disorder possibly resulting from a pathogenic gene for vascular and tissue overgrowth. International journal of dermatology 45(8): 883-890.
-
Dubois J, Laurent Garel,Andrée Grignon, Michèle David, Louise Laberge, et al. (1998) Imaging of hemangiomas and vascular malformations in children. Academic radiology 5(5): 390-400.
-
Dubois J, L Garel (1999) Imaging and therapeutic approach of hemangiomas and vascular malformations in the pediatric age group. Pediatric radiology 29(12): 879-893.
-
Enjolras O (1997) Classification and management of the various superficial vascular anomalies: hemangiomas and vascular malformations. The Journal of dermatology 24(11): 701-710.
-
Howlett D C, Roebuck DJ, Frazer CK, Ayers B (1994) The use of ultrasound in the venous assessment of lower limb Klippel-Trenaunay syndrome. European journal of radiology 18(3): 224-226.
-
Kern, S, Niemeyer C, Darge K, Merz C, Laubenberger J, Uhl M (2000) Differentiation of vascular birthmarks by MR imaging: An investigation of hemangiomas, venous and lymphatic malformations. Acta Radiologica 41(5): 453-457.
-
Laor T, P Burrows (1998) Congenital anomalies and vascular birthmarks of the lower extremities. Magnetic resonance imaging clinics of North America 6(3): 497-519.
-
Phillips GN, Gordon DH, Martin EC, Haller JO, Casarella W (1978) The Klippel-Trenaunay Syndrome: Clinical and Radiological Aspect 1. Radiology 128(2): 429-434.
-
Burrows P E, Tal Laor, Harriet Paltiel, Richard L Robertson (1998) Diagnostic imaging in the evaluation of vascular birthmarks. Dermatologic clinics 16(3): 455-488.
-
Thoma M L, G Macfie (1974) Phlebography in the Klippel-Trenaunay syndrome. Acta Radiologica Diagnosis (Sweden) 15(1): 43-56.
-
Noel A A, Gloviczki P, Cherry KJ, Rooke TW, Stanson AW, Driscoll DJ (2000) Surgical treatment of venous malformations in Klippel-Trenaunay syndrome. Journal of vascular surgery 32(5): 840-847.
-
Enjolras O, J B Mulliken (1993) The current management of vascular birthmarks. Pediatric dermatology 10(4): 311-333.
-
Meine J, R Schwartz, C Janniger (1997) Klippel- Trenaunay-Weber syndrome. Cutis 60(3): 127-132.
-
Viljoen D, N Saxe, J Pearnj, P Beighton (1987) The cutaneous manifestations of the Klippel‐Trenaunay‐Weber syndrome. Clinical and experimental dermatology 12(1): 12-17.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance