Agenesis of the Gallbladder: About A Case
The agenesis of the gallbladder is a rare, unsung congenital anomaly, presenting itself in different clinical forms. The ultrasound balance sheet often describes a lichen-atrophic vesicle, which can lead to unnecessary and potentially dangerous surgery. We report the case of a 45-year-old patient with no history of Cholecystitis, with cholestasis jaundice and whose ultrasound diagnosis of lichen-atrophic vesicle was questioned. Magnetic resonance imaging (Cholangio-MRI) has led to the diagnosis of gallbladder agenesis. No hepatic or pancreatic abnormalities, the GB couldn’t be found in its normal site, or in an ectopic place. Endoscopic retrogradeCholangio-Pancreatography with sphincterotomy was done to extract the GB stones and to confirm the diagnosis GB agenesis. The evolution has been marked by the improvement of jaundice and the stabilization of laboratory findings.
Benhbelbardadi I and Pr Ajana FZ
C, Ibn Sina Hospital, Hay El Chbanate N 153 City Yacoub El Mansour, Morocco, Tel:
0658212007; Email: Saednawal01@hotmail.com
jaundice and the stabilization of laboratory findings.
Keywords: Jaundice; Gallbladder; Agenesis; Endoscopic Retrogradecholangio-Pancreatography
Introduction
Gallbladder agenesis is an extremely rare congenital anomaly. Their diagnosis is usually carried out intraoperatively. The ultrasound often describes a gallbladder (GB) atrophy, which can lead to unnecessary and potentially dangerous surgery. We report the case of a 45-year-old patient with no history of Cholecystitis, with cholestasis jaundice and whose ultrasound diagnosis of gallbladder agenesis was questioned. Magnetic resonance imaging resulted in the diagnosis of gallbladder agenesis, which was confirmed by the Endoscopic Retrograde Cholangio-Pancreatography (ERCP).
Objective
To present a clinical case of agenesis of the gallbladder diagnosed by US examination following a cholestasis jaundice.
Clinical Cases
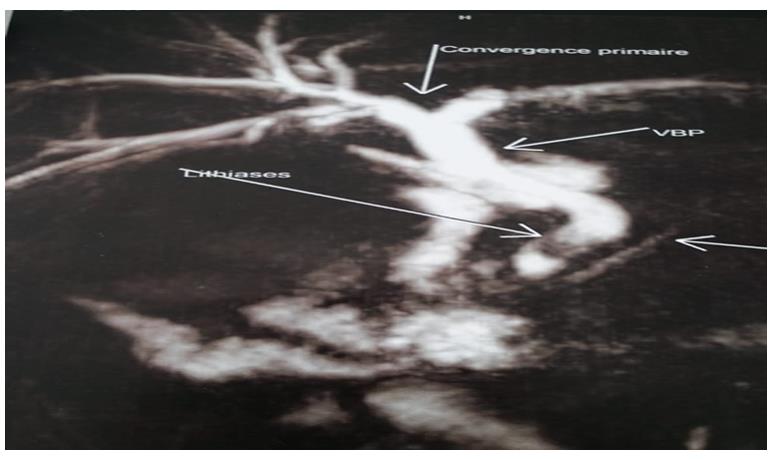
It is a 45-year-old, married, father of four children, with no personal or a relevant family history, no history of drug taking; it is a patient who has been addressed to us by her doctor treat for taking care of her cholestasis, without biliary colic or fever. The clinical examination of the abdomen is normal, and the gallbladder is not palpable. Biological (hematological and chemical) examination showed objectively hepatic injury and cholestasis with a bilirubin of 25mg/L without liver cell failure. A serology has been requested (Viral hepatitis B, Viral hepatitis C, Anti-mitochondrial antibodies type 2 (AM2), autoimmune profile) which is strictly normal. An abdominal ultrasound was performed showing a strictly normal liver, dilation of Biliary intrahepatic (IHBD) and common bile duct (CBD) to 12mm without visible obstacle, but GB was not seen (presence of gas). Magnetic
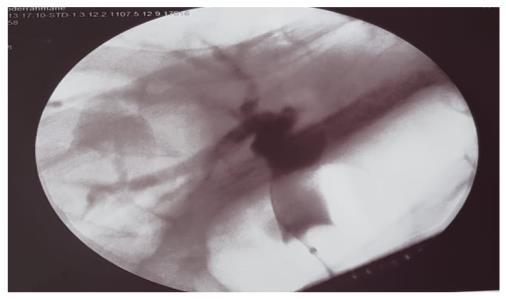
resonant cholangiopancreatography showed a dilation of IHBD and main bile duct to 12mm with 2 GB stones at the lower bile duct, measuring 8, 7mm and 7, 5mm (Figure 1), no hepatic or pancreatic abnormalities, the GB couldn’t be found in its normal site , or in an ectopic place. Endoscopic retrogradeCholangio-Pancreatography with sphincterotomy was done to extract the GB stones and to confirm the diagnosis GB agenesis (Figure 2). The evolution has been marked by the improvement of jaundice and the stabilization of laboratory findings.
Discussion
The first case of gallbladder agenesis was described by Bergman in 1701. The incidence of autopsy discovery in adults ranges from 0.013 to 0.075% with an equal proportion in men and women, but clinical cases are more common in women [1, 2, 3, 4].
The number of cases of gallbladder agenesis reported up to 1988 is 393 cases per dumpster and since that date
20 new cases have been added [4]. Of these, 1 case considered among the group of multiple fetal anomalies, and died, like the others, in the peri-natal period. Two cases correspond to the asymptomatic group of autopsy findings. The other 17 cases became part of the group at clinical manifestations and were discovered during the laparotomy or laparoscopy [5, 6, 7, 8].
Embryo logically, the extra hepatic bile ducts develop from the anterior intestine, at the level of the ventral pancreas. The first physiological hypotheses suggested an anomaly of vascularization of the vesicular trunk explaining its absence [9]. More recently, it has been showed that genetic transcription factors were needed for the development of the gallbladder: Sox 17+, PDX 1+, HNF6, HNF1b located respectively on chromosomes 8,13,15 and 17. In a murine model, their absence resulted in agenesis of the GB and other bile tract anomalies.
In this context, Benner, et al. has established a classification to distinguish 3 groups of GB agenesis: a) Group of multiple fetal anomalies (12.9%): These patients usually die in the perinatal period due to other malformations, the absence of gallbladder is only observed at the autopsy [9, 10]. Cardiovascular malformations are the most common, followed by those of gastrointestinal and genitourinary systems. b) Asymptomatic group (31.6%): This group of patients without gallbladder is most often found at the “autopsy or during” an intervention. None of these patients have any biliary symptoms. c) Group with clinical manifestations, symptomatic form (55.6%): This group corresponds to the age range of 40 to 50 years, usually without other congenital anomalies Among the patients carrying this anomaly, 23% developed symptoms [11, 12, 13, 14, 15, 16]. Right hypochondrial pain (90% of cases), nausea or vomiting (66%), intolerance to a diet rich in fat (38%), dyspepsia (30%), choledocholithiasis. Twenty-two percent of patients have a major dilated CBD, but only 27% of them have CBD stones (case of our patient). These symptoms may be attributed to a biliary dyskinesia and assimilated to the post-cholecystectomy syndrome [17]. An increase in the pressure of the sphincter of Oddi would promote biliary stasis and dilation of bile. Similarly, the latter could be explained by the fact that the main bile duct is substituted for the GB.
The diagnosis of GB agenesis is difficult to establish, because rare and therefore little known. It is often established when the surgical exploration indicated for atrophic GB. Currently, ultrasound is the reference exam to explore the biliary pathways. Ultrasound performed in a context of biliary colic often concluded with the presence of atrophic GB. The air in the duodenum gives a sub hepatic hyper dens image making this error in the interpretation. Nevertheless, according to Hammond [13], even in the case of atrophic GB, there is always a fine bile shadow for identifying the GB. Moreover, this situation, which is linked to the repetition of Cholecystitis episodes, is unlikely in the child. In case of diagnostic doubt in a child, MRCP allows accurate analysis of the entire bile duct and confirms the agenesis [18, 19, 20, 21]. A vesicle should also be removed if in the ectopic position (to the left of the ligament, intrahepatic, retro hepatic, Retroduodnal or Retro pancreatic). In the absence of pre surgical diagnosis, symptomatic patients are operated for cholecystectomy and the diagnosis is restored. However, in the intra operatively, the not well trained surgeon may seek a GB in an ectopic position, to dissect the hepatic pedicle without the usual anatomical clues, exposing to injury of the CBD [22]. It is therefore important to mention this diagnosis in case of doubt. In adults, if the diagnosis is made before any surgery, an anti-spasmodic treatment can be proposed to symptomatic patients.
Conclusion
The agenesis of the gallbladder is well known but it produces a rare congenital anomaly. Sila Gall bladder is not visualized in its normal site; this anomaly should be strongly suspected. If during the c laparoscopy, the examination of all ectopic locations is not feasible, the conversion by a surgical laparotomy to identify the eventual ectopic localizations require a wide surgical dissection exhibiting to decay; and if that clinical conditions do not threaten the life of the subject, it is preferable for these reasons to suggest, a surgical laparotomy, and other investigations like ERCP and abdominal ct.
References
-
Serralta de Colsa D, Arjona Medina I, QuirósHigueras E, Sanz Sánchez M, Pérez Díaz MD, et al. (2006) Gallbladder agenesis: Diagnosis of a case without surgery. Rev Esp EnfermDig 98(12): 964-968.
-
Singh B, Satyapal KS, Moodley J, Haffejee AA (1999) Congenital absence of the gallbladder. Surg Radiol Anat 21(3): 221-224.
-
Guillermo J, Valencia F, Noemí S (2012) Agenesia vesicular: reporte de caso. Rev Med Inst Mex Seguro Soc 50(1): 63-66.
-
Muguruma N, Okamura S, Ichikawa S, Tsujigami K, Suzuki M, et al. (2001) Asymptomatic case of congenital absence of gallbladder. J Med Invest 48(1- 2): 118-121.
-
Beuran M, Păun S, Negoi I, Gănescu R, Runcanu A, et al. (2010) Laparoscopic approach in gallbladder agenesis-an intraoperative surprise. Chirurgia (Bucur) 105(4): 531-136.
-
Leone V (2011) Isolated Agenesis of the Gallbladder: A Pitfall in Laparoscopic Cholecystectomy. Webmed Central 2(12): 1-7.
-
Malde S (2010) Gallbladder agenesis diagnosed intra- operatively: a case report. J Med Case Rep 4: 285.
-
Singh S, Tayal A, Kaur V (2011) Mystery of absent gallbladder: Surgical concerns and review of literature. JIMSA 24(2): 71.
-
Lamah M, Karanjia ND, Dickson GH (2001) Anatomical variations of the extra hepatic biliary tree: review of the world literature. Clin Anat 14(3): 167- 72.
-
Mu˜noz HJ, Quirarte CC, Arribas MA, Góngora SM, Cruz RO, et al. (2011) Agenesia de vesículabiliar. Reporte de caso y revisión de laliteratura. Rev Mex CirEndoscop 12(1): 35-37.
-
Gaxiola WR, Gómez GNG, Alcántara MFJ, Valero OUJ (2000) Vesicular agenesis and choledocholithiasis. Presentation of a patient. Cir Gen 22(4): 362-366.
-
Flores Valencia JG, Vital Miranda SN, Mondragón Romano SP, dela Garza Salinas LH (2012) Vesicular agenesis: case report. Rev Med Inst Mex Seguro Soc 50(1): 63-66.
-
Peloponissios N, Gillet M, Cavin R, Halkic N (2005) Agenesis of the gallbladder: A dangerously misdiagnosed malformation. World J Gastroenterol 11(39): 6228-6231.
-
Böyük A, Kırkıl C, Karabulut K, Sözen S, Demirelli S (2012) A choledochal cyst resulting in obstructive jaundice in a case with gallbladder agenesis: report of a case and review of the literature. Balkan Med J 29: 106-108.
-
Cockbain AJ, Watson J, Toogood GJ (2011) Hepatobiliary and Pancreatic: Agenesis of the gallbladder. J Gastroenterol Hepatol 26(5): 935.
-
Lehman GA, Sherman S (1996) Sphincter of Oddi dysfunction. Int J Pancreatol 20(1): 11-25.
-
Elorza Orúe JL (2001) Agenesis of the gallbladder. Presentation of a case studied by RM- cholangiography Cir Esp 69(4): 427-428.
-
Fiaschetti V, Calabrese G, Viarani S, Bazzocchi G, Simonetti G (2009) Gallbladder agenesis and cystic duct absence in an adult patient diagnosed by magnetic resonance cholangiography: report of a case and review of the literature. Case Report Med.
-
Chowbey PK, Dey A, Khullar R, Sharma A, Soni V, et al. (2009) Agenesis of gallbladder: our experience and a review of literature. Indian J Surg 71(4): 188-192.
-
Cano Valderrama O, Talavera P, Domínguez Serrano I, Sánchez Pernaute A, Torres García AJ (2011) Gallbladder agenesis: presentation of a case. Cir Esp 89(7): 471-472.
-
Amadon PD (1933) Agenesis of the gallbladder associated with pancreatitis: report of a case. The American Journal of Surgery 19(2): 263-267.
-
Kabiri H, Domingo OH, Tzarnas CD (2006) Agenesis of the gallbladder. Curr Surg 63(2): 104-106.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient