A Preliminary Predictive Model of Post-Transplant Tumor Recurrence in Hepatitis B Virus Associated Hepatocellular Carcinoma-Epidemiological and Therapeutic Implications
Background: Hepatocellular carcinoma (HCC) is one of the most aggressive malignancies worldwide with hepatitis B virus (HBV) as the most important etiological agent. Unfortunately, the outcome of medical management of HBV related HCC is abysmal and post-transplant tumor recurrence represents a major challenge. However, a robust clinical predictor of disease recurrence in HBV mediated HCC is yet to be established despite several evidences illustrating multiple causative factors. Aim: Here we report a preliminary model that predicted the probability of post-transplant tumor recurrence in patients presenting with HBV related HCC and opting for living donor liver transplantation (LDLT). Methods: Our study prospectively recruited 67 quantitative HBV DNA positive HCC patients and 71 quantitative HBV DNA negative HCC patients, all with documented evidences of chronic HBV infection. A linear model analysis based on minimum Akaike’s Information Criterion (AIC) values was computed. This generated a statistical inference about the causal relationship between different pre- and post-transplant clinicopathological variables of the study population and pre-transplant tumor recurrence of HBV related HCC. Additionally, a Cox's proportional hazard modeling showing independent predictors of post transplant tumor recurrence was also illustrated. Results: Several combinations of linear models were assessed and significant parameters like age (b=0.06, p=0.02), alpha-fetoprotein (b=0.02, p=0.01) levels, HBV DNA (b=0.05, p=0.03) levels, total tumor burden (b=0.08, p=<0.001) and Model for End-Stage Liver Disease (MELD) score (b=0.07, p=0.04) predicted probability of post-transplant tumor recurrence. Multivariable analysis through Cox proportional hazard modeling further depicted HBV DNA and AFP levels as predictors of post transplant tumor recurrence in HBV related HCC. Additionally, a novel algorithm proposed a differentiation of patients opting for living donor liver transplantation (LDLT) into low, intermediate and high risk categories for developing recurrence of the disease. Conclusions: The outcome of our study might facilitate improved prognostication, risk stratification and better clinical management of patients with HBV related HCC.
Introduction
Hepatocellular carcinoma (HCC) is the 5th most common primary liver malignancy and 2nd commonest cause of cancer-related deaths worldwide, with ~695,900 deaths being recorded annually [1]. Infection with hepatitis B virus (HBV) has been documented as the most common etiological factor [2]. Surgical treatment strategies including liver resection and liver transplantation, although underutilized, are considered potentially curative. However, post surgical tumor recurrence rates of ~30-50% continue to jeopardize long- term disease-free survival in patients [3, 4, 5]. Causative factors implicated in recurrence of HBV related HCC are HBeAg status, HBV-BCP mutations, HBV DNA viral load (by far considered as the most critical component), tumor size, tumor stage, alpha-fetoprotein levels and presence of cirrhosis. Attributes independently associated with HBV recurrence post transplantation have also been adequately defined [6, 7, 8]. Recently researchers have opined that long non-coding RNA PVT1 is associated with tumor progression and is a significant predictor of recurrence in liver cancer patients [9]. Contrarily, reports indicate that in patients with NBNC-HCC profile (patients with HCC in absence of both hepatitis B virus surface antigen, HBsAg and hepatitis C virus antibody, HCVAb), elevated serum bilirubin could predict poor recurrence- free survival after surgery [10]. Studies have also revealed low serum IL-6 level to be an independent prognostic factor for disease-free survival together with low platelet count and low serum albumin level, in patients with HBV- related early HCC who underwent hepatic resection or radiofrequency ablation with a curative intent [11]. Furthermore, data also display an up regulation of heat shock proteins HSPA12A, HSP90B1, HSPA4, HSPA5 and HSPA6 in tumor tissues to be significantly associated with poor outcomes from HBV-related early-stage HCC [12]. Till date, however, there are limited strategies to predict recurrence of HBV related HCC following liver transplantation. Majority of studies have illustrated several attributes for recurrence of HBV related HCC singly or in combination that fails to predict the probability of recurrence. In the above backdrop, our study aimed at creating a preliminary model to putatively predict the probability of post-transplant tumor recurrence of HBV related HCC. In addition, our study also depicts a novel algorithm that differentiates patients opting for living donor liver transplantation (LDLT) into low, intermediate and high risk categories for developing recurrence of the disease which might facilitate improved prognostication, better patient selection for transplant services and tailoring of post-operative management to suit individual patients in various risk categories.
Methods
Study population
A total of 138 patients presenting with HBV related HCC and opting for LDLT were prospectively recruited from the Centre for Liver and Biliary Surgery, Indraprastha Apollo Hospital, New Delhi, with written informed consent from May 2014 to May 2017. The study protocol conformed to the provisions of the 1975 Declaration of Helsinki (as revised in Seoul, Korea, October 2008) and was approved and acquitted by the Institutional Ethical Clearance Committee of Jamia Millia Islamia. In this study, HCC patients presenting with underlying cirrhosis and documented evidence of chronic HBV infection who attained negative quantitative HBV DNA levels before transplant, comprised Group 1 (n=71) patients. On the other hand, HCC patients presenting with underlying cirrhosis, documented evidence of chronic HBV infection and high positive quantitative HBV DNA levels before transplant, were included as Group 2 (n=67) patients, in our study. The diagnostic criteria for the selection of HCC patients were followed as described elsewhere [13]. To confirm whether all patients had chronic HBV infection (CHB) for a period of at least 6 months, hepatitis B surface antigen (HBsAg), hepatitis B virus core antibody and hepatitis B e-antigen or hepatitis B e-antibody were confirmed as seropositive. CHB was further diagnosed with serum HBV-DNA levels >1,000 copies/mL, as well as elevated alanine aminotransferase (ALT) or aspartate aminotransferase levels (AST) (>2 times the upper limit of normal) [14]. HCC patients co- infected with HBV/HCV and/or HBV/HIV, without documented evidence of chronic HBV infection, with a history of alcohol consumption and those on hepatotoxic drugs (e.g. acetaminophen >3 grams/day for >30 days or >7 grams/day at any point of time) were not included in our study. Additionally, patients with psychiatric illnesses who were unable to provide informed consent were also excluded from this study.
Collection of Clinicopathological Variables
Patient proforma for recording clinical data and patient consent form for obtaining written informed consent were maintained for every patient throughout the course of the investigation. Data on the date of diagnosis, age, sex, status of HBV serological markers and HBV genotypes, details of hematological and biochemical investigations in addition to Child-Pugh-Turcotte (CPT) score and class and Model for End-Stage Liver Disease (MELD) score for LDLT with regard to HCC patients were abstracted from the medical records of every patient. For the purpose of this study, the MELD score was calculated without any exception points. At the time of recruitment, each patient was personally interviewed to ascertain information on his/her socio-demographic characteristics, ethnicity, lifestyle, lifetime history of cigarette smoking, tobacco and alcohol consumption, dietary factors in addition to personal and family history of various chronic diseases followed by standardized clinical examination. The cumulative exposure to cigarettes was calculated as pack-years. Additionally, history of exposure to blood and blood products, transfusion procedures, HBV vaccination, exposure to chemicals, family history of cirrhosis or any other member being positive for HBV infection were also recorded. Furthermore, post surgical details on tumor differentiation, number and size of tumor nodules together with the total tumor burden were also recorded for the cases. The total tumor burden in cases was further classified as within (≤8 cm) and beyond (>8 cm) the University of California San Francisco (UCSF) criteria. Recurrence and mortality data were followed up after a median one year (365 days) of surgery (living donor liver transplantation).
Linear Modeling (LM)
In this study, a generalized linear regression analysis was performed using recurrence as the dependent variable and various components of pre-transplant and post-transplant characteristics of the study population as covariates. The results were utilized to develop a model that predicted the probability of post-transplant tumor recurrence of HBV related HCC. The goodness of fit of the models was achieved through minimum Akaike’s Information Criterion (AIC) values.
Multivariable Cox-proportional Hazard Modeling
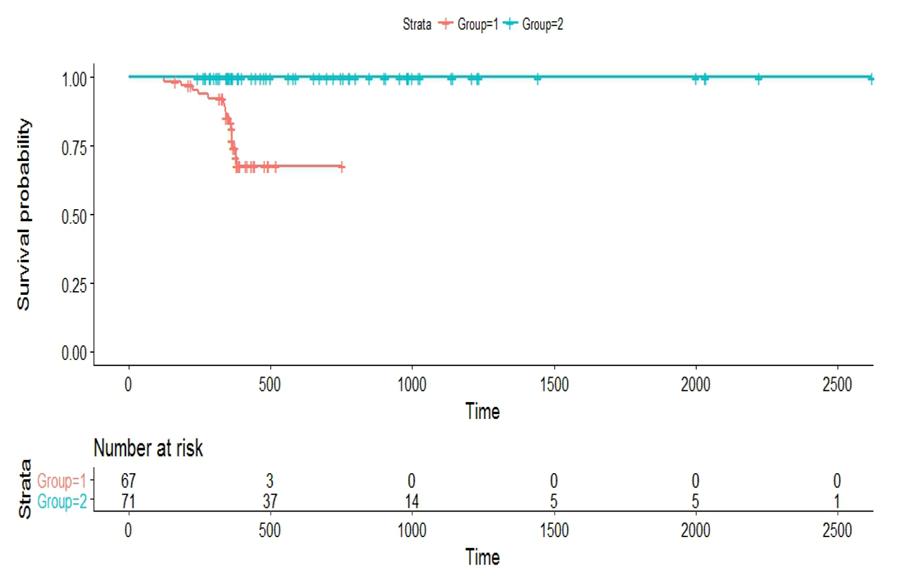
A multivariable Cox's proportional hazard modeling showing independent predictors of post transplant tumor recurrence and a survival analysis taking Group 1 & 2 into consideration was performed through Kaplan-Meier survival curves.
Statistical Analysis
hazard modeling. For the purpose of this study, data were normalized using log10 transformation wherever required. A two-tailed probability level of p<0.05 was considered statistically significant.
Results
- Baseline Characteristics of the Study Population
- The baseline characteristics of the study population are described in Table 1.
- HBV related HCC obtained with respect to pre- and posttransplant HBV DNA and AFP levels is illustrated in Table
- 2.
- Profile of Follow-up and Recurrence of HBV
- Related HCC in the Study Population
- Post-surgical follow-up of patients and recurrence of
- Group
- Mean follow-
- Recurrence (No.
- HBV DNA levels
- HBV DNA levels post recurrence
- AFP levels preup (in days) of patients) pre- transplant transplant recurrence
- I
- 365
- 16
- 6.40
- 2.53
- 1036.36
- 256.52
- II
- 730
- 0
- Negative
- Negative
- 687.55
- 38.01
Table 1: Profile of follow-up and recurrence of HBV related HCC in the study population with respect to alpha-fetoprotein
| Parameter | Group I (n=67) | Group II (n=71) | ||||||
|---|---|---|---|---|---|---|---|---|
| Sex ratio (male: female) | 63:4 | 65:6 | ||||||
| Mean age (in years) | 54.5±7.1 | 53.7±6.8 | ||||||
| No. of tumor nodules (No. of patients) | ||||||||
| 1 | 20 | 25 | ||||||
| 2 | 43 | 41 | ||||||
| ≥3 | 4 | 5 | ||||||
| Size of tumor nodule (No. of patients) | ||||||||
| <2 cm | 18 | 22 | ||||||
| 2 cm-5 cm | 46 | 45 | ||||||
| ≥5 cm | 3 | 4 | ||||||
| Total tumor burden (No. of patients) | ||||||||
| Within UCSF criteria# (≤8 cm) | 62 | 68 | ||||||
| Beyond UCSF criteria (>8 cm) | 5 | 3 | ||||||
| Tumor differentiation (No. of patients) | ||||||||
| Well differentiated | 15 | 21 | ||||||
| Moderately differentiated | 41 | 43 | ||||||
| Poorly differentiated | 11 | 7 | ||||||
| MELD score [Median]$ | 12 | 13 |
Table 2: Profile of follow-up and recurrence of HBV related HCC in the study population with respect to alpha-fetoprotein (in IU/
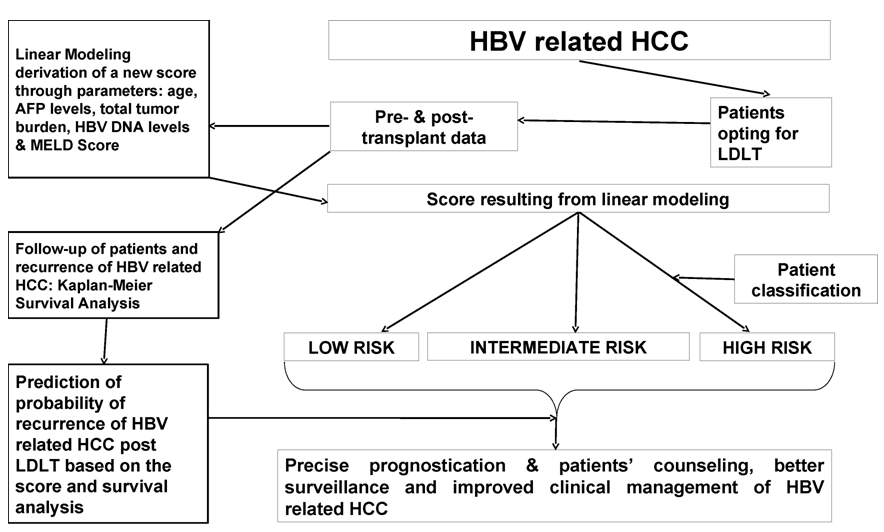
models (as depicted in Table 3 and Table 4), the parameters namely age (in years), alpha-fetoprotein (in IU/L) level, HBV DNA (in log10 copies/ml) level, total tumor burden and MELD score were found to be significantly correlated with the probability of post- transplant tumor recurrence of HBV related HCC (Figure 2).
Survival Analysis in HBV Related HCC
A multivariable Cox's proportional hazard modeling (Models 1-4) showing independent predictors of post transplant tumor recurrence is illustrated in Table 4. Survival analysis through Kaplan-Meier survival curves taking Group 1 & 2 into consideration with regard to HBV DNA and AFP levels is sketched in Figure 1.
A Novel Algorithm as a Post-Operative Management Strategy in HBV Related HCC
A novel algorithm stratifying patients opting for LDLT
into low, intermediate and high risk categories for developing post-transplant tumor recurrence of HBV related HCC is sketched in Figure 2.
Discussion
Our study elucidates a preliminary model to predict the probability of post-transplant tumor recurrence in HBV related HCC and a novel algorithm that stratifies patients opting for LDLT into low, intermediate and high risk categories for developing recurrence. Several studies have zeroed in on the illustration of predictive factors for HCC recurrence. Noninvasive fibrosis indices have been shown to predict intrahepatic distant recurrence (IDR) of HBV related HCC following radiofrequency ablation (RFA) [15]. Forns index is a predictor of recurrence and death in patients with HBV related HCC after curative resection [16]. Elevated preoperative neutrophil/lymphocyte ratios (NLR) have been shown to predict significantly increased risk of tumor recurrence in patients undergoing liver transplantation for HCC [17, 18]. Similarly, NLR at recurrence has been depicted as a prognostic factor affecting survival after recurrence in LDLT for HCC [19, 20]. Recent reports have also showed a significant association of pre-transplant platelet to lymphocyte ratio (PLR) of ≥125 with advanced tumor stage and aggressive tumor behavior suggesting its potential use as a prognostic tool for post-transplant HCC recurrence [21]. Additionally, previous reports have deliberated on the risk of hepatitis B recurrence after liver transplantation [22]. Our study explored the correlation between multiple clinicopathological variables in HBV mediated HCC and tumor recurrence. Unlike previous reports looking for association between one causative factor and one end point, our model is more holistic, taking multiple pre- and post-operative factors into consideration A generalized linear regression model (GLM) was derived that predicted the probability of recurrence through the predictive factors viz. age, total tumor burden, AFP and HBV DNA level and MELD score. The goodness of fit of the final model as depicted in our study was assessed by minimum AIC values. The novel algorithm depicted in our study will help to stratify patients as low risk, intermediate risk and high risk individuals who opt for LDLT as a therapeutic surgical regimen. Consistent with our results, a recent French study illustrates a validation of the AFP model as a predictor of HCC recurrence in patients with viral hepatitis-related cirrhosis who had received a liver transplant for HCC [23]. Further data elucidate several tumor, virological and biochemical factors to be tightly correlated with a higher cumulative risk of HCC recurrence post resection [24]. In the same vein, data display that a HBV viral load of >2,000 IU/mL (4 log10 copies/mL) is the most important correctable risk factor for HCC recurrence after resection [25]. Interestingly, among HCC patients with HBV-HCV co-infections, those with preoperatively high HBV DNA quantification or HBeAg seropositivity, essayed a short survival time and served as poor survival indicators [26]. Contrarily however, reports are suggestive of the fact that high levels of HBV surface antigen (HBsAg) increase risk of HCC in patients with low HBV viral load (27-28). Our model is a preliminary depiction based on pre- and post-transplant data from a limited number of patients. However, since the Indian subcontinent has a multiethnic population, our patient population included in the study may be considered as reasonably representative. Due to the limited number of cases and the specificity of HBV related HCC, this study probably couldn’t establish a significant association between pre-transplant data alone with the risk of tumor recurrence. Hence this model presently cannot be used for pre-transplant counseling of patients on disease recurrence. Larger multicentric studies using similar data and endpoints involving larger cohort of patients will help to refine our model further. Additionally, it is of paramount importance to verify our results among patients presenting with HCC of other etiologies.
Conclusions
Taken together, this is a first treatise on a preliminary depiction of a predictive model of post-transplant tumor recurrence in hepatitis B virus associated hepatocellular carcinoma. However, it is imperative to include a large number of patients opting for LDLT in future so that those patients may be differentiated into two independent cohorts such as a “test cohort” and a “validation cohort”. Subsequently, the new score obtained from the described equation from the test cohort can be legitimized on the validation cohort, which will then become a more powerful prognostic indicator. Additionally, our model will facilitate counseling of patients on the hazards of post-transplant recurrence and consequent critical insights on timely initiation of antiviral therapies may be obtained, thus facilitating better prognostication and management of this deadly disease.
Conflicts of Interest
The authors declare they have no conflict of interests.
Acknowledgements
This study was aptly supported by the Department of Biotechnology, Jamia Millia Islamia, New Delhi, India, in terms of infrastructure.
References
-
Jemal A, Bray F, Center MM, Ferlay J, Ward E, et al. (2011) Global cancer statistics. CA Cancer J Clin 61(2): 69-90.
-
Schütte K, Bornschein J, Malfertheiner P (2009) Hepatocellular carcinoma-epidemiological trends and risk factors. Dig Dis 27(2): 80-92.
-
Cha C, Fong Y, Jarnagin WR, Blumgart LH, DeMatteo RP (2003) Predictors and patterns of recurrence after resection of hepatocellular carcinoma. J Am Coll Surg 197(5): 753-758.
-
Shah SA, Cleary SP, Wei AC, Yang I, Taylor BR, et al. (2007) Recurrence after liver resection for hepatocellular carcinoma: risk factors, treatment, and outcomes. Surgery 141(3): 330-339.
-
Zimmerman MA, Ghobrial RM, Tong MJ, Hiatt JR, Cameron AM, et al. (2008) Recurrence of hepatocellular carcinoma following liver transplantation: a review of preoperative and postoperative prognostic indicators. Arch Surg 143(2): 182-188.
-
Wong SN, Reddy KR, Keeffe EB, Han SH, Gaglio PJ, et al. (2007) Comparison of clinical outcomes in chronic hepatitis B liver transplant candidates with and without hepatocellular carcinoma. Liver Transpl 13(3): 334-342.
-
Kiyici M, Yilmaz M, Akyildiz M, Arikan C, Aydin U, et al. (2008) Association between hepatitis B and hepatocellular carcinoma recurrence in patients undergoing liver transplantation. Transplant Proc 40(5): 1511-1517.
-
Saab S, Yeganeh M, Nguyen K, Durazo F, Han S, et al. (2009) Recurrence of hepatocellular carcinoma and hepatitis B reinfection in hepatitis B surface antigen- positive patients after liver transplantation. Liver Transpl 15(11): 1525-1534.
-
Ding C, Yang Z, Lv Z, DU C, Xiao H, et al. (2015) Long non-coding RNA PVT1 is associated with tumor progression and predicts recurrence in hepatocellular carcinoma patients. Oncol Lett 9(2): 955-963.
-
Hiwatashi K, Ueno S, Sakoda M, Iino S, Minami K, et al. (2015) Problems of Long Survival Following Surgery in Patients with NonBNonC-HCC: Comparison with HBV and HCV Related-HCC. J Cancer 6(5): 438-447.
-
Cho HJ, Kim SS, Ahn SJ, Park SY, Park JH, et al. (2015) Low serum interleukin-6 levels as a predictive marker of recurrence in patients with hepatitis B virus related hepatocellular carcinoma who underwent curative treatment. Cytokine 73(2): 245-252.
-
Yang Z, Zhuang L, Szatmary P, Wen L, Sun H, et al. (2015) Upregulation of heat shock proteins (HSPA12A, HSP90B1, HSPA4, HSPA5 and HSPA6) in tumour tissues is associated with poor outcomes from HBV-related early-stage hepatocellular carcinoma. Int J Med Sci 12(3): 256-263.
-
de Lope CR, Tremosini S, Forner A, Reig M, Bruix J (2012) Management of HCC. J Hepatol 56 Suppl 1: S75-87.
-
Lok AS, McMahon BJ (2007) Chronic hepatitis B. Hepatology 45 (2): 507-539.
-
Seo JY, Kim W, Kwon JH, Jin EH, Yu SJ, et al. (2013) Noninvasive fibrosis indices predict intrahepatic distant recurrence of hepatitis B-related hepatocellular carcinoma following radiofrequency ablation. Liver Int 33(6): 884-893.
-
Choi WM, Lee JH, Ahn H, Cho H, Cho YY, et al. (2015) Forns index predicts recurrence and death in patients with hepatitis B-related hepatocellular carcinoma after curative resection. Liver Int 35(8): 1992-2000.
-
Xiao GQ, Liu C, Liu DL, Yang JY, Yan LN, et al. (2013) Neutrophil-lymphocyte ratio predicts the prognosis of patients with hepatocellular carcinoma after liver transplantation. World J Gastroenterol 19(45): 8398- 8407.
-
Wang GY, Yang Y, Li H, Zhang J, Jiang N, et al. (2011) A scoring model based on neutrophil to lymphocyte ratio predicts recurrence of HBV-associated hepatocellular carcinoma after liver transplantation. PLoS One 6(9): e25295.
-
Harimoto N, Shirabe K, Nakagawara H, Toshima T, Yamashita Y, et al. (2013) Prognostic factors affecting survival at recurrence of hepatocellular carcinoma after living-donor liver transplantation: with special reference to neutrophil/lymphocyte ratio. Transplantation 96(11): 1008-1012.
-
Motomura T, Shirabe K, Mano Y, Muto J, Toshima T, et al. (2013) Neutrophil-lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment. J Hepatol 58(1): 58-64.
-
Xia W, Ke Q, Wang Y, Wang W, Zhang M, et al. (2015) Predictive value of pre-transplant platelet to lymphocyte ratio for hepatocellular carcinoma recurrence after liver transplantation. World J Surg Oncol 13: 60.
-
Xu X, Tu Z, Wang B, Ling Q, Zhang L, et al. (2011) A novel model for evaluating the risk of hepatitis B recurrence after liver transplantation. Liver Int 31(10): 1477-1484.
-
Notarpaolo A, Layese R, Magistri P, Gambato M, Colledan M, et al. (2017) Validation of the AFP model as a predictor of HCC recurrence in patients with viral hepatitis-related cirrhosis who had received a liver transplant for HCC. J Hepatol 66(3): 552-559.
-
Hung IF, Wong DK, Poon RT, Fong DY, Chui AH, et al. (2016) Risk Factors and Post-Resection Independent Predictive Score for the Recurrence of Hepatitis B- Related Hepatocellular Carcinoma. Plos One 11(2): e0148493.
-
Hung IF, Poon RT, Lai CL, Fung J, Fan ST, et al. (2008) Recurrence of hepatitis B-related hepatocellular carcinoma is associated with high viral load at the time of resection. Am J Gastroenterol 103(7): 1663- 1673.
-
Fu XT, Shi YH, Zhou J, Peng YF, Liu WR, et al. (2017) Association of hepatitis status with surgical outcomes in patients with dual hepatitis B and C related hepatocellular carcinoma. Infect Agent Cancer 12: 28.
-
Tseng TC, Liu CJ, Yang HC, Su TH, Wang CC, et al. (2012) High levels of hepatitis B surface antigen increase risk of hepatocellular carcinoma in patients with low HBV load. Gastroenterology 142(5): 1140- 1149.e3.
-
Huang G, Lau WY, Zhou WP, Shen F, Pan ZY, et al. (2014) Prediction of Hepatocellular Carcinoma Recurrence in Patients With Low Hepatitis B Virus DNA Levels and High Preoperative Hepatitis B Surface Antigen Levels. JAMA Surg 149(6): 519-527.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient