Chylous Ascites: A Rare Entity
Chylous ascites is a distinct and rare entity. Diagnosis of chylous ascites is by milky white appearance of the ascitic fluid with triglyceride content more than 200 mg/dl. We present a case of chylous ascites due to Non Hodgkin`s Lymphoma where the diagnosis was missed in another tertiary hospital.
Case
MFS a 34year non-alcoholic male patient presented with Progressive abdominal distension for last one year, Painless. Associated pedal oedema. No vomiting, gastrointestinal bleeding, Bowel / bladder habits normal. No history of jaundice. No surgeries in past. Was being treated as Tuberculous ascites in another hospital without relief hence came for second opinion.
He looked ill and cachexic, weighed 53 kg, vital signs were normal. Left axillary central group and bilateral inguinal lymph nodes were enlarged, non-tender. He was pale, had bipedal pitting oedema. No icterus or signs of chronic liver disease. Abdomen was distended, no visible veins or lump. There was gross ascites and organomegaly was difficult to assess due to tense ascites. He had right pleural effusion. There was ejection systolic murmur in mitral area.
His earlier investigation had showed intraabdominal, multiple necrotic lymph nodes, IC junction and ileal thickening, gross ascites, bilateral pleural effusions on USG and CT abdomen. Fluid examination had shown 1000 cells/cu mm with 90 % lymphocytes, no abnormal cells. Total protein 1.8 gm/dl with albumin of 1.1 and SAAG of 1.8. He was negative for HBV, HCV, HIV. CA19-9, CA125, αFP, PSA were normal. His liver and kidney function tests were normal.
He was reinvestigated at our centre and was found to have Lymph node mass in central abdomen, honeycomb appearance of spleen (Figure 1), bilateral pleural effusions on USG. His serum β2 microglobin was grossly elevated at 7626 and LDH was 238. Ascitic fluid was grossly milky (Figure 2) and was found to have cholesterol < 45, Triglycerides 1100 mg/ dl and ADA 20 IU. No abnormal cells on cytology. Upper Gi endoscopy revealed duodenal lymphangiectasia with visible oozing of lymph. Biopsy of distal duodenal mucosa confirmed intestinal lymphangiectasia (Figure 3). Inguinal lymph node biopsy revealed grade IIIA Non-Hodgkin`s Lymphoma follicular type. Tumour cells were positive for CD20, CD10, BCL 2, BCL 6, negative for CD3. Mib 1 index 30%. Patient was put on chemotherapy R-CHOP six cycles and made good recovery. Ascites disappeared. He was advised maintenance Rituximab for two years.
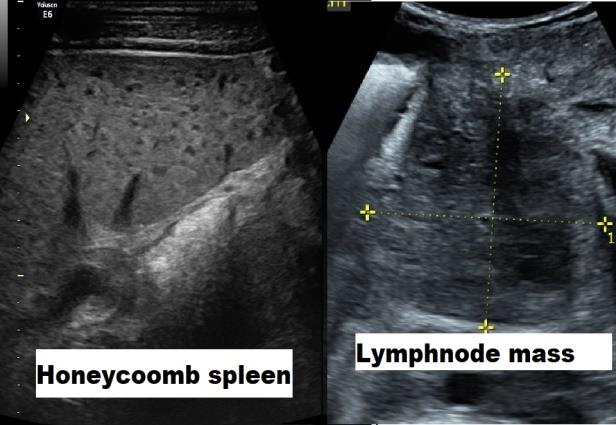
A: Honey-comb appearance of spleen B: Central abdominal lymph node mass


Discussion
Chylous ascites is a rare entity and is a manifestation of some underlying disease pathology rather than a diagnosis by itself. The incidence of chylous ascites was reported to be 1:20,000 hospital admissions at Massachusetts general hospital in 1990 [1]. However recently the incidence has increased probably due to prolonged survival of the cancer patients and due to more aggressive surgical techniques and laparoscopic interventions and transplantations [2, 3]. Chylous ascites accounts for less than 1 % of all of ascites patients. The prognosis is generally poor as majority of adult cases are due to malignancy or advanced cirrhosis of liver.
Aetiology of chylous ascites differs in adults and children. In children it is mainly due to congenital causes like congenital lymphangiectasia, mesenteric cyst, or part of various syndromes like Turner / Klippel Trenaunay or yellow nail syndrome [2]. In adults, causes can be divided into portal hypertension related or unrelated [4]. Non portal hypertension related causes are generally due to various malignancies like lymphoma, disseminated carcinomatosis of various malignancies like pancreas, ovary, testis, hepatoma, breast, colon, prostate etc. In these cases, blockage of lymphatics causes rupture and leakage of chylous fluid in the peritoneum. Chylous ascites is seen in approximately 0.5 % of cirrhotic patients and is due to portal hypertension with exudation of chyle from space of Disse due to portal hypertension [5]. Infections like tuberculosis or filariasis also can cause chylous ascites especially in tropical countries. Other causes include retroperitoneal fibrosis, pelvic irradiation, blunt abdominal trauma, peritoneal dialysis and post-operative chylous ascites. The causes are summarized in Table 1.
| Congenital lymphatic | |||||
|---|---|---|---|---|---|
| Cirrhosis of Liver | |||||
| disorders | |||||
| Blunt abdominal trauma | Disseminated carcinomatosis | ||||
| Lymphoma | Infections: Tuberculosis, Filariasis | ||||
| Pelvic irradiation | Retroperitoneal fibrosis | ||||
| Post-operative |
Table 1: Causes of chylous ascites.
The chylous nature of ascites is diagnosed by demonstrating grossly milky ascitic fluid which has Triglycerides > 200 mg/dl [3, 6]. The ascitic fluid to serum triglycerides ratio is in the range of 2:1 to 8:1. Generally fluid has high protein content and SAAG may be high if the underlying cause is Cirrhosis of Liver. Fluid Cholesterol is generally low. ADA is high if there is tuberculosis. Fluid cytology can show abnormal cells and fluid cytology has been reported to have a sensitivity of 62.4 % and specificity of 98 % with a positive predictive value of 100 % and negative predictive value of 88 %. Fluid cytology yield can be improved by using immunohistochemistry [7]. At least 100 ml fluid is required for cytology.
The underlying aetiology assessment may require imaging studies lymph node biopsy, laparoscopy with peritoneal biopsy or occasionally lymhangiography depending on the underlying pathology.
Treatment and prognosis depend on the underlying aetiology. Diuretics, TIPS, Peritoneo-venous shunts repeated paracentesis have been described depending on the underlying cause. For patients with lymphoma or disseminated carcinomatosis chemotherapy depending on underlying pathology is needed. However, prognosis is often dismal. For portal hypertension related chylous ascites salt restriction, diuretics, Somatostatin or Octreotide, TIPS have been used [3]. If a definite leak is identified, Lymhangiographic embolization or surgery is used to tackle the leak.
Dietary modification with use of Medium Chain Triglycerides has been found useful. MCT are absorbed directly into portal circulation and bypass the intestinal lymphatics hence reduce the lymph production [3, 6]. Coconut oil is rich source of MCT however can have palatability and tolerance issues. TPN can be a short-term alternative when the aetiology is correctable by some means.
Conclusion
Chylous ascites is a rare entity usually associated with underlying serious diseases. Prognosis is generally dismal as nearly two third of cases are associated with advanced malignancies or advanced Cirrhosis of Liver. Mortality at one year is approximately 40 - 70 % depending on underlying aetiology [2].
This case also signifies the importance of relook approach when the patient is not responding to the treatment. The diagnosis of Chylous nature of ascites and its underlying aetiology was missed in a tertiary university hospital.
References
-
Browse NL, Wilson NM, Russo F, al-Hassan H, Allen DR (1992) Aetiology and treatment of chylous ascites. Br J Surg 79: 1145-1150.
-
Aalami OO, Allen DB, Organ CH (2000) Chylous ascites: a collective review. Surgery 128(5): 761-778.
-
Cárdenas A, Chopra S (1900) Chylous ascites. Am J Gastroenterol 97(8): 1896-1900.
-
Bhardwaj R, Vaziri H, Gautam A, Ballesteros E, Karimeddini D, et al. (2018) Chylous Ascites: A review of pathogenesis,diagnosis and treatment. Journal of clinical and translational hepatology 6(1): 105-113.
-
Witte MH, Witte CL, Dumont AE (1971) Progress in liver disease: physiological factors involved in the causation of cirrhotic ascites. Gastroenterology 61(5): 742-750.
-
Almakdisi T, Massoud S, Makdisi G (2005) Lymphomas and chylous ascites: review of the literature. Oncologist 10(8): 632-635.
-
Motherby H, Nadjari B, Friegel P, Kohaus J, Ramp U, et al. (1999) Diagnostic accuracy of effusion cytology. Diagn Cytopathol 20(6): 350-357.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient