Association between Hypothyroidism and Chronic Kidney Disease in Patients with Type 2 Diabetes Mellitus in Saudi Community b based Hospital- A Retrospective Single Centre Study
Background and objective: The association between type 2 diabetes (T2DM) complicated with chronic kidney disease (CKD) and hypothyroidisms were not well studied. To estimate retrospectively the prevalence of hypothyroidism in patients with T2DM complicated with CKD in Saudi community based hospital. Design: We analyzed retrospectively 1364 participants with T2DM whom are between the ages 20 to 96 years. All patients were from the population of the Primary health centre at King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia. All data were collected on the basis of a review of electronic medical data. Patients with Thyrotropin level (TSH) above the normal range of TSH for our laboratory reference, history of hypothyroidism and taking thyroid replacement therapy were included. Patient who are pregnant were excluded. All patients in the present study fulfilled the revised National Kidney Foundation criteria for the diagnosis of CKD. Results: Out of 1286 subjects with T2DM, there were 346 cases (26.9%) male and 940 cases (73.1%) were female with mean age 55.4±12.3 and body mass index 31.8±6.3 kg/m2. There were 53 cases (4.1%), 736 cases (57.2%) and 346 cases (26.9%) with CKD, hypertension and hypothyroidism respectively. The mean TSH and FT4 value was 4.2±8.0 mIU/l and 15.1±2.9 pmol/l respectively. Among cases of T2DM and CKD, there were 21 cases (39.6 %) with hypothyroidism, p=0.04. Regression analysis of odd ratio of risk factors for patients with T2DM and CKD with hypothyroidism showed that male gender, age, presence of hypothyroidism and HbA1c were associated with higher likely hood of CKD, (OR=11.5; 95% confidence interval [CI]=5.2, 25.6), p
Mohammad A Melibari1 and Bandari K Aljabri4
khalidsaljabri@yahoo.com patients with T2DM complicated with CKD in Saudi community based hospital.
Kidney Foundation criteria for the diagnosis of CKD.
Association between Hypothyroidism and Chronic Kidney Disease in Patients with Type 2 Diabetes Mellitus in Saudi Community b based Hospital- A Retrospective Single Centre Study Diabetes Obes Int J
15.1±2.9 pmol/l respectively. Among cases of T2DM and CKD, there were 21 cases (39.6 %) with hypothyroidism, p=0.04.
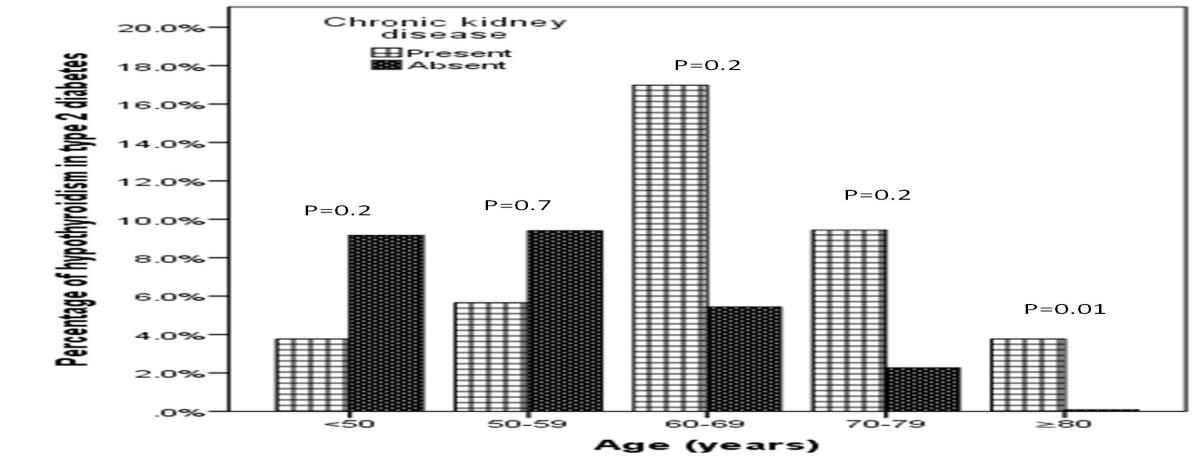
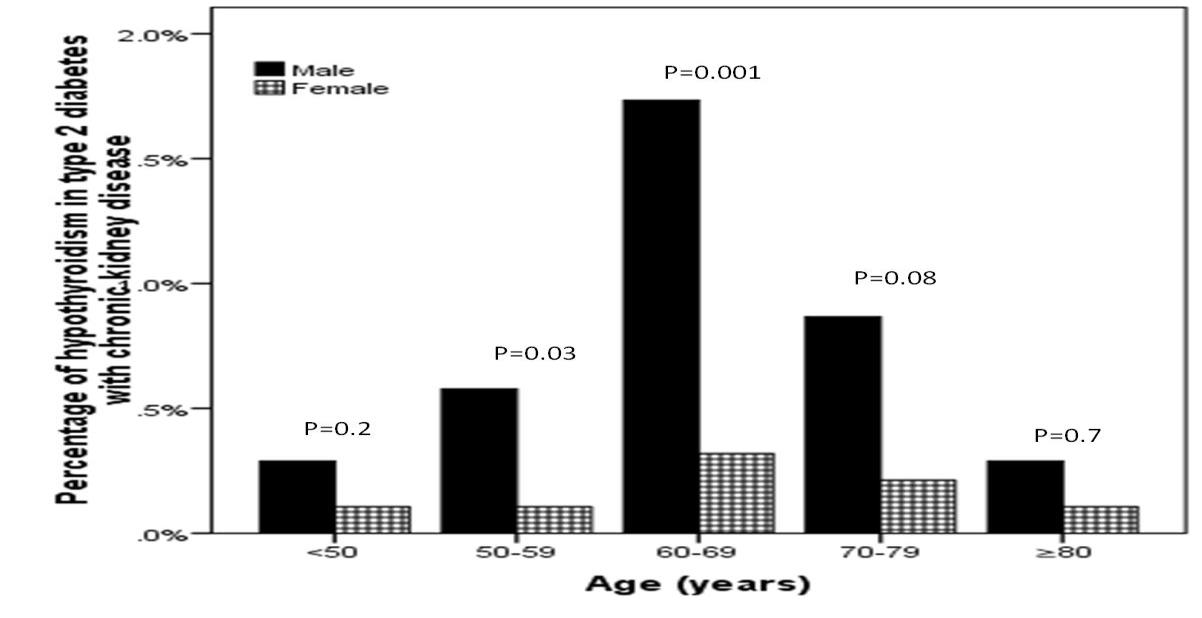
Regression analysis of odd ratio of risk factors for patients with T2DM and CKD with hypothyroidism showed that male gender, age, presence of hypothyroidism and HbA1c were associated with higher likely hood of CKD, (OR=11.5; 95% confidence interval [CI]=5.2, 25.6), p<0.0001), (OR=1.1; 95% CI=1.04, 1.1), p=0.004), (OR=4.4; 95% CI=2.1, 9.1), p<0.0001) and (OR=1.2; 95% CI=1.04, 1.4), p=0.01) respectively. Hypothyroidism with CKD was more prevalent in the seventh decade (17%). Prevalence of hypothyroidism was more prevalent across all age groups and significantly more prevalent in males as compared to females in the sixth (1.7% vs. 0.3%) and seventh (0.9% vs. 0.2%) decades.
Conclusion: We conclude that despite the limitations of this hospital-based retrospective study, hypothyroidism is highly prevalent in cohort of Saudis with CKD and T2DM. The majority of our patients with primary hypothyroidism in our finding were predominantly males. These two observations remain to be validated by population-based studies. In the absence of registry data, larger cooperative studies involving diverse population samples from multiple centers could help to provide further information on the true frequency nationally.
Keywords: Chronic Kidney Disease; Hypothyroidism; Type 2 Diabetes; Saudi Arabia
Introduction
Hypothyroidism has increased recently and is considered the commonest endocrine diseases [1]. Diabetes Mellitus is the commonest endocrine disorder, leading cause of death worldwide [2]. Saudi Arabia is the seventh of the top ten countries in terms of the prevalence of diabetes among the adult population aged 20-79 years [3].
Despite the growing literature about other metabolic and hormonal abnormalities that begin at much milder degrees of renal insufficiency, little is known about thyroid abnormalities or related adaptations in persons with chronic kidney disease (CKD) [4].
While numerous contributing factors have been suggested, including altered iodine metabolism and autoimmune thyroiditis, the exact mechanisms remain unclear. One previous study has examined the prevalence of hypothyroidism among patients with CKD. Among a small group of patients with diabetic and nondiabetic nephropathy, 24% of study subjects had overt or subclinical hypothyroidism, with a higher prevalence among patients with diabetes [5]. Lo, et al. [6] reported a prevalence of hypothyroidism of 23.1% in CKD patients. In another study, clinically apparent hypothyroidisms have been reported to occur in 18-20% of patients with CKD not requiring renal replacement therapy [7].
Thus, the present study was conducted to find out the relationship between CKD and hypothyroidism in patients with type 2 diabetes (T2DM) in a cohort of Saudi population.
Methods
We analyzed retrospectively 1286 participants whom are between the ages 20 to 96 years. All patients were from the population of the Primary health centre at King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia. All data were collected on the basis of a review of electronic medical data. Patients with Thyrotropin level (TSH) above the normal range of TSH for our laboratory reference, history of hypothyroidism and taking thyroid replacement therapy were included. Patient who are pregnant were excluded. The reference range values of TSH 0.22-4.2 MIU/L, Free T4 12.0-22.0 pmol/L. Participants were defined as having T2DM according to self-report, clinical reports, use of antidiabetic agents and HbA1c (≥6.5) [8]. HbA1c was expressed as percentage. High performance liquid chromatography was used. HTN was defined when the systolic blood pressure was ≥130 mm Hg and/or diastolic blood pressure was ≥85 mm Hg in addition to receiving any medication for hypertension [9]. All patients in the present study fulfilled the revised National Kidney Foundation criteria for the diagnosis of CKD [10]. The independent relationship between the stratified risk factors and the odds ratio of having albuminuria were analyzed using logistic regression. The
total number of cohort were separated on basis of age values into five groups: <50 years, 50-59 years, 60-69 years, 70-79 years and ≥80 years.
Statistical Analysis
Continuous variables were described using means and Standard Deviations. Univariate analysis of baseline demography both between groups, were accomplished using unpaired t-test and Chi square test were used for categorical data comparison. Regression analysis was performed to assess for odd ratio (OR). P value <0.05 indicates significance. The statistical analysis was conducted with SPSS version 22.0 for Windows.
Results
Out of 1286 subjects with T2DM included, there were 346 cases (26.9%) male and 940 cases (73.1%) were female with mean age 55.4±12.3 and BMI 31.8±6.3 kg/m2, Table
- There were 53 cases (4.1%), 736 cases (57.2 %) and 346 cases (26.9%) with CKD, HTN and hypothyroidism respectively. The mean TSH and FT4 value was 4.2±8.0 mIU/l and 15.1±2.9 pmol/l respectively. Among cases of T2DM and CKD, there were 21 cases (39.6%) with hypothyroidism, p=0.04, Table
- Regression analysis of odd ratio of risk factors for patients with T2DM and CKD with hypothyroidism showed that male gender, age, presence of hypothyroidism and HbA1c were associated with higher likely hood of CKD, (OR=11.5; 95% confidence interval [CI]=5.2, 25.6), p<0.0001), (OR=1.1; 95% CI=1.04, 1.1), p=0.004), (OR=4.4; 95% CI=2.1, 9.1), p<0.
| Parameters | Total (1286) | |||||
|---|---|---|---|---|---|---|
| Age (years) | 55.4 ±12.3 | |||||
| Gender | Male | 346 (26.9) | ||||
| Female | 940 (73.1) | |||||
| Body mass index (kg/m2) | 31.8 ±6.3 | |||||
| Hypertension | 736 (57.2) | |||||
| Chronic kidney disease | 53 (4.1) | |||||
| Hypothyroidsm | 346 (26.9) | |||||
| HbA1c | 8.1 ±2.2 | |||||
| TSH ( mIU/l) | 4.2 ±8.0 | |||||
| FT4 ( pmol/l) | 15.1 ±2.9 | |||||
| Serum creatinine (μmol/L) | 69.2 ±26.1 |
Table 1: Base line characteristic of patients with type 2 diabetes [mean±standard deviation or number (%)].
| Chronic kidney disease | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Parameters | Present | Absent | P value | |||||||
| 53 ( 4.1 ) | 1233 ( 95.9 ) | |||||||||
| Age (years) | 64.5 ±10.7 | 55.0 ±12.2 | <0.0001 | |||||||
| Gender | Male | 36 ( 67.9 ) | 320 ( 25.1 ) | <0.0001 | ||||||
| Female | 17 ( 32.1 ) | 923 ( 74.9 ) | ||||||||
| Body mass index (kg/m2) | 30.4 ±6.9 | 31.9 ±6.3 | 0.1 | |||||||
| Hypertension | 44 ( 83.0 ) | 692 ( 56.1 ) | <0.0001 | |||||||
| Hypothyroidism | 21 ( 39.6 ) | 325 ( 26.4 ) | 0.04 | |||||||
| HbA1c | 9.2 ±2.2 | 8.1 ±2.2 | <0.0001 | |||||||
| TSH ( mIU/l) | 4.0 ±3.5 | 4.2 ±8.1 | 0.9 | |||||||
| FT4 ( pmol/l) | 15.1 ±2.8 | 15.1 ±2.9 | 0.9 | |||||||
| Serum creatinine (μmol/L) | 145.4 ±47.9 | 66.0 ±18.8 | <0.0001 |
Table 2: Comparison between patients with type 2 diabetes with and without chronic kidney disease [mean±standard deviation or num
| Parameters | Odd Ratio | P value | ||||||
|---|---|---|---|---|---|---|---|---|
| Male gender | 11.5 (5.2-25.6) | <0.0001 | ||||||
| Age (years) | 1.1 (1.04-1.1) | 0.004 | ||||||
| Hypertension | 2.2 (0.98-1.1) | 0.06 | ||||||
| Hypothyroidism | 4.4 (2.1-9.1) | <0.0001 | ||||||
| HbA1c | 1.2 (1.04-1.4) | 0.01 |
Table 3: Regression analysis for odd ratio of risk factors for patients with type 2 diabetes and chronic kidney disease.
Discussion
Among a nationally representative sample of Saudis, we found an increased prevalence of hypothyroidism in persons with CKD, independent of age and gender. The current study revealed that hypothyroidism in patients with T2DM complicated by CKD was found in 39.6 %. To our knowledge, this is the first national and the largest study to explore the association between hypothyroidism and CKD in T2DM population. Chronic kidney disease is a worldwide public health problem. They are the 12th cause of death and 17th cause of disability respectively [11]. The association between diabetes and thyroid disease is well known. Thyroid diseases are also common in the general population. Most reports documenting hypothyroidism with renal impairment have described patients with unexplained worsening of pre-existing renal disease of an alternative aetiology. Recent epidemiological studies, identifying a high prevalence of thyroid dysfunction amongst patients with renal impairment, lend a new importance to the phenomenon of reversible hypothyroidism-induced renal impairment. Clinically-apparent hypothyroidism occur in 18–20% of patients with chronic kidney disease not requiring renal replacement therapy, with the prevalence rising as the degree of renal impairment worsens [6, 7].
The causal relationship between hypothyroidism and CKD is also uncertain. Increased prevalence of goiter and thyroid gland volume have been reported in patients with end-stage renal disease (ESRD), and it has been suggested that primary hypothyroidism may be more common in patients with ESRD compared with the general population [12, 13, 14]. Despite the growing literature about other metabolic and hormonal abnormalities that begin at much milder degrees of renal insufficiency, little is known about thyroid abnormalities or related adaptations in persons with CKD who do not require maintenance dialysis [4]. Although numerous hypothesis for contributing factors, like altered iodine metabolism, decreased peripheral sensitivity to hormones, and autoimmune thyroiditis, the exact underlying mechanisms linking advanced CKD and primary thyroid dysfunction remain unclear [7]. One previous study has examined the prevalence of hypothyroidism among patients with CKD not requiring dialysis. Among a small group of patients with diabetic and nondiabetic nephropathy, 24% of study subjects had overt or subclinical hypothyroidism, with a higher prevalence among patients with diabetes [5].
The present study showed that the prevalence of hypothyroidism in patients with T2DM complicated by CKD was more in males (61.9%) as compared to females (38.1%), p<0.0001. This is consistent with the study of Shantha, et al. which showed prevalence of disease was higher in males (73.5%) as compared to females (26.5%) out of 137 ESRD patients and in contrast to the study showed that the prevalence of hypothyroidism was 25%, which was more in females (52%) as compared to males (48%) [15, 16].
Hypothyroidism occurs in all ages, but it is usually more prevalent, in both community- and hospital-based populations, in older people in their sixth and seventh decades [17, 18]. The present study showed that the prevalence of hypothyroidism was highest in age group of 60-69 years which older than others. 15 The risk of CKD, increased by 4.4 for hypothyroidism as compared to euthyroidism, which remained significant after adjustment for other potential risk factors of CKD.
We aimed to identify the frequency of hypothyroidism in patients with T2DM complicated with CKD in primary health care setting. Furthermore, due to the retrospective nature of this study, the observed population reflects a selected yet comprehensive group of patients rather than the general population. Our study could be limited by the question of clustering of cases within the study region and the effect that might have on our estimates, in addition, the current study population may appear limited in size and therefore may underestimate the true frequency of hypothyroidism in patients with T2DM complicated with CKD. In addition, the study shares the limitations of all retrospective studies.
We conclude that despite the limitations of this hospital-based retrospective study, hypothyroidism is highly prevalent in cohort of Saudis with CKD and T2DM. The majority of our patients with primary hypothyroidism in our finding were predominantly males. These two observations remain to be validated by population-based studies. In the absence of registry data, larger cooperative studies involving diverse population samples from multiple centers could help to provide further information on the true frequency nationally. Acknowledgement: The author would like to thank all colleagues from the Department of primary care for helping in data collection.
Conflict of Interests
The authors declare no conflict of interests.
References
-
Garmendia Madariaga A, Santos Palacios S, Guillén- Grima F, Galofré JC (2014) The incidence and prevalence of thyroid dysfunction in europe: a metaanalysis. J Clin Endocrinol Metab 9(3)9: 923-931.
-
Faghilimnai S, Hashemipour M, Kelishadi B (2006) Lipid profile of children with type 1 diabetes compared to controls. ARYA J 2(1): 36-38.
-
IDF Diabetes Atlas 5th edition 2012 update. International Diabetes Federation.
-
Hsu CY, Mcculloch CE, CurhanN GC (2002) Epidemiology of anemia associated with chronic renal insufficiency among adults in the United States: Results from the Third National Health and Nutrition Examination Survey. J Am Soc Nephrol 13(2): 504- 510.
-
Bando Y, Ushiogi Y, Okafuji K, Toya D, Tanaka N, et al. (2002) Non-autoimmune primary hypothyroidism in diabetic and non-diabetic chronic renal dysfunction. Exp Clin Endocrinol Diabetes 110(8): 408-415.
-
Lo JC, Chertow GM, Go AS, Hsu CY (2005) Increased prevalence of subclinical and clinical hypothyroidism in persons with chronic kidney disease. Kidney Int 67(3): 1047-1052.
-
Chonchol M, Lippi G, Salvagno G, Zoppini G, Muggeo M, et al. (2008) Prevalence of subclinical hypothyroidism in patients with chronic kidney disease. Clin J Am Soc Nephrol 3(5): 1296-1300.
-
American Diabetes Association (2019) Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 42(S1): S13-S28.
-
Paul K Whelton, Robert M Carey, Wilbert S Aronow, Donald E Casey, Karen J Collins, et al. (2017) ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC /NMA/PCN A Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 71(6): e13-e115.
-
Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, et al. (2012) KDOQI US Commentary on the 2012 KDIGO Clinical Practice Guideline for the Evaluation and Management of CKD. American Journal of Kidney Diseases 63(5): 713-735.
-
Renal Data System (2003) USRDS 2003 annual data report: atlas of end-stage renal disease in the United States. In: Bethesda Md (Ed.), National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases.
-
Lim VS, Fang VS, Katz AI, Refetoff S (1997) Thyroid dysfunction in chronic renal failure. A study of the pituitary-thyroid axis and peripheral turnover kinetics of thyroxine and triiodothyronine. J Clin Invest 60(3): 522-534.
-
Kaptein EM, Quion-Verde H, Chooljian CJ, Tang WW, Friedman PE, et al. (1988) The thyroid in end-stage renal disease. Medicine (Baltimore) 67(3): 187-197.
-
Hegedüs L, Andersen JR, Poulsen LR, Perrild H, Holm B, et al. (1985) Thyroid gland volume and serum concentrations of thyroid hormones in chronic renal failure. Nephron 40(2): 171-174.
-
Shantha GPS, Kumar AA, Bhise V, Khanna R, Sivagnanam K, et al. (2011) Prevalence of subclinical hypothyroidism in patients with end-stage renal disease and the role of serum albumin. Cardiorenal Med 1(4): 255-260.
-
Gupta A, Kuldeep K, Virmani SK, Arora M (2017) Thyroid dysfunction in patients of chronic kidney disease. Int J Adv Med 4(5): 1333-1337.
-
Riniker M, Tieche M, Lupi GA, Grob P, Studer H, et al. (1981) Prevalence of various degrees of hypothyroidism among patients of general medical department. Clin Endocrinol 14(1): 69-74.
-
Schectman JM, Kallengerg GA, Shumacher RJ, Hirsch RP (1989) Yield of hypothyroidism in symptomatic primary care patients. Arch Intern Med 149(4): 861- 864.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance