Pre-operative Predictive Factors of Long-Term Weight Loss Following Bariatric Surgery: A 3-Year Retrospective Review
Background: With the growing prevalence of obesity, bariatric surgery has become increasingly popular. Despite this, studies have shown that a number of patients fail to achieve successful weight loss. However, there still remains limited long-term data. Aim: Identify pre-operative factors associated with long-term weight loss 3 years post-surgery. Methods: A retrospective, cohort study was performed at the CNY Bariatric Center on patients undergoing bariatric surgery from 2003-2008. Charts of 656 subjects were reviewed. Post-op weight gain, complications, and resolution of co-morbid conditions up to 36 months were assessed. Descriptive statistics compared subjects with post-op weight gain (Group A) versus those with weight loss maintenance (Group B) at 24 and 36 months. Results: Of the subjects meeting inclusion criteria, 61% and 66% gained weight at 24 and 36 months. At 24 months, there was a significant difference in weight gain between Caucasian (63%) and non-Caucasian (37%) subjects (p=0.003). At 36 months, in subjects with persistent diabetes, 62% had weight gain versus 38% that maintained weight loss. Pre-op % excess weight loss (EWL) did not confer an advantage to weight loss maintenance at 36 months (p=0.748). There was a significant difference (p=0.0002) at 6 months post-op in %EWL between Groups A and B. However, on multivariate logistic regression analysis, no predictors of weight loss maintenance were found. Conclusions: No statistically significant pre-operative predictive factors of weight loss maintenance were identified in this 3-year review. These findings are consistent with prior studies that have shown similar results up to 18 months.
Introduction
The worldwide epidemic of overweight (body mass index [BMI] ≥25kg/m2) and obese (BMI≥30kg/m2) individuals is estimated to be 2.1 billion, with the highest percentage in the United States [1]. Results from the 2013-2014 National Health and Nutrition Examination Survey estimate that 32.5% of U.S. adults aged 20 and over are overweight, and 37.7% are obese [2]. With the increasing prevalence of obesity, there has been an associated rise in obesity-related comorbidities such as type 2 diabetes (DM), heart disease (CAD), obstructive sleep apnea (OSA), and weight-bearing degenerative joint disease (DJD) [3]. Medical interventions including dietary measures and pharmaceutical agents remain only moderately effective. In 1991, the NIH established guidelines for the surgical therapy of morbid obesity (BMI≥40 kg/m2 or BMI≥35kg/m2 with significant comorbidities) [4]. At present, bariatric surgery is the most effective method of ensuring significant and sustained weight loss for the morbidly obese, with the additional benefits of improving obesity-related comorbidities and quality of life [3, 5]. The majority of patients undergoing bariatric surgery achieve a successful degree of weight loss which is defined as >50% excess weight loss [6]. Despite this, a significant minority (15- 20%) fail to achieve this goal [6]. To assess this disparity, researchers have attempted to study preoperative predictors of weight loss following bariatric surgery; however, few studies report long-term results with sufficient patient follow-up [7, 8, 9]. Our objective was to identify pre-operative factors associated with long-term weight loss 3 years post-bariatric surgery.
Methods
Retrospective Chart Review Inclusion Criteria
With approval from the Institutional Review Board at SUNY Upstate Medical University, a retrospective chart review was initiated to identify patients undergoing bariatric surgery over a 5-year period, from January 1, 2003 to December 31, 2008, at the Central New York Bariatric Surgery Center (CNYBSC). The CNYBSC is the only accredited Level 1A American College of Surgeons Bariatric Surgery Center Network in Central New York. The CNYBSC performs over four hundred bariatric surgeries per year. Surgical options available at the CNYBSC include the gastric sleeve (GS), laparoscopic adjustable gastric banding (LAGB), and Roux-en-Y gastric bypass (RNY). Charts of 656 subjects were reviewed. Only patients with at least 18 months of follow up were included in the study.
Chart Review Data Collection
Data abstracted from the charts included pre-operative demographic, psychosocial, and medical data. The medical data retrieved included pre- and post-operative: body mass index (BMI), weight loss, % excess weight loss (%EWL), and type of surgery, hypertension, dyslipidemia, diabetes mellitus, coronary artery disease, obstructive sleep apnea, degenerative joint disease, depression, and bipolar disorder. To determine weight change prior to surgery, BMIs from the first clinic visit were compared with BMIs at the time of operation. These values were compared with ideal body weight to calculate the %EWL prior to surgery [10]. Data on post-operative complications were also collected. Post-operative weight gain, complications, and resolution of co-morbid conditions were assessed at 6, 12, 18, 24, and 36 months respectively.
Statistical Analysis
Statistical analysis was performed by the Center for Research and Evaluation at SUNY Upstate Medical University. Descriptive statistics compared subjects with post-operative weight gain versus those with weight loss maintenance at 24 and 36 months (Group A=gained weight, Group B=maintained weight loss). Weight gain was defined as any increase in weight since their previous clinic visit (clinic visits occurred every 3-6 months). Multivariate logistic regression analysis was performed to build a prediction model for successful weight loss maintenance.
Results
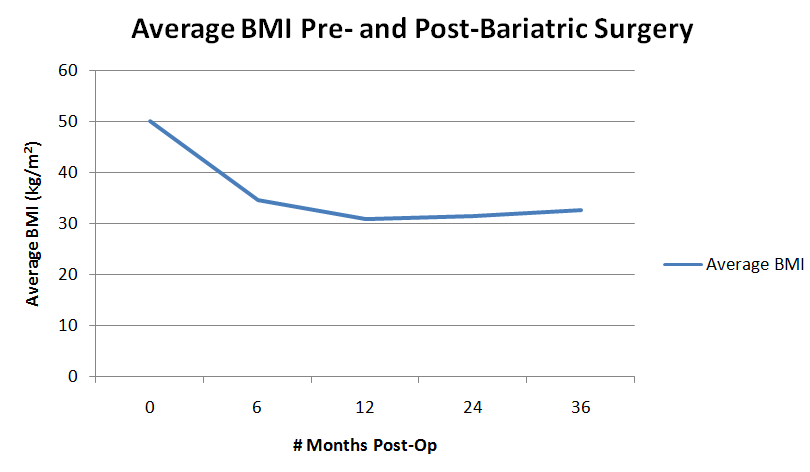
The majority of subjects receiving weight reduction surgery underwent RNY (94%). The remaining 6% underwent LAGB. 71% (469/656) of subjects fulfilled the inclusion criteria. 61% (218/359) and 66% of subjects (174/263) gained weight at 24 and 36 months, respectively (Group A=gained weight, Group B=maintained weight loss). Average BMI plateaued at 12 months, with a slow progressive rise in BMI at 24 and 36 months (Figure 1).
6 Months Post-Bariatric Surgery
At 6 months post-op, there was a statistically significant difference in %EWL between Groups A and B (p=0.0002). However, on multivariate logistic regression analysis, no significant predictors of weight loss maintenance were found. As shown in Figure 1, the most profound weight loss occurred at 6 months post-surgery (average pre-operative BMI= 50.2kg/m2 and average 6 month post-op BMI=34.7kg/m2).
24 Months Post-Bariatric Surgery
At 24 months, there was no significant difference in post-operative weight gain between male and female subjects (60% and 63%, p=0.649) (Table 1). Mean age of subjects between both groups were similar (49.3 and 48.2 years). At 24 months, there was a statistically significant difference in post-operative weight gain between Caucasian and non-Caucasian subjects (63% and 37%, p=0.003). At 24 months, 62% of patients that lost weight pre-operatively re-gained weight at 24 months compared to 38% that maintained weight loss. Pre-operative %EWL did not confer an advantage to weight loss maintenance at
24 months (p=0.784). At 24 months, in the patients with persistent diabetes, 65% had weight gain versus 35% that maintained weight loss. This difference was not statistically significant. In the patients with persistent degenerative joint disease, 62% gained weight at 24 months compared to 38% that maintained weight loss. At 24 months, there was no significant difference in weight gain between depressed and non-depressed subjects (58% and 65% respectively, p=0.162). Of those with persistent depression, 58% of patients gained weight at 24 months versus 42% that maintained weight loss. At 24 months, there was no significant difference in post- operative weight gain between those that did and did not develop post-operative complications (p=0.545). The average BMI at 24 months was 31.4kg/m2 (Figure 1), with an average weight re-gain of 6.2 pounds (range 0-64 pounds).
| Gained Weight (Group A) | Maintained Weight Loss (Group B) | ||||||||
| p-value | |||||||||
| No./Total No. (%) | No./Total No. (%) | ||||||||
| Gender | 0.649 | ||||||||
| Female | 180/299 (60.2) | 119/299 (39.8) | |||||||
| Male | 38/60 (63.3) | 22/60 (36.7) | |||||||
| Race | 0.003 | ||||||||
| Caucasian | 205/324 (63.3) | 119/324 (36.7) | |||||||
| Non-Caucasian | 13/35 (37.1) | 22/35 (62.9) | |||||||
| Pre-op %EWL | 0.492 | ||||||||
| 0-5% | 94/160 (58.8) | 66/160 (41.2) | |||||||
| >5% | 124/199 (62.3) | 75/199 (37.7) | |||||||
| Diabetes | 0.364 | ||||||||
| Yes | 62/96 (64.6) | 34/96 (35.4) | |||||||
| No | 156/263 (59.3) | 107/263 (40.7) | |||||||
| DJD | 0.34 | ||||||||
| Yes | 166/267 (62.2) | 101/267 (37.8) | |||||||
| No | 52/92 (56.5) | 40/92 (43.5) | |||||||
| Depression | 0.162 | ||||||||
| Yes | 123/213 (57.7) | 90/213 (42.3) | |||||||
| No | 95/146 (65.1) | 51/146 (34.9) | |||||||
| Post-op complications | 0.545 | ||||||||
| Yes | 10/14 (71.4) | 4/14 (28.6) | |||||||
| No | 106/167 (63.5) | 61/167 (36.5) |
Table 1: Demographic and Medical Variables of Group A and Group B at 24 Months Post-Bariatric Surgery. %EWL=% excess weight loss;
36 Months Post-Bariatric Surgery
At 36 months, 60% of the original cohort was lost to follow-up. There was a trend toward a difference in weight gain between males and females at 36 months (68.1% and 52.9%, p=0.087), but this did not reach statistical significance (Table 2). Mean age of subjects between both groups were similar (49.8 and 51.9 years). At 36 months there was no significant difference in post- operative weight gain between Caucasian and non- Caucasian subjects (68% and 54%, p=0.166). At 36 months, 65% of patients that lost weight pre-operatively re-gained weight at 36 months compared to 35% that maintained weight loss. There was no significant difference in post-operative weight gain among subjects that did and did not lost weight pre-operatively (65% and 67%, p=0.748). Pre-operative %EWL did not confer an advantage to weight loss maintenance at 36 months (p=0.938). At 36 months, in the patients with persistent diabetes, 62% had weight gain versus 38% that maintained weight loss. Of those with resolution of diabetes at 36 months, 68% had weight gain versus 32% that maintained weight loss. In the patients with persistent degenerative joint disease, 66% gained weight at 36 months compared to 34% that maintained weight loss. At 36 months, there was no significant difference in post-operative weight gain among depressed and non- depressed subjects (66% and 66% respectively, p=0.893). Of those with persistent depression, 66% of patients gained weight at 36 months versus 34% that maintained weight loss. At 36 months, there was no significant difference in post-operative weight gain among subjects with and without post-operative complications (p=0.545). The average BMI at 36 months was 32.6 kg/m2, with average weight re-gain of 9.9 pounds (range 0-64 pounds).
| Gained Weight (Group A) | Maintained Weight Loss (Group B) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| p-value | |||||||||
| No./Total No. (%) | No./Total No. (%) | ||||||||
| Gender | 0.087 | ||||||||
| Female | 156/229 (68.1) | 73/229 (31.9) | |||||||
| Male | 18/34 (52.9) | 16/34 (47.1) | |||||||
| Race | 0.166 | ||||||||
| Caucasian | 159/235 (67.7) | 76/235 (32.3) | |||||||
| Non-Caucasian | 14/26 (53.8) | 12/26 (46.2) | |||||||
| Pre-op %EWL | 0.748 | ||||||||
| 0-5% | 72/107 (67.3) | 35/107 (32.7) | |||||||
| >5% | 102/156 (65.4) | 54/156 (34.6) | |||||||
| Diabetes | 0.402 | ||||||||
| Yes | 48/77 (62.3) | 29/77 (37.7) |
Table 2: Demographic and Medical Variables of Group A and Group B at 36 Months Post-Bariatric Surgery. %EWL=% excess weight loss;
| No | 126/186 (67.7) | 60/186 (32.3) | |
|---|---|---|---|
| DJD | 0.995 | ||
| Yes | 133/201 (66.2) | 68/201 (33.8) | |
| No | 41/62 (66.1) | 21/62 (33.9) | |
| Depression | 0.893 | ||
| Yes | 109/164 (66.5) | 55/164 (33.5) | |
| No | 65/99 (65.7) | 34/99 (34.3) | |
| Post-op complications | 0.809 | ||
| Yes | 9/13 (69.2) | 4/13 (30.8) | |
| No | 165/250 (66.0) | 85/250 (34.0) |
Table 3: Demographic and Medical Variables of Group A and Group B at 36 Months Post-Bariatric Surgery. %EWL=% excess weight loss;
Discussion
Our findings suggest that of the variables reviewed including pre- and post-operative: body mass index (BMI), surgery type, hypertension, dyslipidemia, diabetes mellitus, coronary artery disease, obstructive sleep apnea, degenerative joint disease, and depression, there were no significant pre-operative predictors of long-term weight loss maintenance 36 months post-surgery. These findings are consistent with previous studies that have shown similar results up to 18 months. As documented in the results section, BMI precipitously dropped at 6 months post-surgery. Despite this, BMI plateaued at 12 months and trended up at 24 and 36 months post-surgery, which is similar to previous studies [11]. Prior meta-analyses have indicated that mandatory pre-operative weight loss is positively associated with weight loss after surgery [6]. However, the mean follow-up time in these studies ranged from 13 to 24 months [6]. As shown in our results, pre-operative %EWL did not confer an advantage to weight loss maintenance at both 24 and 36 months. These findings suggest that institution of weight loss behavior prior to surgery confers no long-term post-operative benefit. At 6 months post-op, there was a statistically significant difference in %EWL between Groups A and B (p=0.0002), suggesting the possibility that %EWL at 6 months may predict long-term outcomes and act as a time point for early intervention. However, on multivariate logistic regression analysis, there was no significant difference found. There is suggestion from our study that race may play a role in post-operative weight gain. At 24 months, there was a statistically significant difference in post-operative weight gain between Caucasian and non-Caucasian subjects. However, this significance was lost on multivariate regression analysis and was not recognized at 36 months post-surgery. This was likely due to the large sample size of Caucasian subjects undergoing surgery compared to non-Caucasian counterparts. It is well documented in the literature that type 2 diabetes mellitus resolves rapidly post-bariatric surgery [3]. Our findings showed that at 36 months, of those with persistent diabetes, 62% had weight gain versus 38% that maintained weight loss. This suggests that the mechanism behind resolution of type 2 diabetes post-RNY may extend beyond weight loss alone. The Surgical Treatment and Medications Potentially Eradicate Diabetes Efficiently (STAMPEDE) trial revealed that RNY and sleeve gastrectomy were superior to intensive medical therapy alone in achieving glycemic control one-year post randomization [12]. Follow-up data from the STAMPEDE trial confirmed that intensive medical therapy plus bariatric surgery yielded superior glycemic control in significantly more patients compared to medical therapy alone, 3 and 5 years post-surgery. This displays that surgery is a durable option for the long-term treatment of diabetes with high levels of supervision [13, 14]. Statistically our study revealed that the presence or absence of depression plays no role in post-operative weight gain. Despite this, the majority of patients with persistent depression did gain weight at 36 months post- operatively (66% gained weight vs. 34% maintained weight loss), suggesting that pre- and post-op follow up with mental health experts may be beneficial to those with depression and maintaining successful weight loss. Limitations of our study included a portion of our cohort being lost follow up, with 55% of the cohort following up at 24 months, and 40% at 36 months. Despite a substantial number of subjects lost to follow-up, this appears to be a common problem among long-term follow-up bariatric studies. A recent systematic review assessing long-term follow-up of bariatric surgery identified only 16% (1136/7371) of studies reporting outcomes more than 2 years post-surgery, with <3% (29/1136) reporting weight loss outcomes for more than 80% of the original cohort [7]. Therefore, long-term continuity does appear to be a profound issue. Additionally, there are studies that have been performed up to 10 years post-surgery, but sample size remains small [15, 16, 17]. Further limitations included the lack of access to lab values to assess for the resolution of diabetes and dyslipidemia. The cessation of medications was used to follow the resolution of co-morbidities.
Conclusions
In summary, no statistically significant pre-operative predictive factors of weight loss maintenance were identified in this 3-year review. These findings are consistent with prior studies that have shown similar results up to 18 months. As shown in previous studies, the majority of patients undergoing bariatric surgery do achieve a successful degree of weight loss [6]. Despite this, there is a significant minority (15-20%) who fail to achieve this goal, and as our study suggests, many people re-gain weight post-operatively or plateau at 12 months [6]. In order to optimize resource allocation and avoid exposing patients unlikely to benefit from surgery to its inherent risks, further research needs to be done to identify those patients most likely to obtain successful results. Additionally, further investigation needs to be performed assessing a multidisciplinary approach to the bariatric patient (bariatric surgeon, internist, psychologist, and dietician) over an extended period, and whether or not this improves outcomes.
Conflict of Interest
There are no conflicts of interest to disclose for Christine M. Granato, MD, Uma Murthy, MD, Dongliang Wang, PhD, Elizabeth Weinshel, MD and Renee Williams, MD
Acknowledgments
We would like to express our appreciation to Crystal Whitney, MD and Brittany Misercola, MD who contributed to data collection for this project.
References
-
Ng M, Fleming T, Robinson M, Thomson B, Graetz N, et al. (2014) Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384(9945): 766-781.
-
Fryar C, Carroll M, Ogden C (2016) Prevalence of Overweight, Obesity, and Extreme Obesity among Adults Aged 20 and Over: United States, 1960–1962 through 2013-2014.
-
Buchwald H, Yoav Avidor, Eugene Braunwald, Michael D Jensen, Walter Pories, et al. (2004) Bariatric surgery: a systematic review and meta- analysis. JAMA 292(14): 1724-1737.
-
(1991) NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med 115(12): 956-961.
-
Marihart CL, Brunt AR, Geraci AA (2014) Older adults fighting obesity with bariatric surgery: Benefits, side effects, and outcomes. SAGE Open Med 2: 2050312114530917.
-
Livhits M, Mercado C, Yermilov I, Parikh JA, Dutson E, et al. (2012) Preoperative predictors of weight loss following bariatric surgery: systematic review. Obes Surg 22(1): 70-89.
-
Puzziferri N, Roshek TB, Mayo HG, Gallagher R, Belle SH, et al. (2014) Long-term follow-up after bariatric surgery: a systematic review. JAMA 312(9): 934-942.
-
Arterburn D, Livingston EH, Olsen MK, Smith VA, Kavee AL, et al. (2013) Predictors of initial weight loss after gastric bypass surgery in twelve Veterans Affairs Medical Centers. Obes Res Clin Pract 7(5): e367-376.
-
Karmali S, Brar B, Shi X, Sharma AM, de Gara C, et al. (2013) Weight recidivism post-bariatric surgery: a systematic review. Obes Surg 23(11): 1922-1933.
-
Still CD, Benotti P, Wood GC, Gerhard GS, Petrick A, et al. (2007) Outcomes of preoperative weight loss in high-risk patients undergoing gastric bypass surgery. Arch Surg 142(10): 994-998.
-
Colquitt JL, Pickett K, Loveman E, Frampton GK (2014) Surgery for weight loss in adults. Cochrane Database Syst Rev 8(8): CD003641.
-
Schauer PR, Kashyap SR, Wolski K, Brethauer SA, Kirwan JP, et al. (2012) Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med 366(17): 1567-1576.
-
Schauer PR (2014) Bariatric surgery versus intensive medical therapy for diabetes--3-year outcomes. N Engl J Med 370(21): 2002-2013.
-
Schauer PR, Bhatt DL, Kashyap SR (2017) Bariatric Surgery or Intensive Medical Therapy for Diabetes after 5 Years. N Engl J Med 376(20): 1997.
-
Angrisani L, Cutolo PP, Formisano G, Nosso G, Vitolo G (2013) Laparoscopic adjustable gastric banding versus Roux-en-Y gastric bypass: 10-year results of a prospective, randomized trial. Surg Obes Relat Dis 9(3): 405-413.
-
Angrisani L, Lorenzo M, Borrelli V (2007) Laparoscopic adjustable gastric banding versus Roux- en-Y gastric bypass: 5-year results of a prospective randomized trial. Surg Obes Relat Dis 3(2): 127-132.
-
Sjöström L (2013) Review of the key results from the Swedish Obese Subjects (SOS) trial-a prospective controlled intervention study of bariatric surgery. J Intern Med 273(3): 219-234.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient