The Prognostic Value of Inflammatory Markers to Predict Adverse Clinical Course of Acute Pancreatitis
Background/Aim: Prognosis of complications is important in patients with acute pancreatitis (AP). The aim was to determine the severity of AP based on changes of inflammatory markers (IM). Material and Methods: WBC, immature granulocytes (IG), neutrophil-lymphocytes ratio (NLR) and the C-reactive protein (CRP) were compared in 243 patients with moderately severe pancreatitis (MSP) and in 59 patients with acute severe pancreatitis (ASP). Results: WBC count was significantly more in ASP compare to MSP group (15.4±2.3×109/l. vs. 12.7±1.2×109/l.). IG percentage was high in ASP group; however, lymphocytes count was lower in ASP. NLR during early 48 hours decreased in MSP; but significantly increased in ASP group. The “cut off” for NLR was determined as 10.5. 3-weeks survival in patients with NLI10.5 the survival was 79.2% and mortality raised up to 21.8%. IG in MSP group was 0.39±0.21% and 1.7±0.51% in ASP.CRP on admission was not differ between groups, but increased in ASP in 2nd day and was significantly higher compare to MSP. Conclusion: NLR can predict the survival on admission, but CRP only 2nd day achieve the predictive value. Rational evaluating of IM during early 2 days can predict the further clinical course of AP.
Introduction
Acute pancreatitis (AP) is the most common disease among population. Over the past two decades the incidence has increased from 15 to 45 per 100 000 populations [1, 2, 3].
The number of hospitalized patients with AP in the United States increased from 183 000 up to 275 000 in 1998-2009 years. In Europe the incidence of the AP is different: the lowest spread (17.5 per 100 000 populations) in Germany and the highest incidence (73.4 per 100,000 populations) in Finland were reported [3, 4, 5]. Revised Atlanta classification (2012) defined interstitial edematous pancreatitis, moderately (MSP) and acute severe pancreatitis (ASP), based on the presence or absence of necrosis [6, 7, 8]. The pathological findings in pancreas could be differ from edema up to necrosis depend on severity. For mild AP pharmaco- therapy is more appreciated. Surgical interventions are necessary for necrotic forms, with upcoming intensive care (ICU) management. ICU treatment requires high costs. There was calculated, that in UK one day costs in ICU for patients with complicated pancreatitis is 1.500£, in USA varied from 3000 USD to 4000 USD. The mortality rate is individual in different countries, changed mainly between 10% and 20%. The complications of AP, such as sepsis, lung, hepatic and kidney insufficiency, exacerbate the clinical future and increased the lethal outcomes up to 54% [9, 10, 11].
Ranson criteria, APACHE II, SOFA, Marshall and some other prognostic systems were suggested to the predict the severity of AP. Despite the published prognostic values of these systems, all of them have some disadvantages and limitations, require a lot of laboratory data and complex calculation. Using those systems takes a long time and mainly not satisfies physicians in emergency situations. There is a demand in simple tests for timely planning of treatment, especially on admission and early hospital days, in patients with different clinical performance. The early determining of severity, forecasting of complications and predicting the outcomes of the AP is very important for achieving better results. The aim of study was to determine the predictive value of inflammatory markers for the early diagnostic of severity of acute pancreatitis and for prediction of further course of pathological processes in pancreas [12, 13, 14, 15].
Materials and Methods
Material Description
The retrospective analyses of outcomes of three hundred two patients with acute pancreatitis treated in the Scientific Centre of Surgery between 2010-2018 years were led. Age, sex, BMI, admission and discharge dates, therapy, surgical procedures, laboratory tests, comorbid diseases, inflammatory markers such as white blood cells (WBC), neutrophil lymphocyte ratio (NLR), C-reactive protein concentration were analyzed. According to Atlanta classification all patients were divided in MSP group with 257 patients and ASP group with 49 patients. The etiology of pancreatitis was similar in both groups: biliary pancreatitis – 59.7%; alcohol pancreatitis - 38%; idiopathic and other causes defined in 2.3%. Among MSP patients (females 153; males 104) the average age was 49.1±0.96 years. In this group after examinations pancreas edema were detected; clinically constant pains in epigastria with light elevation of pancreatic enzyme activity. The average age in ASP group was 48.2±1.93 years (36 females and 23 males). In ASP group, the organ insufficiency developed in early 48 hours after admission; also, local complications such as necrosis, infiltration, fluid collection were identified. The duration from the first attack till hospital admission was 15.6±9.3 hour, and varied from 5 hour up to 2 days. Generally, age, female/male ratio, causes and other parameters were not significantly different among groups. All laboratory tests and instrumental examinations were led in the Scientific Centre of Surgery.
Statistics
All data were gathered in Excel sheet, and then transferred for statistical processing in IBM SPSS-20 program. Continuous variables were expressed as Mean ± median (M±m). Categorical variables are expressed as actual numbers and their percentages. The statistical analyze was performed with non-parametric Mann–Whitney U test and with the Student - t test. P values <0.05 were considered statistically significant. For the evaluation of different cut-off points ROC (Receiver Operating Characteristic) curve were used. The ROC curve is a plot of sensitivity versus 1-specificity for all possible cut off values. The index of accuracy is the area under the receiver operating characteristic curve (ROC- AUC), where values close to 1.0 indicate high diagnostic accuracy, and 0.5 indicates a test of no diagnostic value. P values <.05 were considered statistically significant. Kaplan– Meier curves were used to illustrate survival data and log- rank tests were used to test for statistically significant survival. Multivariable analysis was carried out with logistic regression and Cox proportional hazard models. Risk ratios were obtained from hazard models.
Results
Firstly, the WBC count compared among patients. On admission, slightly elevation of the WBC (12.7±1.2×109/l.) in the MSP group was determined. However, in ASP patients WBC count was significantly higher (15.4±2.3×109/l. (p<0.05)). The detailed analysis of the white cells, revealed the significantly difference in numbers of the neutrophil and lymphocytes. The neutrophils in MSP group were 9.3±4.1×109/l, however in ASP group increased significantly and was 13.4±5.6×109/l. Nevertheless, the lymphocytes in ASP group were lower compare to MSP patients (1.1±0.4×109/l vs. 0.96±0.9×109/l). Neutrophil/ lymphocytes ratio (NLR) was in all patients calculated (Table 1). NLR compared among groups at admission day, 1st and
2nd day after admission. On admission, the NLR was high in ASP group compare to MSP patients. Future calculations showed increasing of NLR in ASP group. Two days after admission this ratio was twice more than in MSP patients. Nevertheless, at patients with mild pancreatitis NLR had a tendency to fall up. At admission day and at early two days after hospitalization the NLR was significantly high in ASP group (p<0.05). ROC analyses revealed “cut off” for NLR and it was equal to 10.5. Kaplan – Meyer curve was formatted for 3 weeks survival depends on NLR “cut off”. In cases, when NLR < 10.5 the survival during 21 day after admission was 95.9%. In patients with acute severe pancreatitis by NLR > 10.5 the survival failed up to 79.2%. Moreover, the mortality raised up to 21.8%. Figure 1 Shows the Kaplan-Meyer curve depending of NLR cut off. In patients with acute severe pancreatitis the left shift in leucocytes formula was observed. As an early marker of systemic inflammation, the percentage immature granulocytes (IG) were studied. Compare the percentage of IG between groups allow us to evaluate the prognostic value of this marker. Our investigations showed that the number of IG increased in 47% patients with mild pancreatitis. However, in 72% patients from ASP group this marker was significantly high. The percentages of the immature granulocytes in MP group were 0.39±0.21% and ASP group 1.7±0.51%.With AUROC analyze the cut off for immature granulocytes were as 0.81% calculated.
| Mild pancreatitis | Acute severe pancreatitis | p | |
|---|---|---|---|
| Admission day | 9,78±1,3 | 12,6±1,4 | <0,05 |
| 1 day after | 8,41±1,1 | 14,2±1,7 | <0,05 |
| 2 days after | 7,74±0,9 | 15,3±1,2 | <0,05 |
Note: P values <.05 were considered statistically significant. Table 1: Neutrophil/Lymphocytes Ratio changes in groups.
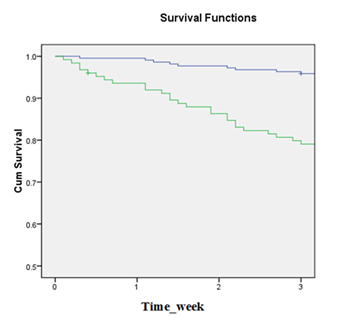
Blue line, survival of patients with NLR less than or equal to the corresponding cut off score: NLR < 10,5;
Green line, survival of patients with NLR more than or equal to cut off score: NLR > 10,5 Figure 1: The Kaplan-Meyer curve for patients depending on NLR cut off score.
Compare of CRP results evaluated an interesting fact. At admission day CRP concentration in both groups (MSP group 12.4±1.8 mg/dL vs. 13.2±2.4 mg/dL in ASP group) was not significantly differ. As shown in Figure 2 the concentration of CRP in future two days after admission cardinally changed. 1st day after admission the CRP concentration raised up at both groups, however at MSP patients this tendency was minimal and compare to the CRP value at admission the difference was not significant. But in ASP group the CRP increased about 55.3% from initial values at admission day (p < 0.05). At the 2nd day CRP concentration decreased at MSP group, however the raise the CRP values at ASP group continued. The impact of the comorbid diseases to outcomes was also investigated. Most of patients suffered from different diseases, in most cases simultaneously two or three comorbid diseases were observed. Distribution of comorbid diseases were: coronary heart disease at 40,8%; arterial hypertension at 29,6%; diabetes mellitus at 25,4%; gastritis and duodenitis at 25,4%; fatty liver disease at 59,2% patients were determined. Table 2 shows the multivariate analyze aiming to determine risk factors. As an independent risk factor, diabetes mellitus was associated with emerging of the septic complications. The negative impact of fatty liver disease to beginning and next exacerbation of multiorgan failure at patients with pancreatic tissue necrosis was also identified.
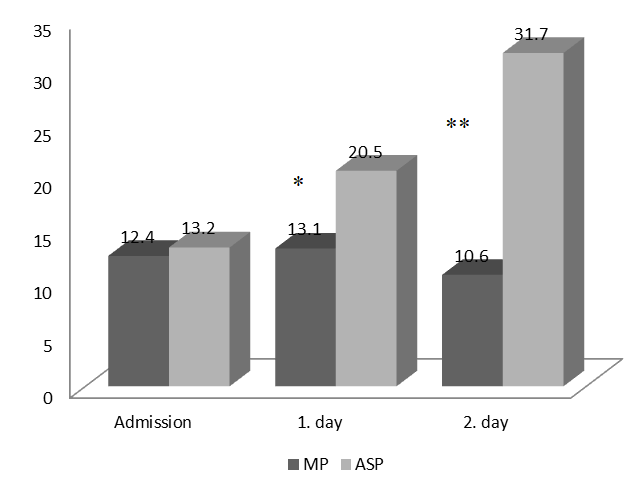
Note: MP – mild pancreatitis; ASP – acute severe pancreatitis. * - p<0,05;** - p < 0,01 Figure 2: C-reactive protein changes at patients with pancreatitis at admission day and next 2 day of hospitalization.
| OR | 95% CI | p | |
|---|---|---|---|
| Coronary heart disease | 1.014 | 0.991 – 1.038 | 0.23 |
| Arterial hypertension | 1.047 | 0.971 – 1.128 | 0.231 |
| Diabetes mellitus | 1.034 | 1.001 – 1.069 | 0.045* |
| Gastritis and duodenitis | 1.026 | 0.997 – 1.057 | 0.083 |
| Fatty liver disease | 3.006 | 1.369 – 6.600 | 0.006** |
Table 2: Multivariate analyse for identification of independent risk factor among comorbid diseases.
Notes: OR – Odd Ratio; CI – Confidence Interval. * p<0.05; p<0.01; Table 2:** Multivariate analyse for identification of independent risk factor among comorbid diseases.
Discussion
The examination and quantification of inflammatory markers at admission day and in early 2 days allowed us to detect important facts for future developing acute pancreatitis. The increased WBC at admission was essential for all patients, however at ASP group leucocytes count was significantly high compare to MSP group. Analyze of percentage ratio of the main parts of leucocytes formula showed, that NLR could use as a significant marker of pancreatitis complication in early days of hospitalization. The importance of increased immature granulocytes’ percentage as a predictor of the emerging of complications, such as fluid collection and gland tissue necrosis was confirmed. At admission day the CRP concentration was equal in all patients, not depending on complicated or mild forms of disease. So, at admission, CRP is not enough good for prediction of complication. NLR together with immature granulocytes count have more predictive value compare to CRP in early days after hospitalization. However, during the next 2 day after admission CRP achieved strong predictive value. At patients with mild pancreatitis, CRP had tendency to reduce, however rising of this marker directly indicate to emerging of complications. CRP values, as predictors on 2nd day after admission showed more significance.
Conclusion
We suggest that in patients with acute severe pancreatitis not only WBC, also the neutrophils and IG count should be used as laboratory test markers. At admission day the NLR shows more specific prognostic performance compare to CRP concentration. CRP value at the 2 day after admission has important significance. Diagnostic of comorbid diseases and evaluation of this severity is very important in patients with pancreatitis. Multivariate analyze defined, that comorbid diseases seriously influence to the future clinical course of acute pancreatitis. Diabetes mellitus and fatty liver disease significantly impact to the developing of life-threatening complications in patients with acute pancreatitis and led to untoward outcomes.
References
-
Xiao AY, Tan MLY, Wu LM, Asrani VM, Windsor JA, et al. (2016) Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta- regression of population-based cohort studies. Lancet Gastroenterol Hepatol 1(1): 45-55.
-
Machicado JD, Yadav D (2017) Epidemiology of recurrent acute and chronic pancreatitis: Similarities and differences. Dig Dis Sci 62(7): 1683-1691.
-
Whitcomb DC, Yadav D, Adam S, Hawes RH, Brand RE, et al. (2008) Multicenter approach to recurrent acute and chronic pancreatitis in the United States: the North American Pancreatitis Study 2 (NAPS2). Pancreatology 8(4-5): 520-531.
-
Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, et al. (2012) Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology 143(5): 1179-1187.
-
Krishna SG, Kamboj AK, Hart PA, Hinton A, Conwell DL (2017) The changing epidemiology of acute pancreatitis hospitalizations: a decade of trends and the impact of chronic pancreatitis. Pancreas 46(4): 482-488.
-
Shah AP, Mourad MM, Bramhall SR (2018) Acute pancreatitis: current perspectives on diagnosis and management. J Inflamm Res 11: 77-85.
-
Ignatavicius P, Gulla A, Cernauskis K, Barauskas G, Dambrauskas Z (2017) How severe is moderately severe acute pancreatitis? Clinical validation of revised 2012 Atlanta Classification. World J Gastroenterol 23(43): 7785-7790.
-
Chua TY, Walsh RM, Baker ME, Stevens T (2017) Necrotizing pancreatitis: Diagnose, treat, consult. Cleve Clin J Med 84(8): 639-648.
-
Greenberg JA, Hsu J, Bawazeer M, Marshall J, Friedrich JO, et al. (2016) Clinical practice guideline: management of acute pancreatitis. Can J Surg 59(2): 128-140.
-
Janisch NH, Gardner TB (2016) Advances in Management of Acute Pancreatitis. Gastroenterol Clin North Am 45(1):1-8.
-
Neoptolemos JP, Raraty M, Finch M, Sutton R (1998) Acute pancreatitis: the substantial human and financial costs. Gut 42(6): 886-891.
-
Nicolás LAL, Hernández JLP, Pérez EGD, Zúñiga AES (2010) Correlation among clinical, biochemical and tomographic criteria in order to evaluate the severity in acute pancreatitis. Rev Esp Enferm Dig 102(6): 376-380.
-
Ferreira ADF, Bartelega JA, Urbano HCDA, Souza IKFD (2015) Acute pancreatitis gravity predictive factors: which and when to use them? Arq Bras Cir Dig 28(3): 207-211.
-
Chatzicostas C, Roussomoustakaki M, Vlachonikolis IG, Notas G, Mouzas I, et al. (2002) Comparison of Ranson, APACHE II and APACHE III scoring systems in acute pancreatitis. Pancreas 25(4): 331-335.
-
Phillip V, Steiner JM, Algül H (2014) Early phase of acute pancreatitis: Assessment and management. World J Gastrointest Pathophysiol 5(3): 158-168.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient