Esophageal Heterotopic Gastric Mucosal: How to Deal with it in CDH1 Mutation Carriers?
Opinion
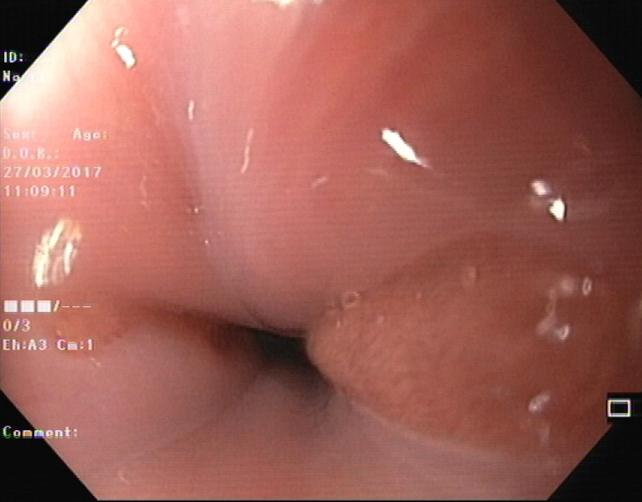
Germline mutations in CDH1 gene have been implied in the development of early-onset diffuse gastric cancer which often presents with multiple foci of signet ring cell carcinoma not effectively detected by endoscopy. Accordingly, prophylactic total gastrectomy is the only risk-reducing measure for gastric cancer in CDH1 mutation carriers [1, 2, 3]. Although the vast majority of gastric specimens already present signet ring cell carcinoma foci, this surgical approach potentially eradicate gastric mucosa and no reports of malignant recurrence has been described [4]. However, the presence of gastric heterotopic mucosal in esophagus is not a rare endoscopic finding and, to our knowledge, there are no recommendations regarding the presence of gastric heterotopic mucosal in CDH1 mutation carriers [5]. In our department of Gastroenterology, we are currently following 18 patients with CDH1 mutation. In this manuscript we are going to focus on two of those patients. Accordingly to current guidelines, they were first submitted to a baseline upper endoscopy (using Cambridge protocol) without no endoscopic or histological lesions. However in these two patients, we observed small inlet salmon colored patches just below the upper esophageal sphincter suggesting heterotopic gastric mucosal (Figure 1). These findings were confirmed after histologic assessment: gastric heterotopic mucosal without malignancy. After careful counseling and multidisciplinary discussion they were submitted to a prophylactic total gastrectomy. The histopatological evaluation revealed a pT1aN0M0 tumor in both cases.
How to manage these cases? The risk of diffuse gastric cancer is still present in these patients? We think that this case constitutes a unique opportunity to debate which is the best clinical approach to CHD1 mutation carriers with heterotopic gastric mucosal.
Less than 50 cases of primary adenocarcinoma arising from heterotopic gastric mucosa have been described, mostly surgically treated, but endoscopic resection appears safe and efficacious in recent published cases [6, 7]. In this particular case, a proximal surgical extension may be not an ideal approach in a benign setting considering non-negligible morbidity and mortality. Endoscopic ablative techniques may not guarantee a complete mucosal eradication, local recurrence or allow the access to a precise histopathological evaluation. Probably only an endoscopic resection can ensure complete resectability and a histopathological evaluation capable of defining the subsequent therapeutic and follow-up strategy. In conclusion, despite the Cambridge protocol, only a meticulous evaluation, outside gastric cavity and gastroesophageal junction in initial surveillance endoscopy may detect these findings. Not only esophageal, but also duodenal heterotopic mucosa, are within range of upper endoscopic observation which may alter the extent of the prophylactic resection. All these areas may well be included for further biopsies and managed accordingly. With no clear evidence of carcinoma rising in these patients, but with a not negligible risk of cancer, endoscopic resection through piecemeal EMR seems to be the most convenient and safe procedure to consider.
| Brandão C1, Castro R1* and Dinis Ribeiro M1,2 1Department of Gastroenterology, Instituto Português de Oncologia do Porto, Portugal 2Porto Faculty of Medicine, Biostatistics and Medical Informatics, Portugal | Opinion | ||
| Volume 3 Issue 1 | |||
| Received Date: August 07, 2018 | |||
| Published Date: August 20, 2018 |
References
-
Guilford P, Hopkins J, Harraway J, McLeod M, McLeod N, et al. (1998) E-cadherin germiline mutations in familial gastric cancer. Nature 392(6674): 402-405.
-
Fitzgerald RC, Hardwick R, Huntsman D, Carneiro F, Guilford P, et al. (2010) International Gastric Cancer Linkage Consortium. J Med Genet 47(7): 436-444.
-
van der Post RS, Vogelaar IP, Carneiro F, Guilford P, Huntsman D, et al. (2015) Hereditary diffuse cancer: updated clinical guidelines with an emphasis on germline CDH1 mutation carriers. J Med Gastr 52(6): 361-374.
-
Norton JA, Ham CM, Van Dam J, Jeffrey RB, Longacre TA, et al. (2007) CDH1 truncating mutations in the E- cadherin gene: an indication for total gastrectomy to treat hereditary diffuse gastric cancer. Ann Surg 245(6): 873-879.
-
Chong VH (2013) Clinical significance of heterotopic gastric mucosal patch of the proximal esophagus. World J Gastroenterol 19(3): 331-338.
-
Kadota T, Fujii S, Oono Y, Imajoh M, Yano T, et al. (2016) Adenocarcinoma arising fromheterotopic gastric mucosa in the cervical esophagus and upper thoracic esophagus: two case reports and literature review. Expert Rev Gastroenterol Hepatol 10(3): 405- 414.
-
Hudspeth VR, Smith DS, Pacicco T, Lewis JJ (2016) Successful endoscopic resection of adenocarcinoma arising in an esophageal inlet patch. Dis Esophagus 29(7): 880-882.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient