Association of Angiotensin II Type I Receptor (AGTR1) Gene Polymorphism and Type 2 Diabetes & Nephropathy among the Eastern Indian Bengali Patients
Genetic polymorphisms of the angiotensin II type I receptor (AGTR1), has been reported to be the most probable candidate genes for hypertension, diabetes and complication of diabetes. Ethnic differences in the frequencies of these gene genotypes have also been reported. As there is no data available for AGTR1 polymorphism and T2DM in the Bengali population, it’s our attempt to fill the scientific gap. To investigate whether the angiotensin II type I receptor gene A1166C (rs5186) polymorphism is associated with a risk of type 2 diabetes and nephropathy in Indian Bengali patients, in a case-control study, the AGTR1 gene (rs5186; A1166C) was examined in type 2 diabetic patients with and without nephropathy (T2DM: N=246; T2DNH: N= 168) and normal control (N=304) participants and genotyped using PCR-RFLP methods. Result of Fisher exact test for allelic association of SNP rs5186 exhibits significant difference in the allele frequencies between the control and T2DM groups p= 0.0308). It is observed through the 4 genotypic model tests that additive model predicted significant association than basic genotype, dominant and recessive models and shows significant difference between CON vs. T2DM groups (p = 0.038). The present study reveals that the A1166C polymorphism (rs5186) of AGTR1 has a positive association with T2DM. This polymorphism with C allele may contribute to diabetic complication, nephropathy development particularly in T2DM patients.
Introduction
Type 2 Diabetes Mellitus (T2DM) constitutes the major mass of diabetes and India is the “Diabetes Capital of the World” with 69.2 million Indians having diabetes and with an estimated 72 million cases in 2017 [1, 2] with every fifth diabetic in the world being an Indian. Nephropathy is a complication of diabetes and is related to the damage or disease of kidney. Diabetic nephropathy is impairment to the kidney caused by the hyperglycemia and characterized by consistent proteinuria (>300 mg/ 24 h) convoyed by increased arterial blood pressure and steady decline in renal function. In severe cases kidney can be failure. The kidneys filter waste from blood through its capillaries. Diabetes result of high blood sugar can destroy these tiny blood vessels. Renal failure or kidney disease in diabetes is intervened by various biochemical pathways such as renin-angiotensin-aldosterone system (RAAS) [3, 4], aldose reductase-polyol [5], di-acyl glycerol-protein kinase C [6], hexosamine pathway [7] and advanced glycosylation end products (AGE) [8, 9]. The renin- angiotensin-aldosterone system (RAAS) actually provides a signal transduction mechanism for regulating body’s blood pressure and water balance. When an individual confronted with low blood pressure or certain nerve impulse such as stressful situation, the kidneys release an enzyme known as renin. This triggers a signal transduction pathway: renin cleaves the circulating protein angiotensinogen to produce angiotensin I, which is later converted to angiotensin II by another enzyme angiotensin converting enzyme (ACE). Angiotensin II causes blood vessels to compress, which results in high blood pressure. It also stimulates the secretion of the water retaining hormone vasopressin in the pituitary gland as well as the release of adrenaline, noradrenaline and aldosterone in the adrenal gland [10, 11, 12, 13].
The biological effects of angiotensin II are mediated via the angiotensin II receptor. By the help of ligand binding experiments two subtypes of cell surface receptors have been identified (AT1 & AT2) and are classified to the G-protein coupled receptor super family, which has seven transmembrane spanning domain[14]. In humans, the AT1 receptor is present predominantly in vascular smooth muscle cells, and the AT2 receptor is present in the uterus, brain and adrenal medulla [15, 16]. Both subtypes are also expressed in the adrenal cortex and kidney [17]. But most of the physiologic and pathphysiologic signals of Ang II, such as vasoconstriction, aldosterone release, stimulation of tubular transport, renal sodium reabsorption, proinflmmatory effects and growth stimulatory actions are transduced by AGTR1 receptors [18]. The AGTR1 gene extents >55 kilo bases (kb) on chromosome 3q22 and comprises of five exons, four of which are untranslated and alternatively spliced [19]. It has been found that AGTR1 is highly polymorphic [20, 21, 22, 23] but particularly rs5186 (A1166C) polymorphism of the AGTR1 gene, which was primarily identified by Bonnardeaux et al., a substitution of adenine (A) by cytosine (C) at position 1166, positioned at the 5’ end of the 3’ un-translated region of the gene, is the best evaluated [20] . Except this A1166C polymorphism, few other DNA polymorphisms have no significant impact on hypertension, diabetic nephropathy or myocardial infarction [20, 21, 22].
The renin-angiotensin-aldosterone system regulates not merely blood pressure but also the internal pressure of the glomerulus, and hypertension, which is an independent risk factor of diabetic nephropathy. The RAAS has been implicated in the pathogenesis of progressive renal disease [24, 25], diabetic renal complications [26] and seem to be especially relevant both biologically and clinically to renal disease [27, 28]. Therefore polymorphisms of RAAS candidate genes such as AGT, ACE, REN and AGTR1 are closely related to the progression of DN [13, 29, 30, 31, 32, 33]. Several studies suggest that the AGTR1 receptor might be involved in DN, type2 diabetes [21, 34, 35, 36], though many other investigator did not find any such relation between polymorphism of AGTR1 gene and diabetes as well as diabetic nephropathy [37, 38, 39]. Erstwhile we have identified that RAAS gene candidates ACE, AGT, CYP11B2, REN polymorphisms are significantly associated with type2 diabetes, hypertension, DN respectively, in eastern Indian Bengali population and western Indian Mewari population [13, 33, 40, 41].
Due to controversial results about the role of AGTR1 gene locus in diabetes, DN and the lack of information in this regard in Bengali population the aim of our present study was to scrutinize the role of AGTR1, in the development of DN in type 2 diabetes mellitus in Bengali population.
Materials and Methods
Study Patients
Recruitment of patients and study design describe elsewhere [13, 33]. Patients were recruited from registered patients list of two participating medical institutions of Kolkata city, West Bengal. A total of 718 age and sex matched individuals were participated in the present study, out of which 55.40% (n=398) male and 44.60% (n= 320) female. The study included 304 healthy control (CON: Male = 180; Female = 124), 246 type 2 diabetes patients without nephropathy (T2DM: Male = 128; Female = 118 )and 168 type 2 diabetic nephropathy patients on hemodialysis (T2DNH: Male = 90 ; Female = 78 ). The identification of Type 2 diabetic and nephropathy patients was based on physician’s recommendation or registered patient for dialysis. The unrelated controls were randomly selected and recruited from local community centres. A standardized protocol was implemented to obtain detailed medical history and data from each of the study participants. Ethical committee clearance was obtained from the medical institutions prior to the recruitment of subjects in this study. An informed consent was obtained from all the participants prior to their recruitment for the study.
Genotyping
Genomic DNA was prepared from fresh whole blood by using the conventional phenol-chloroform extraction method followed by ethanol precipitation [42]. DNA working dilutions (100μl) were prepared at a concentration of 50ng/ μl by dissolving required amount of stock DNA sample in TE buffer. After preparation of working dilutions the uniformity of the samples were checked by performing electrophoresis on a 1% agarose gel. In this study, previously published primers were used for the PCR based detections of SNPs [30, 40]. PCR amplification was performed in a final volume of 10μL reaction mixture containing 50ng of genomic DNA, 20 pmol of each primer, 10X Taq PCR buffer, 25 mM MgCl2, 100 mM of each dNTPs and 0.5 U/uL of Red Taq polymerase. PCR amplification was performed in a DNA thermo cycler (Bio- Rad). The DNA was amplified for 35 cycles with denaturation at 94°C for 1 min, annealing at 61°C for 1:30 min and extension at 72°C for 1:30 min and final extension 72°C for 10 min. The PCR products were checked by 2% agarose gel electrophoresis with ethidium bromide staining and directly visualized in UV light. Only those PCR products that had a single amplification product with no evidence of non-specific amplification were used for PCR-RFLP, details about the PCR- RFLP of AGTR1 gene described in our previous article [43].
Statistical Analysis
Allele frequencies were calculated for all the SNPs and were tested for Hardy-Weinberg equilibrium (HWE) and allelic association with the disease (Chi-Square test / Fisher exact test). Allelic and genotype association with the phenotypes was tested under different genetic models for both quantitative and qualitative traits by regression analysis and Fisher Model Test. Allele frequencies were calculated for the SNPs and tested for Hardy-Weinberg equilibrium (HWE) and allelic association with disease (Fisher exact test, logistic regression and Fisher model tests) using PLINK software [44]. For comparing the allelic distributions between study groups, the odds ratio (OR) with 95% confidence interval (CI) were also calculated. Quantitative data were analyzed using SPSS Version 16.0 (SPSS Inc., Chicago,IL, USA), were expressed as Mean ± SD and ANOVA test were used to determine differences in means and significance levels. A level of p <0.05 was assumed statistically significant.
Results
Genotype and Allele Frequency
Distribution of study groups based on genotype of AGTR1 gene polymorphism presented in Table 1. CC genotype were found among only 10 patients, out of which 8 patients are belongs to T2DM group and only 2 patients in T2DNH group.
The SNP rs5186 is an established polymorphism of the AGTR1 gene on chromosome 3: 148459988. It occurred in three forms, wild type homozygous AA, heterozygous AC and mutant homozygous CC (Figure 1). Genotype distribution of this polymorphism is presented in Table 2 and statistical analyses are given in Table 3 to Table 6. . The results of Hardy-Weinberg Equilibrium (HWE) test for rs5186 (A>C) of AGTR1 gene among the present study groups are presented in Table 3. From the HWE test it is found that the SNP rs5186 is not in Hardy-Weinberg equilibrium among T2D and T2DM groups, whereas Control and T2DNH groups maintain the Hardy-Weinberg Equilibrium.
Result of Fisher exact test for allelic association of SNPrs5186 (A>C) of AGTR1 gene among the study groups is presented in Table 4. The results exhibit no significant difference in the allele frequencies of the SNP between the control and T2D groups. However, significant differences are observed between CON vs. T2DM (χ2= 4.664, OR= 1.593, p= 0.0308) and T2DM vs. T2DNH (χ2= 3.967, OR= 0.5928, p=0.04639) groups.
The associations were further verified through 4 genotypic model tests (Fisher model test) to confirm which of these models predict best associations between the study groups and the results are presented in table 5. It is observed through the analyses that additive model predicted significant association than basic genotype, dominant and recessive models and shows significant difference between CON vs. T2DM groups (TREND, χ2 =4.269, p = 0.03882).
The mean values of quantitative variables, among study group based on AGTR1 gene genotype are presented in Table 6. The mean values of weight, BMI, triglyceride, total protein, globulin were significantly higher among the CC genotype group compared to AA and AC genotype groups of AGTR1 gene. The CC genotype individuals are relatively shorter while AA and AC genotype individuals are taller. Mean value of blood glucose comparatively higher among the CC genotype group, although not at significant level.
Comparison of Allele Frequency of AGTR1 Gene Variant Rs5186 with World Population
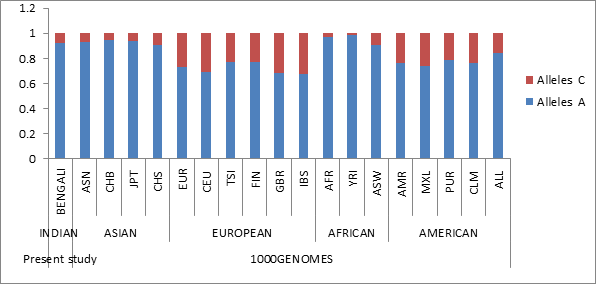
The allele frequency of the variant is calculated in the Indian Bengali population as well as in the World populations to check the utility of the SNP as a marker in our population as well as in the World populations (Table 7). The allele frequency of the rs5186 has been illustrated by the column graph in Figure 2. It is evident that the minor allele frequency is quite low in African population (YRI) where the ‘C’ allele shows a low frequency of 0.011, which is yielding a very low heterozygosity. The ancestral allele (A) frequency is quite high in all populations except in the European population and the lowest frequency among IBS population (0.679). Although European and American populations show quit higher frequency of minor allele, the two Mongoloid Asian populations CHB and JPT show similar profile, whereas the present study Indian Bengali population shows profile similar to the all Asian (ASN) and CHS populations.
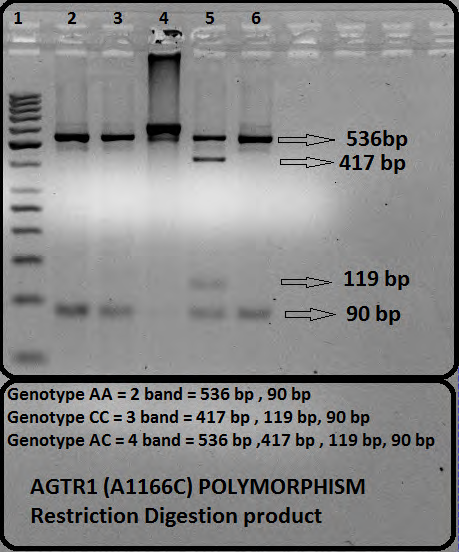
Figure 1: Ethedium bromide stained 2.5% agarose gel shows digested products for AGTR1 A1166C polymorphism(rs5186) by HpyF3I (DdeI) restriction enzyme . Fragments for allele ‘A’ = 536 bp and 90 bp ; allele ‘C ‘= 417 bp, 119 bp, and 90bp. Lane 1: DNA marker.; Lane 2,3,6 : Genotype AA : 2 Fragments of 536 bp and 90 bp ; Lane 4: Undigested PCR product ; Lane 5: Genotype AC : 4 fragments of 536 bp, 417 bp , 119 bp and 90 bp.
| AGTR1 Gene Polymorphismrs5186 (A1166C) Male Female | Sex | Total | |||||
|---|---|---|---|---|---|---|---|
| A A | Study Group | Control | Count | 154 | 108 | 262 | |
| % within Study Group | 58.8% | 41.2% | 100.0% | ||||
| T2DM | Count | 108 | 94 | 202 | |||
| % within Study Group | 53.5% | 46.5% | 100.0% | ||||
| T2DN | Count | 76 | 72 | 148 | |||
| % within Study Group | 51.4% | 48.6% | 100.0% | ||||
| Total % within Study Group | Count | 338 | 274 | 612 | |||
| 55.2% | 44.8% | 100.0% | |||||
| A C | Study Group | Control | Count | 26 | 16 | 42 | |
| % within Study Group | 61.9% | 38.1% | 100.0% | ||||
| T2DM | Count | 16 | 20 | 36 | |||
| % within Study Group | 44.4% | 55.6% | 100.0% | ||||
| T2DN | Count | 12 | 6 | 18 | |||
| % within Study Group | 66.7% | 33.3% | 100.0% | ||||
| Total % within Study Group | Count | 54 | 42 | 96 | |||
| 56.2% | 43.8% | 100.0% | |||||
| C C | Study Group | T2DM | Count | 4 | 4 | 8 | |
| % within Study Group | 50.0% | 50.0% | 100.0% | ||||
| T2DN | Count | 2 | 0 | 2 | |||
| % within Study Group | 100.0% | .0% | 100.0% | ||||
| Total % within Study Group | Count | 6 | 4 | 10 | |||
| 60.0% | 40.0% | 100.0% | |||||
| SNP | Genotype | Control | T2DM | T2DNH | |||
| N=304 | % | N=246 | % | N=168 | % | ||
| rs5186 | A A | 262 | 86.18 | 202 | 82.11 | 148 | 88.10 |
| A C | 42 | 13.82 | 36 | 14.63 | 18 | 10.71 | |
| C C | 0 | 0.00 | 8 | 3.25 | 2 | 1.19 |
Table 1: Sex wise distribution of study groups on the basis of AGTR1 Gene Polymorphism.
| SNP | Alleles | Study group | ObsHET | PredHET | HWpval | MAF |
|---|---|---|---|---|---|---|
| rs5186 | A:C | CON | 0.138 | 0.129 | 0.4369 | 0.069 |
| T2DM | 0.146 | 0.189 | 0.004* | 0.106 | ||
| T2DNH | 0.107 | 0.122 | 0.2876 | 0.065 |
Table 2: Hardy-Weinberg Equilibrium (HWE) test for rs5186 (A>C) of AGTR1 gene among the study groups.
*:Significant Table 3: Hardy-Weinberg Equilibrium (HWE) test for rs5186 (A>C) of AGTR1 gene among the study groups.
SNP A1 A2 Between Study group F_A F_U CHISQ P OR L95 U95
rs5186 C A
CON vs. T2DM 0.1057 0.0690 4.664 0.0308* 1.593 1.041 2.437
CON vs. T2DNH 0.0654 0.0690 0.0444 0.833 0.944 0.553 1.61
T2DM vs. T2DNH 0.0654 0.1057 3.967 0.0463* 0.592 0.352 0.996
- *;Significant
Table 3: Fisher exact test for allelic association of SNP rs5186 (A>C) of AGTR1 gene among the study groups.
| SNP | A1 | A2 | Between Study group | GENO | TREND | DOM | REC | |
|---|---|---|---|---|---|---|---|---|
| rs5186 | C | A | CONVs.T2DM | AFF | 8/36/202 | 52/440 | 44/202 | 8/238 |
| UNAFF | 0/42/262 | 42/566 | 42/262 | 0/304 | ||||
| CHISQ | NA | 4.26 | NA | NA | ||||
| p | NA | 0.04* | NA | NA | ||||
| CONVs.T2DNH | AFF | 2/18/148 | 22/314 | 20/148 | 2/166 | |||
| UNAFF | 0/42/262 | 42/566 | 42/262 | 0/304 | ||||
| CHISQ | NA | 0.0447 | NA | NA | ||||
| p | NA | 0.8326 | NA | NA | ||||
| T2DMVs.T2DNH | AFF | 2/18/148 | 22/314 | 20/148 | 2/166 | |||
| UNAFF | 8/36/202 | 52/440 | 44/202 | 8/238 | ||||
| CHISQ | NA | 3.31 | NA | NA | ||||
| p | NA | 0.06 | NA | NA |
Table 4: Fisher model test for SNP rs5186 of AGTR1 gene among the study groups.
*Significant Table 5: Fisher model test for SNP rs5186 of AGTR1 gene among the study groups.
| Quantitative variables | AGTR1 GENE POLYMORPHISM | ANOVA | |||
|---|---|---|---|---|---|
| AA (n=612) | AC (n=96) | CC (n=10) | F | Sig. | |
| Mean ± SD | Mean ± SD | Mean ± SD | |||
| Age (Years) | 54.91 ± 7.57 | 53.9 ± 7.099 | 55.8 ± 9.343 | 0.846 | 0.43 |
| Height (cm) | 160.47 ± 9.45 | 160.24 ± 10.29 | 157.72 ± 10.74 | 0.419 | 0.658 |
| Weight (kg) | 61.43 ± 12.31 | 61.18 ± 10.84 | 72.67 ± 15.75 | 4.245 | 0.015* |
| BMI (kg/m2) | 23.77 ± 3.83 | 23.85 ± 3.98 | 29.89 ± 8.910 | 11.787 | 0.000* |
| SBP(mmHg) | 134.87 ± 24.80 | 134.94 ± 23.15 | 138 ± 25.29 | 0.08 | 0.923 |
| DBP (mmHg) | 84.33 ± 11.53 | 86.73 ± 10.94 | 84.00 ± 8.43 | 1.852 | 0.158 |
| Glucose (mg/dl) | 130.23 ± 53.986 | 126.58 ± 36.089 | 131.2 ± 38.142 | 0.209 | 0.811 |
| Cholesterol (mg/dl) | 176.10 ± 39.95 | 183.37 ± 33.14 | 164.27 ± 24.15 | 1.984 | 0.138 |
| Triglyceride (mg/dl) | 160.89 ± 76.39 | 180.83 ± 84.11 | 200.16 ± 64.21 | 3.857 | 0.022* |
| Creatinine (mg/dl) | 2.33 ± 2.31 | 2.07 ± 2.00 | 2.11 ± 1.88 | 0.544 | 0.581 |
| Total Protein (g/dl) | 7.55 ± 0.96 | 7.67 ± 1.18 | 8.76 ± 0.86 | 7.747 | 0.000* |
| Albumin (g/dl) | 4.21 ± 0.69 | 4.25 ± 0.69 | 4.62 ± 0.33 | 1.91 | 0.149 |
| Globulin (g/dl) | 3.34 ± 0.81 | 3.41 ± 0.81 | 4.14 ± 0.94 | 5.043 | 0.007* |
Table 5: Comparison of mean values of different quantitative variables among the study groups based on genotype of AGTR1 gene pol
*Significant Table 6: Comparison of mean values of different quantitative variables among the study groups based on genotype of AGTR1 gene polymorphism.
| POPULATION | Alleles A | Alleles C | ||
|---|---|---|---|---|
| PRESENT STUDY | INDIAN | BENGALEE | 0.919 | 0.081 |
| 1000GENOMES | ASIAN | ASN | 0.93 | 0.07 |
| CHB | 0.948 | 0.052 | ||
| JPT | 0.938 | 0.062 | ||
| CHS | 0.905 | 0.095 | ||
| EUROPEAN | EUR | 0.728 | 0.272 | |
| CEU | 0.694 | 0.306 | ||
| TSI | 0.77 | 0.23 | ||
| FIN | 0.769 | 0.231 | ||
| GBR | 0.68 | 0.32 | ||
| IBS | 0.679 | 0.321 | ||
| AFRICAN | AFR | 0.974 | 0.026 | |
| YRI | 0.989 | 0.011 | ||
| ASW | 0.91 | 0.09 | ||
| AMERICAN | AMR | 0.765 | 0.235 | |
| MXL | 0.742 | 0.258 | ||
| PUR | 0.791 | 0.209 | ||
| CLM | 0.767 | 0.233 |
Table 6: Allele frequencies of AGTR1 gene variant rs5186 in present study groups and World population (1000 GENOME PROJECT) [45].
Discussion
Insensitivity to insulin or type2 diabetes is diligently associated to the metabolic syndrome [45, 46], and the RAAS have a pivotal role in the insulin sensitivity [47, 48, 49] as well as in the regulation of blood pressure, maintaining stable equilibrium of sodium ion and extracellular fluid volume [50, 51].
In our preceding work we have found that RAAS polymorphisms are genetically susceptible for hypertension, and renal complication associated with diabetes [13, 32, 33, 41]. Though various studies have found the association of RAAS variants with hypertension [52, 53, 54, 55, 56], atherosclerosis [57], progression of renal disease [35, 53, 58], diabetic nephropathy 29], the relevance of RAAS polymorphism regarding insulin resistance yet has not been fully illuminated. Polymorphisms of different candidate of the RAAS i.e. REN, ACE, AGT, AGTR1 have been explained with controversial results [21, 34, 35, 36, 37, 38, 39, 59, 60] mainly elucidated by the diverse ethnic backgrounds of the study population.
Out of several single nucleotide polymorphisms within the AGTR1 gene, the best evaluated polymorphism is rs5186 (A1166C) where nucleotide Adenine (A) is substituted by Cytosine (C). The A allele devoid of restriction enzyme site (DdeI) therefore produce larger fragment, whereas the C allele carries the enzyme-restriction site at nucleotide position 1166, therefore produce smaller fragment [54]. This rs5186 (A1166C) polymorphism of the AGTR1 gene was reported to be associated with a number of cardiovascular outcomes [61, 62, 63, 64], essential hypertension [20, 65, 66], and has been proposed as a predictor of renal injury in T2DM [21]. The C allele (either in homozygous CC or heterozygous AC) carrying Type 2 diabetes patients showed rapid deterioration of renal function than those with the AA genotype and this was confirmed in a later study which showed that the A1166C polymorphism was associated with the development of renal disease and progression to end-stage renal failure [67, 68, 69]. A previous study reported that the A1166C polymorphism may contribute to nephropathy development, particularly in T2DM patients and the homozygote variant genotypes (CC) for the risk of DN [70]. Although a recent Japanese study reported that the impact of C allele on progression of DN in a small number of Japanese women T2DM patients [34]. However, a study from china reported that AGTR1 is not a contributing factor for DN in T2DM patient in Chinese population [71].
The result of our study have replicate findings of previous studies who have reported synergistic effect between the AGTR1 C1166 allele and poor glycemic control on risk of developing nephropathy in type 2 diabetic patients. The present study also reveals that the AGTR1 A1166C polymorphism has a positive association with T2DM (OR =1.593, p < 0.05). This polymorphism with C allele may contribute to diabetic nephropathy development particularly in T2DM patients and this result is in agreement with previous meta-analysis study [70].
Previously it was considered, the RAAS as an endocrine system resulting in the production of angiotensinogen in the liver, which is split by renin released from the renal juxtaglomerular cells [72]. But over the past three decades several studies revealed that local RAAS independently operate from their systemic counterpart [73]. A local RAAS along with its all the members present in the proximal tubular cells of the kidney. Angiotensin II actively produced from the proximal tubular cell, which also secretes angiotensinogen into the urine [73]. Intraluminal angiotensinogen perhaps converted to Ang II in the distal tubules, which leads to the stimulation of sodium channels independent of aldosterone [74]. Poor glycemic control and abnormal quantities of protein in urine could stimulate the synthesis of local Ang II mainly by oxygen species as signal transducers [17]. AGTR1 expression is induced by various stimuli, but down regulated by high conc. of Ang II [17], a feedback mechanism of gene regulation. Now the polymorphic AGTR1 may be insensitive to this down regulation by Ang II and therefore predisposed to renal dysfunction in hyperglycemic condition. It is beyond our scope to investigate this idea, but one can design an experimental set up to explore any such contribution of AGTR1 gene polymorphism to the renal dysfunction in individual who is suffering from poor glycemic control.
Conclusion
To expose a particular disease and also to identify its tendency within a particular population in a particular ethnic background, the delineation of the responsible functional genes of the genome is of great importance which eventually be of support to the doctors for recommending personalized medicine.
The study reveals that the AGTR1 A1166C polymorphism has a positive association with T2DM and C allele may contribute to diabetic nephropathy development particularly in T2DM patients of Bengali population of Eastern India. The present study has to be taken under consideration within its limitations, that it was limited to a specific ethnic group (Eastern Indian Bengali population). The CC genotype individual are relatively shorter and shows higher mean values of weight, BMI, triglyceride, total protein, globulin compared to AA and AC genotype groups. A larger study from different ethnic groups will be needed to confirm for any contribution of AGTR1 gene polymorphism to T2DM complications for development of renal problem or nephropathy. It is to mention here that this research work only deals with the association study (irrespective of gender) between diabetic nephropathy and the genetic variation of AGTR1 gene within its 5’ end of the 3’-untranslated region.
Acknowledgement
We would like to thank the members of the study populations, patients and control participants for voluntarily taking part in this research work and donating their blood samples and cooperation during data collection. We wish to express our deep gratitude to the Director, Anthropological Survey of India, for his kind permission to initiate the work and also for providing financial support.
Funding
This study was funded by the Anthropological Survey of India (Fellowship to Dr. Pulakes Purkait as Junior Research Fellowship and Senior Research Fellowship).
Availability of Data Materials: Although the study is not a clinical trial, it is a genetic study. All data submitted to the Anthropological survey of India.
Conflicts of Interest
The authors declare that they have no competing interests.
Consent for Publication
Although the manuscript does not involve the use of live photographs of any of the participants, consent was obtained from them for the data to be published as at the time recruitment into the study.
Ethics Approval and Consent to Participate
Ethical committee clearance was obtained from the respective medical institutions and Ethical committee of the Anthropological Survey of India, Govt. of India.. Verbal and written well informed consent was obtained from all participants before they were eligible for recruitment into the study.
Authors’ Contributions
PP was involved in the experiments, screening for gene mutations, performed the statistical analysis as well as participating in the write up of the manuscript; KH contributed to preparation of the manuscript. All authors read and approved the final manuscript.
References
-
International Diabetes Federation (2015) IDF Diabetes Atlas- 7th (Edn.), Diabetes Atlas.
-
Zheng Y, Ley SH, Hu FB (2018) Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nature Reviews Endocrinology 14(2): 88-98.
-
Ruggenenti P, Craverdi P, Remuzzi G (2010) The RAAS in the pathogenesis and treatment of diabetic nephropathy. Nature Rev Nephrol 6(6): 319-330.
-
Chawla T, Sharma D, Sing A (2010) Role of renin angiotensin system in diabetic nephropathy. World Journal of Diabetes 1(5): 141-145.
-
Dunlop M (2000) Aldose reductase and the role of polyol pathway in diabetic nephropathy. Kidney Int 58(S77): S3-S12.
-
Noh H, King GL (2007) The role of protein kinase C activation in diabetic nephropathy. Kidney Int 106: S49-S53.
-
Schleicher ED, Weigert C (2000) Role of hexosamine biosynthetic pathwayin diabetic nephropathy. Kidney Int 58(S77): S13-S18.
-
Forbes JM, Cooper ME, Oldfield MD, Thomas MC (2003) Role of advanced glycation end products in diabetic nephropathy. J Am Soc Nephrol 14(S8): S254-S258.
-
Buse MG (2006) Hexosamines, insulin resistance and complications of diabetes: current status. Am J Physiol Endocrinol Metab 290(1): E1-E8.
-
Remuzzi G, Pinares F, Bettinaglio P, Ruggenenti P (2008) Angiotensin Converting Enzyme Insertion/Deletion Polymorphism and Renoprotection in Diabetic and Nondiabetic Nephropathies. Clin J Am Soc 3(5): 1511- 1525.
-
Wang F, Fang Q, Yu N, Zhao D, Zhang Y, et al. (2012) Association between genetic polymorphism of the angiotensin converting enzyme+e and diabetic nephropathy: a meta-analysis comprising 26,580 subjects. J of Renin-Angiotensin-Aldosterone Syst 13(1): 161-174.
-
Felehgari V, Hasanvand A, Rahimi Z (2012) Interaction of MTHFR 1298C with ACE D allele augments the risk of diabetic nephropathy in Western Iran. DNA Cell Biol 31(4): 553-559.
-
Purkait P, Halder K, Naidu J, Sarkar B (2018) Genetic variants of Renin on the prevalence of diabetic nephropathy. Vessel Plus 2(19): 1-10.
-
Guo DF, Sun YL, Hamet P, Inagami T (2001) The angiotensin II type 1 receptor and receptor –associated proteins. Cell Res 11(3): 165-180.
-
Curnow KM, Pascoe L, Davies E, White PC, Corvol P, et al. (1995) Alternatively spliced human type 1 angiotensin receptor mRNAs are translated at different efficiencies and encode two receptor isoforms. Mol Endocrino 9(9): 1250-1262.
-
Martin MM, Willardson BM, Burton GF, White CR, McLaughlin JN, et al. (2001) Human angiotensin II type 1 receptor isoform encoded by mRNA splice variants are functionally distinct. Mol Endocrinol 15(2): 281-293.
-
Wolf G, Butzmann U, Wenzel UO (2003) The renin- angiotensin system and progression of renal disease: From hemodynamics to cell biology. Nephron Physiol 93(1): P3-P13.
-
Ruster C, Wolf G (2006) Renin-angiotensin-aldosterone system and progression of renal disease. J Am SocNephrol 17(11): 2985-2991.
-
Curnow KM, Pascoe L, White PC (1992) Genetic analysis of the human type-1 angiotensin II receptor. Mol Endocrinol 6(7): 1113-1118.
-
Bonnardeaux A, Davies E, Jeunemaitre X, Féry I, Charru A, et al. (1994) Angiotensin II type 1 receptor gene polymorphisms in human essential hypertension. Hypertension 24(1): 63-69.
-
Doria A, Onuma T, Warram JH, Krolewski AS (1997) Synergistic effect of angiotensin II type 1 receptor genotype and poor glycemic control on risk of nephropathy in IDDM. Diabetologia 40(11): 1293-1299.
-
Poirier O, Georges JL, Ricard S, Arveiler D, Ruidavets JB, et al. (1998) New polymorphisms of the angiotensin II type 1 receptor gene and their associations with myocardial infarction and blood pressure: the ECTIM study. Etude Cas-Témoin de l’Infarctus du Myocarde. J Hypertens 16(10): 1443-1447.
-
Erdmann J, Riedel K, Rohde K, Folgmann I, Wienker T, et al. (1999) Characterization of polymorphisms in the promoter of the human angiotensin II subtype 1 (AT1) receptor gene. Ann Hum Genet 63(Pt 4): 369-374.
-
Schmidt S, Ritz E (1997) Genetics of the renin-angiotensin system and renal disease: a progress report. Curr Opin Nephrol Hypertens 6(2): 146-151.
-
Lee KB, Kim UK (2003) Angiotensin and Angiotensin II type 1 receptor gene polymorphism in patients with autosomal dominant polycystic kidney disease: Effect on hypertension and ESRD. Yonsei Med J 44(4): 641-647.
-
Harrison-Bernard LM (2009) The renal renin- angiotensin system. Adv Physiol Educ 33(4): 270-274.
-
Gumprecht J, Zychma MJ, Grzeszczak W, Zukowska- Szczechowska E (2000) Angiotensin-I-converting enzyme gene insertion/deletion and angiotensinogen M235T polymorphisms: Risk of chronic renal failure. End- Stage Renal Disease Study Group. Kidney Int 58(2): 513-519.
-
Lovati E, Richard A, Frey BM, Frey FJ, Ferrari P (2001) Genetic polymorphisms of the renin-angiotensin- aldosterone system in end-stage renal disease. Kidney Int 60(1): 46-54.
-
Viswanathan V, Zhu Y, Bala K, Dunn S, Snehalatha C, et al. (2001) Association between ACE gene polymorphism and diabeticnephropathy in South Indian patients. J Pancreas 2(2): 83-87.
-
Prasad P, Tiwari AK, Prasanna KM, Ammini AC, Gupta A, et al. (2006) Cronicrenal insuffiency among Asian Indians with type 2 diabetes: I. Role of RASSgene polymorphisms. BMC Med Genet 7: 42.
-
Purkait P, Raychodhury P, Bandhyopadhya S, Naidu JM, Sarkar BN (2013a) Analysis of Aldosterone Synthase Gene Promoter (- 344 C >T) Polymorphism in Indian Diabetic Nephropathy Patients. J Diabetes Metab 4(5): 271.
-
Purkait P, Halder K, Ghosh Roy A, Venugopal PN, et al. (2015c) A comparative study of _angiotensin converting_ _enzyme_ (ACE) gene polymorphism of bengali and mewari type 2 diabetes patients in India. J Harmoniz Res Appl Sci 3(1): 01-09.
-
Purkait P, Halder K, Thakur S, Ghosh Roy A, Raychaudhuri P, et al. (2017) Association of angiotensinogen gene SNPs and haplotypes with risk of hypertension in eastern Indian population. Clinical Hypertension 23: 12.
-
Tomino Y, Makita Y, Shike T, Gohda T, Haneda M, et al. (1999) Relationship between polymorphism in the angiotensinogen, angiotensin converting enzyme or angiotensin II receptor and renal progression in japanese NIDDM patients. Nephron 82(2): 139-144.
-
Jacobsen P, Tarnow L, Carstesen B, Hovind P, Poirrier O, et al. (2003) Genetic variation in the renin-angiotensin system and progression of diabetic nephropathy. J Am Soc Nephrol 14(11): 2843-2850.
-
Akasaka H, Katsuya T, Saitoh S, Sugimoto K, Fu Y, et al. (2006) Effects of angiotensin II type 1 receptor gene polymorphisms on insulin resistance in a Japanese general population: Thr Tanno-Sobetsu study. Hypertens Res 29(12): 961-967.
-
Tarnow L, Cambien F, Rossing P, Neilson FS, Hansen BV, et al. (1996) Angiotensin II type 1 receptor gene polymorphism and diabetic microangiopathy. Nephrol Dial Transplant 11(6): 1019-1023.
-
Chowdhury TA, Dyer PH, Kumar S, Gough SC, Gibson SP, et al. (1997) Lack of association of the angiotensin II type 1 receptor gene polymorphism with diabetic nephropathy in insulin-depenent diabetes mellitus. Diabetes Med 14(10): 837-840.
-
Savage DA, Feeney SA, Fogarty DG, Maxwell AP (1999) Risk of developing diabetic nephropathy is not associate with synergism between the angiotensin II (type 1) receptor C1166 allele and poor glycemic control. Nephrol Dial Transplant 14(4): 891-894.
-
Purkait P, Suthar PC, Purohit VK, Naidu JM, Sarkar BN (2013b) Renin- Angiotensin- Aldosterone System gene polymorphisms in Type 2 Diabetic patients among the Mewari population of Rajasthan. Int J Biol Med Res 4(2): 3128-3134.
-
Purkait P, Roy AG, Halder K, Suthar PC, Raychaudhuri P, et al. (2015b) Sex-based Association of _CYP11B2_ (-344 C/T) Polymorphism in Indian Type 2 Diabetic Patients. Int J DiabetolVasc Dis Res 3(4) 89-93.
-
Miller SA, Dykes DD, Polesky HF (1998) A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acid Res 16(3): 12-15.
-
Purkait P, Gandharve LK, Purohit VK, Naidu JM, Sarkar BN (2013c) Gender based association between _ACE_ gene(I/D) polymorphism and Type 2 Diabetic Mewari patients of Udaipur city, Rajasthan. Jr Anth Survey of India 62(2): 169-177.
-
Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MA, et al. (2007) PLINK: a toolset for whole-genome association and population-based linkage analysis. Am J Hum Genet 81(3): 559-575.
-
Cheal KL, Abbasi F, Lamendola C, McLaughlin T, Reaven GM, et al. (2004) Relationship to insulin resistance of the adult treatment panel III diagnostic criteria for identification of the metabolic syndrome. Diabetes 53(5): 1195-1200.
-
Reaven GM (1995) Pathophysiology of insulin resistance in human disease. Physiol Rev 75(3): 473-486.
-
Higashirua K, Ura N, Takada T, Li Y, Torii T, et al. (2000) The effects of an angiotensin-converting enzyme inhibitor and an angiotensin II receptor antagonist on insulin resistance in fructose fed rats. Am J Hypertens 13(3): 290-297.
-
Ura N, Higashiura K, Shimamoto K (1999) The mechanisms of insulin sensitivity improving effects of angiotensin- converting enzyme inhibitor. Immunopharmacology 44(1-2): 153-159.
-
O’Donnell CJ, Lindpaintner K, Larson MG, Rao VS, Ordovas JM, et al. (1998) Evidence for association and genetic linkage of the angiotensin-converting enzyme locus with hypertension and blood pressure in men but not women in the Framingham Heart Study. Circulation 97(18): 1766-1772.
-
Manrique C, Lastra G, Gardner M, Sowers JR (2009) The renin angiotensin aldosterone system in hypertension: roles of insulin resistance and oxidative stress. Med Clin North Am 93(3): 569-582.
-
Glosnicka KN, Lacka BI, Zychma MJ, Grzeszczak W, Szczechowska EZ, et al. (2000) Angiotensin II type 1 receptor gene A1166C polymorphism is associated with the increased risk of pregnancy-induced hypertension. Med Sci Monit 6(3): 523-529.
-
Kim UK, Lee KB (2003) Angiotensin and angiotensin II type 1 receptor gene polymorphism in patients with autosomal dominant polycystic kidney disese: Effect of hypertension and ESRD. Yonsei Med J 44(4): 641-647.
-
Baudin B (2004) Polymorphism in angiotensin II receptor genes and hypertension. Exp Physiol 90(3): 277-282.
-
Freitas SRS, Cabello PH, Moura-Neto RS, Dolinsky LC, Lima AB, et al. (2006) Analysis of renin-angiotensin- aldosterone system gene polymorphisms in resistant hypertension. Brazilian journal of Medical and Biological Research 40(3): 309-316.
-
Behravan J, Naghibi M, Mazloomi MA, Hassany M (2006) Polymorphism of angiotensin type II receptor gene in essential hypertension in Iranian population. DARU Journal of Pharmaceutical Sciences 14(2): 82-86.
-
Kretowski A, McFann K, Hokanson JE, Maahs D, Kinney G, et al. (2007) Polymorphisms of the renin-angiotensin system genes predict progression of subclinical coronary atherosclerosis. Diabetes 56(3): 863-871.
-
Campbell CY, Fang BF, Guo X, Peralta CA, Psaty BM, et al. (2010) Association between genetic variants in the _ACE_, _AGT_, _AGTR1_, and _AGTR2_ genes and renal function in the multi-ethnic study of atherosclerosis. Am J Nephrol 32(2): 156-162.
-
Jardine AG, Padmanabhan N, Connell JM (1998) Angiotensin converting enzyme gene polymorphisms and renal disease. Curr Opin Nephrol Hypertens 7(3): 259-264.
-
Dostal DE, Baker KM (1992) Angiotensin II stimulation of left ventricular hypertrophy in adult rat heart. Meditation by AT1 receptor. Am J Hypertens 5(5): 276- 280.
-
Ortlepp JR, Vosberg HP, Reith S, Ohme F, Mahon NG, et al. (2002) Genetic polymorphisms in the renin-angiotensin- aldosterone system associated with expression of left ventricular hypertrophy in hypertrophic cardiomyopathy: a study of five polymorphic genes in a family with a disease causing mutation in the myosin binding protein C gene. Heart 87(3):270-275.
-
Denus SD, Zakrzewski-Jakubiak M, Dubé MP, Bélanger F, Lepage S, et al. (2008) Effects of AGTR1 A1166C gene polymorphism in patients with heart failure treated with candesartan. Annals of pharmacotherapy 42(7-8): 925- 932.
-
Coto E, Palacín M, Martín M, Castro MG, Reguero JR, et al. (2001) Functional polymorphisms in genes of the Angiotensin and Serotonin systems and risk of hypertrophic cardiomyopathy: AT1R as a potential modifier. Journal of translational medicine 8(1): 64.
-
Xu M, Sham P, Ye Z, Lindpaintner K, He L (2010) A1166C genetic variation of the angiotensin II type I receptor gene and susceptibility to coronary heart disease: collaborative of 53 studies with 20,435 cases and 23,674 controls. Atherosclerosis 213(1): 191-199.
-
Makeeva OA, Puzyrev KV, Pavlyukova EN, Koshelskaya OA, Golubenko MV, et al. (2004) ACE and AGTR1 polymorphisms in pathogenesis of human left ventricular hypertrophy. Molecular Biology 38(6): 844-849.
-
Mahmoud Y, Badwy MD, Othman AN, Zalata GA, Aziz AA (2009) Renin Angiotensin System Genotypes and Oxidized LDL in Hypertensive Egyptian Patients. The Egyptian Society of Cardiology Board of Directors.
-
Buraczynska M, Ksiazek P, Zaluska W, Spasiewicz D, Nowicka T, et al. (2002) Angiotensin II type 1 receptor gene polymorphism in end-stage renal disease. Nephron 92(1): 51-55.
-
Buraczynska M, Ksiazek P, Drop A, Zaluska W, Spasiewicz D, et al. (2005) Genetic polymorphisms of the reninangiotensin system in end-stage renal disease. Nephrol Dial Transplant 21(4):979-983.
-
Lin J, Hu FB, Qi L and Curhan GC (2009) Genetic polymorphisms of angiotensin-2 type 1 receptor and angiotensinogen and risk of renal dysfunction and coronary heart disease in type 2 diabetes mellitus. BMC Nephrol 10: 9.
-
Ding W, Wang F, Fang Q, Zhang M, Chen J, et al. (2012) Association between two genetic polymorphisms of the renin-angiotensin-aldosterone system and diabetic nephropathy: a meta-analysis. Molecular biology reports 39(2): 1293-1303.
-
Songhua WU, Kunsan X, Taishan Z (2000) Association study of three key genes of renin-angiotensin system in the patients of type 2 diabetes with nephropathy. Chinese Journal of Endocrinology and Metabolism.
-
Wolf G, Neilson EG (1996) From converting enzyme inhibition to angiotensin II receptor blockade: New insights on angiotensin II receptor subtypes in the kidney. Exp Nephrol 4(S1): 8-19.
-
Nishiyama A, Seth DM, Navar LG (2002) Renal interstitial fluid concentrations of angiotensins I and II in anesthetized rats. Hypertension 39(1): 129-134.
-
Beutler KT, Masilamani S, Turban S, Nielsen J, Brooks HL, Ageloff S, et al. (2003) Long-term regulation of ENaC expression in kidney by angiotensin II. Hypertension 41(15): 1143-1150.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance