The Expected Pandemic of Mild-Alzheimer (≈Type 3 Diabetes), How to Combat?
With the increasing aging of the world population, the share in the population with mild Alzheimer's (m-ADs) - also referred to as type-3 diabetes - is increasing. Rough estimates indicate that by 2050 around 140 million people will suffer from this disease, especially in developed countries. m-ADs can be characterized by senile plaques that consist of extracellular amyloid beta (Aβ) deposition while neurofibrillary tangles (NFT) consisting of hyperphosphorylated tau which are located intracellular in Alzheimer Diseased brain. It must be emphasized that these are the consequences of the disease and not the cause. These amyloid plaques have also been observed in other organs of patients with poorly treated type 2 diabetes such as pancreas, liver, kidney and heart, so it must be emphasized that they are not characteristic of the brain alone. But what is then consequently the cause of m-ADs? The idea was first that the brain produced Insulin to a lesser extent but a "breakthrough" study LC-MS by van Ginneken, et al. indicated that in post mortem Type Diabetes brain donors there more saturated bonds occur, making the brain more rigid and the Insulin molecule less likely to reach its destination, leading to neural death. A second hypothesized cause is the formation of plaques in the fluid mosaic membrane of poly unsaturated fatty acids (PUFAs), as a result of which the Insulin molecule is less able to penetrate the human brain, which also leads to neural death. Finally, the role of Sphingomyelins as lipids in foods such as soy and milk should be mentioned, which can be converted via the Land's cycle in the brain to toxic ceramide, which also could lead to neural death. In addition, in a small cohort of patients from the Dutch brain bank - where post mortem histopathological the brain disease has been assessed in addition to body characteristics - it appears that m-ADs or also Type-3 Diabetes is independent of Body Mass Index (BMI).
Vincent van Ginneken* and Floris Schouten
Bluegreen Technologies, Heelsum, Netherlands
Body Mass Index (BMI).
Index (BMI).
Perspective
Introduction
There were an estimated 46.8 million people worldwide living with dementia in 2015 and this number is believed to be close to 50 million people in 2017. This number wills almost double every 20 years, reaching 75 million in 2030 and 131.5 million in 2050. Much of this increase towards 2050 will be in Low- and Middle-Income countries (figure 1), [1].
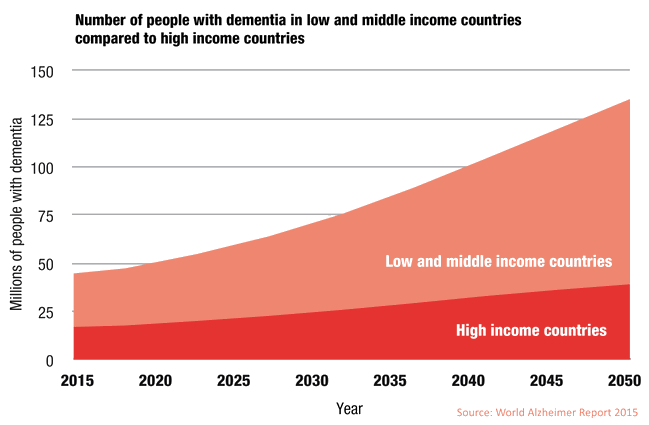
Alzheimer’s disease is the most common type of dementia, with a prevalence that varies from about 3% in individuals around 65 years of age to nearly 50% in people aged ≥ 85 years. The World Alzheimer report 2018 highlights an urgent need for increased and sustainable funding for dementia research. The global ratio of publications on neurodegenerative disorders, versus cancer, is an astonishing 1:12. The number of people with Alzheimer’s disease/Dementia is the highest in High income Countries (Figure 1), but data are scarce and projections of the World Alzheimer Report [1] figure 1 show an increased morbidity in Low- and Middle-income countries towards 2050. For a High-income country the United States, an estimated 5.7 million Americans have Alzheimer’s dementia. By mid-century, the number of people living with Alzheimer’s dementia in the United States is projected to grow to 13.8 million, fuelled in large part by the aging baby boom generation. In 2015, official death certificates recorded 110,561 deaths from AD, making AD the sixth leading cause of death in the United States and the fifth leading cause of death in Americans age ≥ 65 years. Without doubt mild-Alzheimer’s Disease (m-AD) is a typical elderly disease (Figure 2). In 2018 the global societal cost was estimated around US$1 trillion [2].
![Figure 2: Alzheimers Disease and Figures 2018 [2].](/fulltextimages/4137/fig_2.png)
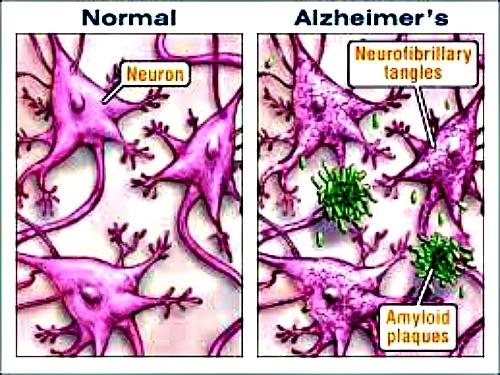
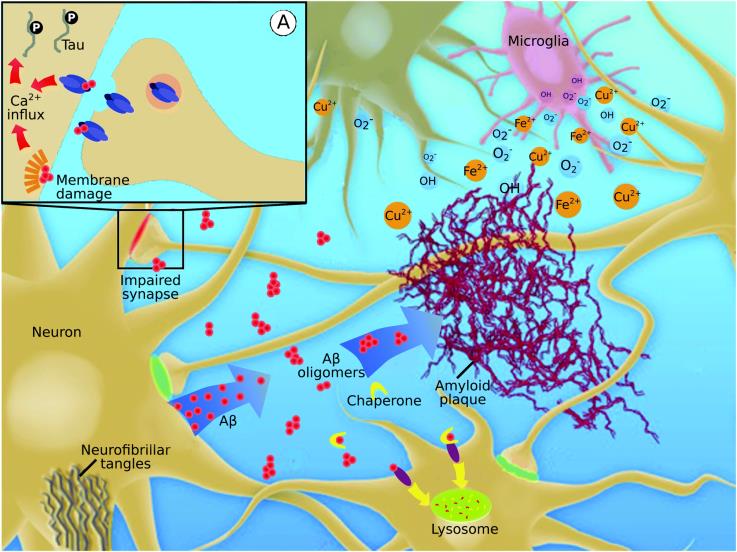
Alzheimer's disease (AD) has characteristic neuropathological disorders including regionalization neurodegeneration, neurofibrillary tangles, amyloid beta (Aβ) deposition, activation of pro-apoptotic genes, and oxidative stress. Because the brain functions continue to disintegrate, there is a decline in the person's cognitive skills, memory, state of mind, spontaneity and socializing behavior. A framework that sequentially connects all these phenomena is missing under one event.
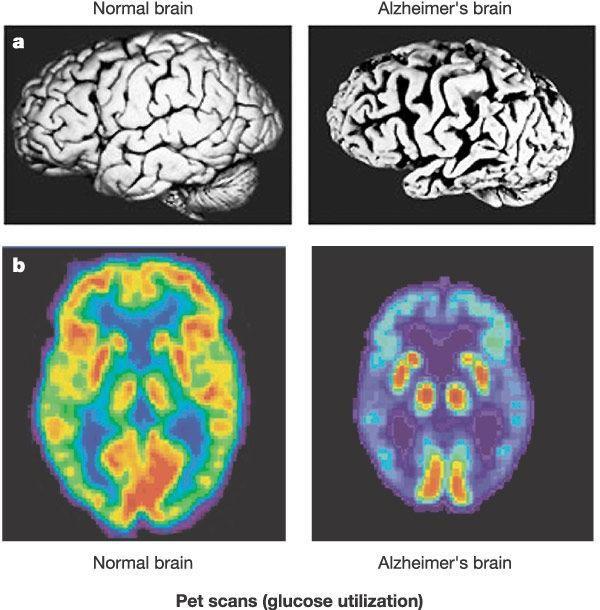
mediators of AD neurodegeneration and neurotoxicity of Sphingomyelins (SPMs) by conversion to the toxic compound Ceramide (see §5). In this, the research group of Neth & Craft [4] has indications from the development of an AD animal model caused by diabetes. Striking evidence has attributed the loss of Insulin receptor bearing neurons that precede or accompany the initial phase of AD. This condition seems to be progressing with AD in such a way that, in the end stages, it is getting worse and becoming global in the whole brain (Figure 3). Alzheimer’s disease can be characterized by extracellular senile amyloid plaques and intracellular neurofibrillary tangles (NFT), (Figure 4).
Here we will postulate a Systems Biology [3], lipidomics based hypothesis. Gathering evidence has the role of Insulin deficiency and Insulin Resistance (IR) as
How type 2 diabetes and Alzheimer are’s linked?
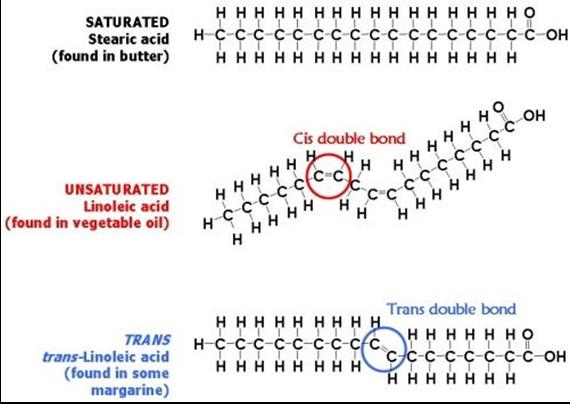
The cause of Alzheimer’s in itself is not well enough understood at present, and the link between Alzheimer’s and diabetes therefore, is also not clear. However, the two conditions seem to be linked and people who are over 60 years with type-2 diabetes are thought to be twice as likely to develop Alzheimer’s than those without diabetes. One reason why Alzheimer’s may be more prevalent in people with type-2 diabetes is that diabetes can damage the small blood vessels which feed cells and nerves. Damage to these blood vessels can therefore lead to damage to the cells and nerves they nourish. If brain cells are damaged in this way, Alzheimer’s can result. This was the general assumption about the disease some fifteen years ago. It came about in 2005 when a team led by Prof. Dr. Suzanne de la Monte at US Brown Medical School came across a remarkable diabetes breakthrough. The perception two decades ago was that our brains produce Insulin and that it is very important to our brain health. She wrote, “that neurons ‘degenerate’ when Insulin is reduced”. ‘Degenerate’, means that they die. When they die, memory loss begins along with other cognitive function failure. In fact -to our awareness- the brain cannot produce Insulin, but due to the number of more double bonds in the "trans" formation, the Insulin molecule is less able to invade the neo-cortex, leading to neural death (see below Table 1). Research further indicated that Insulin Resistance (IR) -like that found in type 2-diabetes- may also be found in those suffering from type-3 diabetes.
Deformation of the ‘Fluid Mosaic Membrane’ by Protein Deposits (Amyloid Plaques) Forming ‘Rafts’
Another big link is found in protein deposits (amyloid plaques). People with severe uncontrolled type-2 diabetes can also have protein deposits (≈IAPP=Islet Amyloid Poly-Peptide) in their pancreas Cooper, et al. [5] or even other organs such as numerous non-pancreatic tissues, including kidney (diabetic nephropathy), sensory neurons (diabetic neuropathy) and heart (diabetic cardiomyopathy) Mukherjee et al. [6] just like in the brain. This is an important observation from which we can conclude that the IAPP-plaques often characterized as a feature for mild-Alzheimer disease (m-AD) are a consequence of a low Insulin level reaching the target organ.
Another theory that explains why Alzheimer's disease occurs is the formation of plaque that sticks to the phospholipid bilayer of brain neurons. These plaques obstruct block communication between the brain neurons, which ultimately leads to neural death and in turn cause the symptoms of Alzheimer's disease (ADs) (Figure 5), [7].
By far, the biggest impact ‘Journal Alzheimer’s Disease’ had in relation to own research was the publication of a 6- manuscript series in 2005 and 2006, including: 1) a review article on the expression and function of Insulin and Insulin-like growth factor (IGF) signalling networks in the brain [8]; 2) the first primary research article demonstrating brain Insulin Resistance and Insulin deficiency in AD [9]; 3) a follow-up report showing AD Braak-stage dependent declines in Insulin and IGF signalling molecule expression and function in the brain [10]; 4) characterization of AD Braak stage-associated increases in brain oxidative stress and mitochondrial dysfunction, paralleling declines in Insulin/IGF signalling network functions [11]; 5) neuropathological and molecular characterization of the Intra-Cerebral streptozotocin (IC-STZ) model and its relevance to sporadic forms of human AD [12]; and 6) the demonstration that AD-type neurobehavioral deficits and neuropathology in the IC-STZ model could be prevented by treatment with peroxisome proliferator-activated receptor (PPAR) agonist-Insulin sensitizer drugs [13]. These lines of Type 3 Diabetes casu quo Alzheimer disease published in ‘Journal Alzheimers Disease’ of this 6- manuscript series in 2005 and 2006 was recently reviewed by de la Monte, et al. [14].
The majority of putative disease-modifying treatments in development for Alzheimer’s disease are directed against the amyloid-β(Aβ) peptide. Among the anti-Aβ therapeutic approaches, the most extensively developed is immunotherapy—specifically, passive immunization through administration of exogenous monoclonal antibodies (m-Abs) [15]. However, another approach based on another diagnosis of mild-Alzheimer seems to more effective. Based on the observations of Oxidative stress, tau hyperphosphorylation, Amyloid Precursor Protein -Amyloid-beta (APP-Aβ) deposition (Figure 4), and impaired glucose and energy metabolism these expressions of the pathogenesis have all been coupled with disruption of Insulin / IGF signaling. Based on these observations, it is concluded that Alzheimer’s Disease could be referred to as '' type 3 diabetes '' [16]. In addition, because of the common pathophysiology with type-2 diabetes common therapeutic regimen can be effective for Alzheimer’s Disease patients. Another option is related to lifestyle patterns (avoidance sedentary lifestyle, no alcohol and tobacco) [13].
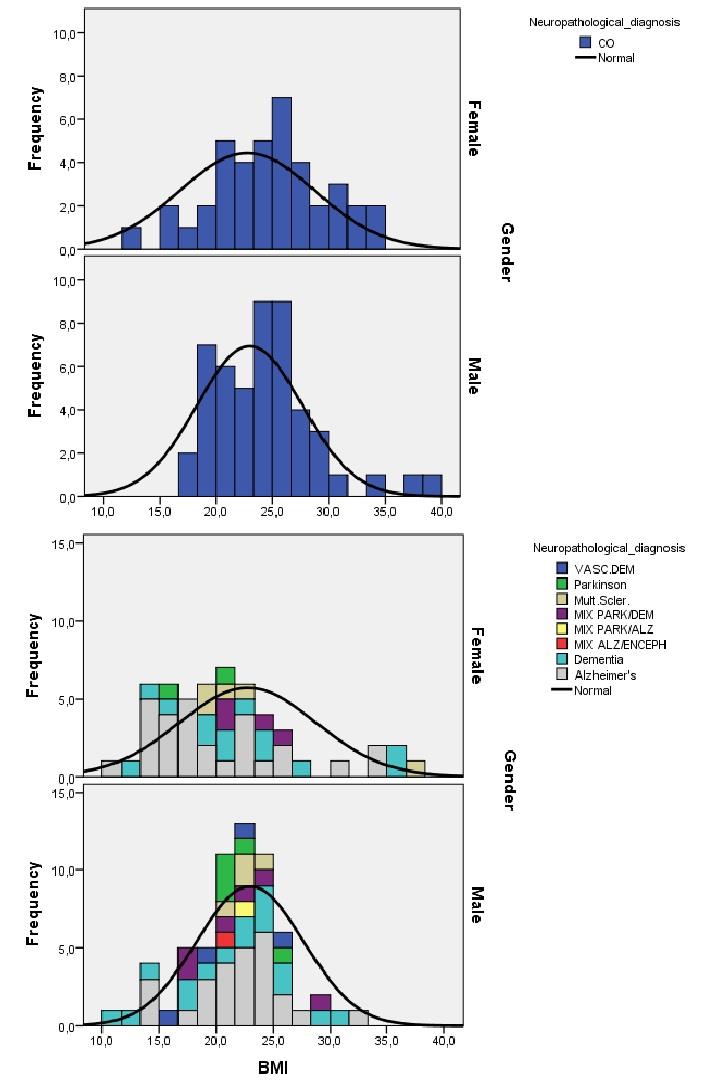
The Inability of the Fluid Mosaic Membrane to Transport E.G. The Important Molecule Insulin in the Brain - Due a Higher Degree of Unsaturation (≈ More Double Bonds) In an earlier landmark study [17], we investigated lipid profiles of brain of post mortem type 2 diabetes patients (T2DM) elderly patients in comparison to a Control group (Co) of the “Netherlands Brain Bank” using LC-MS techniques. We reported that brains of these T2DM patients contained more double bonds and consequently were more rigid (Figure 6). In a small cohort (≈200 patients) we proved that these brain diseases are not interrelated with BMI so obesity is not a major cause (Figure 7). The predicted wave of brain diseases of mild- Alzheimer (m-AD), dementia and depression of the “baby boom generation” might be evolved due to the “fatty” and more “rigid” brain structure due to the quality of fats eaten during earlier lifespan. Our major conclusion is that diabetes and its treatment among T2DM patients are more associated with structural disturbances (lipid composition) in the brain (Table 1) than with glycaemic control. Therefore, we introduced the new terminology “Type-3 diabetes” (T3DM) referring to the mental disorders as a consequence of a disordered lipid metabolism in the human brain related to higher degree of unsaturated fatty acids composition. Important to notice is that T3DM is not related to Body Mass Index (BMI) (figure 7) [17].
| Lipid | Number | Red matter | White matter | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comp. | C-atoms | control(A) | diabetes(B) | control (C) | diabetes(D) | A vs B | C vs D | ||||||||
| LPC | C : 18 | 206.3 ± 23.43 | 235.1 ± 25.80 | 92.6 ± 32.68 | 120.8 ± 46.20 | 0.035* | 0.183 | ||||||||
| SPM | C : 23 | 6.6 ± 5.65 | 8.00 ± 10.82 | 166.0 ± 67.11 | 185.4 ± 101.78 | 0.752 | 0.66 | ||||||||
| C : 24 | 15.7 ± 8.11 | 14.9 ± 3.47 | 30.7 ± 9.92 | 31.6 ± 13.15 | 0.826 | 0.882 | |||||||||
| C : 25 | 13.8 ± 3.12 | 16.3 ± 2.73 | 41.3 ± 15.25 | 44.8 ± 19.29 | 0.105 | 0.691 | |||||||||
| DG | C : 34 | 35.3 ± 6.48 | 36.0 ± 13.11 | 12.2 ± 3.88 | 13.6 ± 4.52 | 0.893 | 0.511 | ||||||||
| PC | C : 32 | 277.7 ± 31.56 | 259.4 ± 25.29 | 109.9 ± 34.27 | 115.1 ± 53.53 | 0.224 | 0.819 | ||||||||
| C : 34 | 18.9 ± 1.09 | 18.61± 0.78 | 6.7 ± 2.77 | 6.9 ± 4.70 | 0.507 | 0.889 | |||||||||
| PE | C : 34 | 46.3 ± 3.00 | 48.0 ± 5.45 | 45.2 ± 4.32 | 47.1 ± 4.86 | 0.452 | 0.422 | ||||||||
| ChE | C : 16 | 58.2 ± 7.31 | 67.0 ± 10.07 | 54.2 ± 7.07 | 70.1 ± 9.07 | 0.068 | 0.002 | ||||||||
| C : 18 | 38.3 ± 6.05 | 33.9 ± 5.64 | 34.3 ± 10.26 | 35.8 ± 5.48 | 0.151 | 0.727 | |||||||||
| TG | C : 48 | 61.5 ± 12.80 | 57.2 ± 11.47 | 54.7 ± 19.26 | 49.7 ± 13.08 | 0.493 | 0.555 | ||||||||
| C : 50 | 26.7 ± 4.37 | 20.5± 5.31 | 23.4 ± 5.72 | 16.6 ± 5.74 | 0.024* | 0.033* |
Table 1: Saturation Degree according to (18. Hulbert et al 2005) of the several lipid compounds of human post-mortem neo-cortical
Sphingomyelines (Spms) and its Interconversion Towards Toxic Ceramide Cause Neural Death and AD
Sphingomyelin (SPM) is a sphingolipid, located mostly in the outer layer of the plasma membrane.
This major lipid fraction has significant structural and functional roles in the cell. It is a plasma membrane component and participates in many signalling pathways. Ceramide is the second messenger in the sphingomyelin signaling pathway (Land’s cycle: Figure 8). Experimental studies revealed that Ceramide might impair Insulin action via: 1). maintaining protein kinase B in an inactive dephosphorylated state; 2). a reduction of GLUT4 translocation to plasma membrane; 3). a decrease in Insulin-stimulated glucose uptake; 4). Tumor Necrosis Factor (TNF)-α, a well-known mediator of Insulin resistance, acts through activation of neutral sphingomyelinase (enzyme which hydrolysis sphingomyelin => Ceramide) and induction of Ceramide formation [19].
![Figure 8: Depicted are the interconversions and formation of sphingomyelin from phosphatidylcholine given and vice versa as described by Marggraff, et al. [20] in the Land’s cycle.](/fulltextimages/4137/fig_8.png)
Such is the case for the lipid Sphingomyelin. This is a type of sphingolipid found in animal cell membranes, especially in the membranous myelin sheath that surrounds some nerve cell axons. It usually consists of phosphocholine and Ceramide, or a phospho- ethanolamine head group; therefore, sphingomyelins can also be classified as SphingoPhospholipids (SPH). In humans, SPH represents ~85% of all sphingolipids, and typically make up 10-20 mol % of plasma membrane lipids. Sphingomyelins contain phosphocholine or phospho-ethanolamine as their polar head group and are because of this characteristic classified along with glycerophospholipids as phospholipids. Indeed, sphingomyelins resemble phosphatidylcholines in their general properties and three-dimensional structure, and in having no net charge on their head groups. Sphingomyelins are present in the plasma membranes of animal cells and are especially prominent in myelin, a membranous sheath that surrounds and insulates the axons of some neurons—resulting in the name “sphingomyelins” reviewed [21]. The metabolism of sphingomyelin creates many products that play significant roles in the cell. Sphingolipids are hydrolyzed in the gastrointestinal tract to Ceramide, sphingosine, and other metabolites that can modulate cell growth, differentiation, and apoptosis. Although the sphingolipid content of foods has not been widely studied, several foods (e.g., milk and soybeans) contain the sphingolipid levels used in these investigations; therefore, this class of compounds could be significant contributors to incidence of Alzheimer’s Disease due to the entrance of sphingomyelins via the commodity of human foodstuff can pass the Blood Brain Barrier and enter the human brain where it via the Land’s cycle can be converted to the toxic compound Ceramide which causes neural death resulting in Alzheimer’s Disease. It would be an exciting hypothesis for further research that the sphingolipid content of foods -e.g., milk and soybeans, via Ceramide
resulting in neural death- could explain the predicted pandemics of Alzheimer’s disease (AD) in Low- and Middle-Income countries (Figure 1) [1].
Conclusions and Perspectives
1) What happens when there is a problem with the cell membrane’s ability to uptake/export important molecules or communicate like Insulin in the human brain? It might cause Alzheimer’s disease because of the inability of the fluid mosaic membrane to transport e.g. the important molecule Insulin in the brain -due a higher degree of unsaturation≈ more double bonds (figure 6 & Table 1) in order to regulate the glucose concentration and the inefficient fuelling of the brain which results in neural death. 2) Another theory explaining why Alzheimer’s disease occurs is the forming of plaque sticking to the phospholipid bilayer of the brain neurons. These plaques hamper block communication between the brain neurons, eventually leading to neural death and in turn causing the symptoms of Alzheimer’s Disease (ADs) (Figure 4) [5]. 3) Sphingomyelin, a major component of myelin membrane formed by mature oligodendrocytes, is abundant in the Central Nervous System (CNS) [21]. Ceramide, its primary catabolic product released by activation of either neutral or acidic sphingomyelinase, serves as a potential lipid second messenger or mediator molecule modulating diverse cellular signalling pathways but most important it is toxic and can cause cellular apoptosis Jaffrézou, et al. [22] via the the Land’s cycle Marggraff, et al. [20] resulting in neural death. 4) Sphingomyelins can also be taken up by the food (e.g. in milk and soybeans) and perform their harmful effects in the brain after passing the Blood Brain Barrier (BBB) and conversion towards toxic Ceramide via the Land’s cycle resulting in neural death and finally Alzheimer’s Disease (ADs). Indeed increased (Ceramide)- concentrations have been observed in brains of AD’s patients [23]. This topic is a rather unexplored neurological/nutritional research field!
References
-
World Alzheimers Report (2015) The Global Impact of Dementia, Analysis of prevalence, incidence, costs and trends, pp: 87.
-
Alzheimer’s Association (2018) Alzheimer’s Association Report: 2018; Alzheimer’s disease facts and figures’. Alzheimers’s & Dementia 14: 367-429.
-
Kitano H (2002) Systems Biology: a brief overview. Science 295(5560): 1662-1664.
-
Neth BJ, Craft S (2017) Insulin Resistance and Alzheimer's Disease: Bioenergetic Linkages. Frontiers in aging neuroscience 9: 345.
-
Cooper GJS, Aitken JF, Zhang S (2010) Is type 2 diabetes an amyloidosis and does it really matter (to patients)? Diabetologia 53(6): 1011-1016.
-
Mukherjee A, Morales-Scheihing D, Butler PC, Soto C (2015) Type 2 diabetes as a protein misfolding disease. Trends in molecular medicine 21(7): 439- 449.
-
Rushworth JV & Hooper NM (2010). Lipid Rafts: Linking Alzheimer's Amyloid-β Production, Aggregation, and Toxicity at Neuronal Membranes. International journal of Alzheimer's disease 2011: 14.
-
de la Monte SM, Wands JR (2005) Review of insulin and insulin-like growth factor expression, signalling, and malfunction in the central nervous system: Relevance to Alzheimer’s disease. J Alzheimers Dis 7: 45-61.
-
Steen E, Terry BM, Rivera EJ, Cannon JL, Neely TR, et al. (2005) Impaired insulin and insulin-like growth factor expression and signalling mechanisms in Alzheimer’s disease-is this type 3 diabetes? J Alzheimers Dis 7: 63-80.
-
Rivera EJ, Goldin A, Fulmer N, Tavares R, Wands JR, et al. (2005) Insulin and insulin-like growth factor expression and function deteriorate with progression of Alzheimer’s disease: Link to brain reductions in acetylcholine. J Alzheimers Dis 8: 247-268.
-
de la Monte SM, Wands JR (2006) Molecular indices of oxidative stress and mitochondrial dysfunction occur early and often progress with severity of Alzheimer’s disease. J Alzheimers Dis 9: 167-181.
-
Lester-Coll N, Rivera EJ, Soscia SJ, Doiron K, Wands JR, et al. (2006) Intracerebral streptozotocin model of type 3 diabetes: Relevance to sporadic Alzheimer’s disease. J Alzheimers Dis 9: 13-33.
-
de la Monte SM, Tong M, Lester-Coll N, Plater M Jr, Wands JR (2006). Therapeutic rescue of neurodegeneration in experimental type 3 diabetes: Relevance to Alzheimer’s disease. J Alzheimers Dis 10: 89-109.
-
de la Monte SM, Tong M, & Wands JR (2018) The 20- Year Voyage Aboard the Journal of Alzheimer's Disease: Docking at 'Type 3 Diabetes', Environmental/Exposure Factors, Pathogenic Mechanisms, and Potential Treatments. Journal of Alzheimer's disease: JAD 62(3): 1381-1390.
-
Van Dyck CH (2018) Anti-Amyloid-β Monoclonal Antibodies for Alzheimer’s Disease: Pitfalls and Promise. Biological Psychiatry 83: 311-319.
-
Kandimalla R, Thirumala V, Reddy PH (2017) Is Alzheimer's disease a Type 3 Diabetes? A critical appraisal. Biochimica et biophysica acta. Molecular basis of disease 1863(5): 1078-1089.
-
Ginneken VV, Vries E de, Verheij E, Greef JVD (2017) Type 3 Diabetes Reflects Disordered Lipid Metabolism in the Human Brain Related to Higher Degree of Unsaturated Fatty Acids Composition and is not Related to Body Mass Index. J Bioanal Biomed 9: 159-163.
-
Hulbert AJ, Turner N, Storlien LH, Else PL (2005) Dietary fats and membrane function: implications for metabolism and disease. Biol Rev 80(1): 155-169.
-
Straczkowski M, Kowalska I, Nikolajuk A, Dzienis- Straczkowska S, Kinalska I, et al. (2004) Relationship between insulin Sensitivity and Sphingomyelin Signalling Pathway in Human Skeletal Muscle, Diabetes 53: 1215-1221.
-
Marggraf WD, Anderer FA, Kanfer JN (1981) The formation of sphingomyelin from phosphatidylcholine in plasma membrane preparations from mouse fibroblasts, Biochim. Biophys. Acta (BBA)/Lipids Lipid Metab 664(1): 61-73.
-
Ridgway N & McLeod RS (editors) (2016) Book 6th (Edn.), Biochemistry of Lipids, Lipoproteins and Membranes, pp: 612.
-
Jaffrézou, JP, Levade T, Bettaïeb A, Andrieu N, Bezombes C, et al. (1996) Daunorubicin-induced apoptosis: triggering of ceramide generation through sphingomyelin hydrolysis. The EMBO journal 15(10): 2417-2424.
-
Filippov V, Song MA, Zhang K, Vinters HV, Tung S, et al. (2012) Increased ceramide in brains with Alzheimer's and other neurodegenerative diseases. J Alzheimers Dis 29(3): 537–547.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient