Gastric Fermentation in Functional Dyspepsia
Background: The role of the gastric fermentation in functional dyspepsia has been investigated. Methods: Lactulose Hydrogen Breath test, H. pylori 13C Urea Breath Test. 47 patients with functional dyspepsia (FD) has been investigated. Results: Positives for lactulose hydrogen breath test 23, negatives 24. H. pylori and hydrogen breath test positives 12.
Introduction
At least 20% of the population has chronic symptoms that can be attributed to disorders of gastroduodenal function, and the majority of these people have no evidence of organic causes [1]. Diagnostic criteria: One or more of the following bothersome: postprandial fullness, early satiation, epigastric pain, epigastric burning and no evidence of structural disease,(including an upper endoscopy) that is likely to explain the symptom onset at least 3 months with symptom onset at least 6 months before diagnosis [2]. The bacterium Helicobacter pylorus is found in 40% of the population and is responsible for the development of the duodenal ulcer disease. The infection also is a cause of gastric ulcer diseases, and of some cases of non-ulcer dyspepsia and gastric adenocarcinoma [3, 4]. In an analogous way, the post- infectious in the IBS (Irritable Bowel Syndrome), several studies have identified the novo development of FD following an enteric infection. Giardia lamblia infection has been shown to provoke visceral hypersensitivity and delay gastric emptying [5]. Besides the bacteria E.coli in gastric infection can produce dysmotility [6]. The latest iteration of the Rome IV, published in 2016, represents a significant departure from prior version with a much broader approach to the definition and potential pathophysiology of functional gastrointestinal disorders and now recognizes the possible contribution of such phenomena as low-grade inflammation, changes in the gut micro biota, and altered brain processing to the pathogenesis of the symptoms [7]. Finally the growth of bacteria was demonstrated with culture of gastric biopsy [8].
Hydrogen breath test using various substrates like glucose, lactulose, lactose and fructose are being used more and more to diagnose small intestinal bacterial overgrowth (SIBO) and lactose or fructose malabsorption. Though quantitative culture of jejuna aspirate is considered as gold standard for the diagnosis of SIBO, hydrogen breath test, in spite of their low sensitivity, are popular for their non-invasiveness [9].
Definition
Functional Dyspepsia (FP): refers to chronic or recurrent pain or discomfort, located in the central part of the upper abdomen (epigastrium). Diagnostic criteria: One or more of the following:
- Bothersome postprandial fullness.
- Bothersome early satiation.
- Bothersome epigastric pain.
- Bothersome epigastric burning.
And no evidence of structural disease (including at upper endoscopy) that is likely to explain the symptoms. No evidence of organic, systemic or metabolic disease that is likely to explain the symptoms on routine investigations. Criteria fulfilled for the last 3 months with symptoms onset at least 6 months before diagnosis [2].
Materials and Methods
Lactulose Breath Test
The patient must have fasted for 12 hours before the test, cigarette smoking and exercise are avoided 2 hours before and during the test, pro-motility and anti-motility drugs, antibiotics have to be avoided at least 2 weeks before of the test.
Patients (N:47) were studied with symptoms of FD such as: pain, bloating, feeling of fullness, nausea, discomfort for at least 3 months before consulting. None of the patient had gastric cancer, previous surgery, or had undergone chemotherapy, radiotherapy or was diabetics or immune deficient. Ages ranged from 14 to 71 years old. We give the patient an exposure dose of 10 g of lactose dissolved in 400 ml of water, after obtaining samples of the final exhaled air every 15 minutes during the first hour, followed every 30 minutes in the next hour. If the average basal values of breath hydrogen were higher, we continue the test for other samples at 15 and 30 minutes. We considered gastric fermentation, when the lactulose have contact with bacteria in the stomach, as normally after of 30 minutes the lactulose is in small intestine.
The C13 Urea Breath Test
A substrate (urea) labeled with Carbon 13 is administered to the patient and exhaled breath is collected to detect the possible catabolism product (CO2 labeled with C13). Breath samples are collected before and 30 minutes after urea was given. The substrate containing 75mg C13 labeled urea in 50ml of water. <4 DOB (Delta over Base) negative and > de 4 DOB positive.
Results
Patients (n=47) were studied. Ages between 14 to 71 years old.
| Males | 26(55.3%) | Females | 21(44.7%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Positives to SIBO | 23 (48.9%) | Negatives | 24(51.1%) | ||||||||
| Positives to SIBO and H. pylori | 8 (17.0%) | ||||||||||
| Negatives to SIBO and positives for H. pylori | 3 (6.3%) |
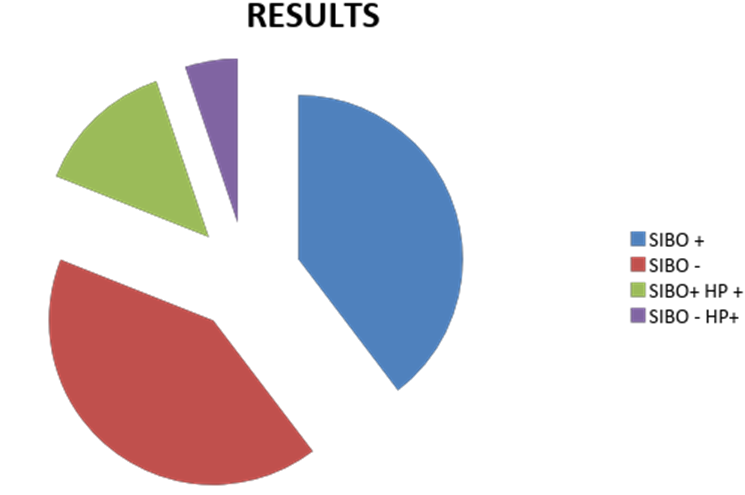
This study was performed to analyze the possible role of the gastric fermentation in functional dyspepsia, all studied patients presented gastric fermentation in functional dyspepsia; besides 6.3% were H. pylori Urea Breath test positive. The incidence for women and men was similar Figure 1. All patients were adults, ages between 14 to 71 years old.
Conclusion
In normal conditions the gastric PH is very low (0.9-1) and acts as a bactericide barrier. However in pathological situations like gastro paresis, stress, duodenogastric reflux and in the present the long time use of antacids, antagonists of H2- receptors and proton pump inhibitors, are producing an increase of the PH, provoking hypochlorhydria that favors the colonization of bacteria and other microorganisms like Giardia lamblia, fungus, etc., and causing gastric fermentation and functional dyspepsia.
Finally the hydrogen breath test can have a clinical importance to evaluate the presence of pathogenic bacteria in the stomach, besides of Helicobacter pylori, than can produce gastric fermentation in functional dyspepsia we propose to consider gastric fermentation as a co-factor in the development of FD [10, 11].
References
-
Jack J, Talley NJ, Camilleri M, Holtmann G, HuS P, et al. (2006) Functional gastroduodenal Disorders. Gastroenterology 130(5): 1466-1479.
-
Stanghellini V, Chan FK, Hasler WL, Malagelada JR, Suzuki H, et al. (2016) Gastroduodenal Disorders. Gastroenterology 150(6): 1380-1391.
-
Caras SD, David AY (1998) Ulcera Peptica y Helicobacter pylori. Secretos de la Gastroenterologia. McGraw-Hill, pp: 81-88.
-
McNulty C, Owen R, Tompkins D, Hawtin P, McColl K, et al. (2002) Helicobacter pylori susceptibility testing by disc diffusion. J antimicrob chemother 49(40: 601- 609.
-
Dizdar V, Gilja OH, Hauskent (2007) Increased Visceral Sensitivity in Giardia-induced post infectious Irritable Bowel Syndrome and Functional Dyspepsia, Effect of the 5HT3-antagonist ondansetron. Neurogastroenterol Motil 19(12): 977-982.
-
Catalayud S, Garca Zaragoza E, Quintana E, Filipo V, Esplugues JV, et al. (2001) Role of Nitric Oxide and Prostaglandins on the endotoxin on gastric emptying. Gastroenterology 120(5): A464.
-
Koduru P, Irani M, Quigley EMM (2018) Definition, pathogenesis and management of that cursed Dyspepsia. Clin Gastroenterol Hepatol 16(4): 467-479.
-
Barrios A, Barrios R, Rodas A, Colop M (2002) Las Torres Clinic, Quetzaltenango, (Guatemala), Gastric Infections, biliary gastritis-DGRD, Poster session F: Gastrointestinal infections, Tropical and Parasitic Diseases, P.F. 002. World Congress of Gastroenterology, Bangkok Thailand, pp: 192.
-
Ghosal UC (2011) How to interpret Hydrogen Breath Tests. J Neurogastroenterol Motil 17(3): 312-317.
-
Gisberte JP, Gonzalez-Lama Y (2005) Pruebas de Aliento en las Enfermedades Digestivas, Servicio de Aparato Digestivo. Hospital Universitario de la Princesa. Madrid. Gastroenterol Hepatol, España 2005(7): 407-416.
-
Corindaldesi R, Barbara G, Stanghellini V (1999) Helicobacter pylori, Gastritis and Functional Dyspepsia. Approach To The Patient With Chronic Gastrointestinal Disorders, Edited by E. Corazziari. Dipartimento Scienze Cliniche, Clinica Medica II, Universita "La Sapienza", Italy, pp: 245-251.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient