Practices in Paediatric Gastrointestinal Endoscopy at Kenyatta National Hospital and Gertrude’s Children’s Hospital in Nairobi, Kenya
Background: Gastrointestinal (GI) diseases are common in children worldwide and pediatric GI endoscopy has become a fundamental component of healthcare for infants and children. There is a wide range of diagnostic and therapeutic indications for pediatric upper and lower GI endoscopy as well as new diagnostic and therapeutic interventions for the endoscopic findings Objectives: To document the indications, endoscopic findings and therapeutic procedures in pediatric upper and lower gastrointestinal endoscopy at the Kenyatta National Hospital (KNH) and Gertrude’s children’s hospital. Design: Cross-sectional, consecutive entry study Setting: Kenyatta National Hospital and Gertrude’s children’s hospital Materials and Methods: This study was done over a period of 5 months involving participants of age 13 years and below who underwent GI endoscopy at the endoscopy units of KNH and Gertrude’s children’s hospital. The subjects who met the eligibility criteria were recruited by the Principal Investigator through consecutive sampling. Data was recorded in a data abstraction form. Permission to undertake the study was obtained from the combined institutional Research and Ethics Committee (IREC) of KNH and University of Nairobi as well as the Ethics Review Board of Gertrude’s Children Hospital.Data was anonymized prior to analysis. Written informed consent for the study was obtained from the participants’ parents or guardians. The data collected was coded and entered in MsAccess data base. Data cleaning was done and the data exported into SPSS version 23.0statistical software. All statistical tests were performed at 5% level of significance. Results: Mean age of the children was 7.3 years (std=3.9). Males were 58 (52.7%). OGD involved 79.1% of the participants. In KNH, the main indications for OGD (oesophagogastroduodenoscopy) were upper GI bleed and dysphagia while in Gertrude’s hospital, they were abdominal pain and emesis. Hematochezia was the predominant indication for colonoscopy. More study participants had normal than abnormal gross and histological findings. The commonest gastroscopic findings were gastritis and esophagitis. Hiatus hernia was detected in only 4.8% of the children. The commonest colonoscopic finding was colonic polyps. 69(62.7%) patients had results of biopsies taken being present. The commonest positive findings in the colon and rectum were chronic ulcerative colitis and juvenile polyps, respectively. The main therapeutic procedures done were banding for oesophageal varices, FB removal and oesophageal dilatation. Conclusions: The higher percentages of normal gross and histologic findings indicate more a functional than organic etiology to the GI presentations. Hiatus hernia is relatively uncommon in our population. Juvenile polyps are more common than ulcerative colitis as a cause of hematochezia in children. Recommendations: Considerations for higher possibility of functional diagnoses should be made for patients with recurrent abdominal pains and recurrent emesis. Emphasis should be made for parents/guardians of children who require biopsy that histology forms a crucial part of management.
Introduction
Gastrointestinal (GI) diseases are common in children worldwide and GI endoscopy in the pediatric population has evolved during the past few decades with an increasing number of diagnostic and therapeutic applications. Technological improvements in endoscope design and endoscopic devices have contributed immensely to the evolution of pediatric endoscopy and improvement in the skills that reflect on training. There has also been improved sedation and general anesthesia (GA) of children by trained anesthetists [1]. There is a gap in pediatric gastroenterology in Sub-Saharan Africa and the evolution of this field is expected to bridge it for the management of gastroenterological disorders in this region. Unlike adult gastroenterology, pediatric gastroenterology practice in Africa is younger and much less advanced in the scope and skill of services offered. Pediatric OGD and Colonoscopy have led to an increased recognition of GI disorders that are unique to children. The increase of disease rates from these pediatric GI procedures is more a reflection of increasing rates of disease diagnosis than a true rise of disease occurrence. According to the European Society of Gastrointestinal Endoscopy/ European Society for Pediatric Gastroenterology Hepatology and Nutrition (ESGE/ESPGHAN), the diagnostic indications for EGD are weight loss, failure to thrive, unexplained anemia, abdominal pain with suspicion of an organic disease, dysphagia or odynophagia, caustic ingestion, recurrent vomiting with unknown cause, hematemesis, hematochezia, unexplained chronic diarrhea, chronic gastroesophageal reflux disease (GERD), to exclude other diseases, or surveillance of Barrett’s esophagus [2]. The diagnostic indications of ileocolonoscopy in pediatric patients according to ESGE and ESPGHAN are unexplained anemia, unexplained chronic diarrhea, perianal lesions (fistula, abscess), rectal blood loss, unexplained failure to thrive, radiological suspicion of ileocolonic stenosis/stricture and polyposis syndromes. The therapeutic indications for ileocolonoscopy are polypectomy, dilation of ileocolonic stenosis, treatment of hemorrhagic lesions, foreign body removal and reduction of sigmoid volvulus. This study was undertaken to document the indications for these procedures in the two tertiary care hospitals.
Materials and Methods
This cross-sectional study was done over a period of 5 months involving participants of age 13 years and below who underwent GI endoscopy at the endoscopy units of KNH and Gertrude’s children’s hospital. 176 (100 males and 76 females) patients were screened for the study. 110 (58 males and 52 females) patients who met the eligibility criteria were recruited by the Principal Investigator through consecutive sampling and included in the study. Written informed consent for the study was obtained from the participants’ parents or guardians. A standard questionnaire was run for each study subject and included biodata and relevant details.
Ethical Approval
Permission to undertake the study was obtained from the combined institutional Research and Ethics Committee (IREC) of KNH and University of Nairobi as well as the Ethics Review Board of Gertrude’s Children Hospital.
Statistical Analysis
Data was recorded in a data abstraction form. Data was anonymized prior to analysis. The data collected was coded and entered in Ms Access data base. Data cleaning was done and the data exported into SPSS version 23.0statistical software. All statistical tests were performed at 5% level of significance.
Hospital Total (N=110) p-value Getrude (N=55) KNH (N=55) Age (years) 0.4771
Mean ± SD
$$ \begin{array}{l} \mathrm {M e a n} \pm \mathrm {S D} 7. 6 \pm 3. 9 7. 0 \pm 3. 9 7. 3 \pm 3. 9 \\ (\mathrm {R a n g e}) (1. 0 - 1 3. 0) 0. 6 6 7 - 1 3. 0 0 0 (0. 6 6 7 - 1 3. 0 0) \\ \end{array} $$
(1.0 - 13.0)
0.667 - 13.000
(0.667 - 13.000)
Sex 0.4452 Male 31 (56.4%) 27 (49.1%) 58(52.7%) Female 24 (43.6%) 28 (50.9%) 52 (47.3%)
Results
| Variable | Hospital | Total (N=110) | p value | |
|---|---|---|---|---|
| Getrude (N=55) Freq (Col %) | KNH (N=55) Freq (Col %) | Freq (Col%) | ||
| Indication | <0.0013 | |||
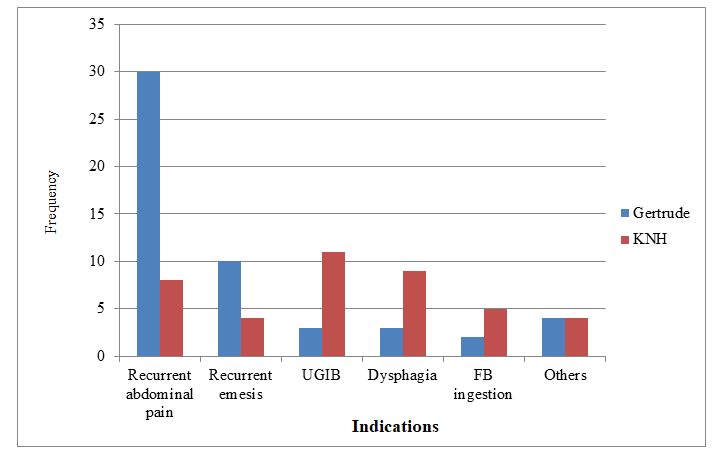
| Recurrent abdominal pain | 30 (54.5%) | 8 (14.5%) | 38 (34.5%) | |
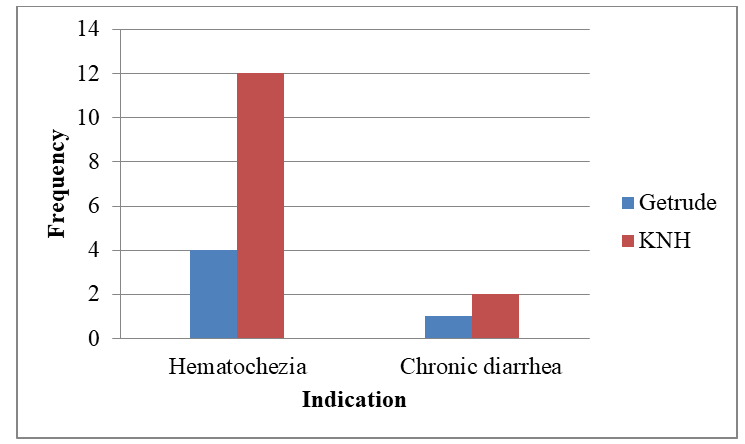
| Hematochezia | 4 (7.3%) | 12 (21.8%) | 16 (14.5%) | |
| Recurrent emesis | 10 (18.2%) | 4 (7.3%) | 14 (12.7%) | |
| UGIB | 3 (5.5%) | 11 (20.0%) | 14 (12.7%) | |
| Dysphagia | 2 (3.6%) | 9 (16.4%) | 11 (10.0%) | |
| FB ingestion | 4 (7.3%) | 5 (9.1%) | 9(8.2%) | |
| Others | 1 (1.8%) | 4 (7.3%) | 5 (4.5%) | |
| Chronic diarrhea | 1 (1.8%) | 2 (3.6%) | 3 (2.7%) | |
| Procedures done | 0.0493 | |||
| OGD | 47 (85.5%) | 40 (72.7%) | 87 (79.1%) | |
| Colonoscopy | 5 (9.1%) | 14 (25.5%) | 19 (17.3%) | |
| OGD and colonoscopy | 3 (5.5%) | 1 (1.8%) | 4 (3.6%) | |
| Material ingested | 0.0233 | |||
| N | 4 | 12 | 16 | |
| Button battery | 0 (0.0%) | 7 (58.3%) | 7 (43.8%) | |
| Caustic ingestion | 2 (50.0%) | 5 (41.7%) | 7 (43.8%) | |
| Coins | 2 (50.0%) | 0 (0.0%) | 2 (12.5%) |
Table 1: Indications and Procedure by hospital. 3Fishers’ exact test All the participants who had ingested a material in the two
| Variable | Hospital | Total (N=110) | p value | |
|---|---|---|---|---|
| Gertrude (N=55) Freq (Col %) | KNH (N=55) Freq (Col %) | |||
| Gross findings in pharynx | 1.0003 | |||
| N | 3 | 3 | 6 | |
| Erythema | 3 (100.0%) | 2 (66.7%) | 5 (83.3%) | |
| Mouth Ulcers | 0 (0.0%) | 1 (33.3%) | 1 (16.7%) | |
| Gross findings in oesophagus | < 0.0013 | |||
| N | 50 | 41 | 91 | |
| Normal | 26 (52.0%) | 14 (34.1%) | 40 (44.0%) | |
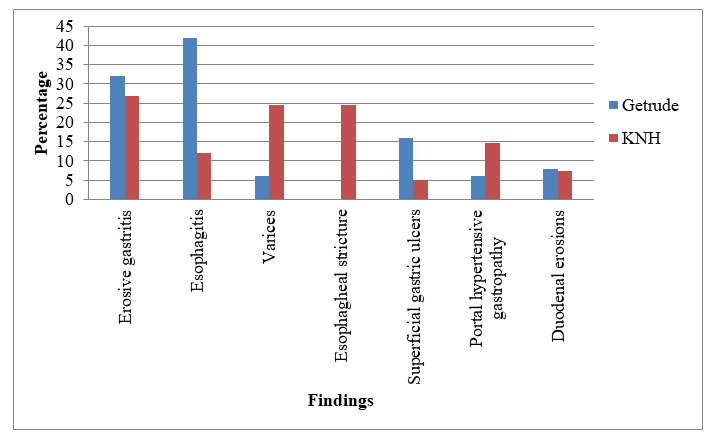
| Esophagitis | 21 (42.0%) | 5 (12.2%) | 26 (28.6%) | |
| Varices | 3 (6.0%) | 10 (24.4%) | 13 (14.3%) | |
| Stricture | 0 (0.0%) | 10 (24.4%) | 10 (11.0%) | |
| Others | 0 (0.0%) | 2 (4.9%) | 2 (2.2%) | |
| Hiatus Hernia | 1.0003 | |||
| N | 50 | 41 | 91 | |
| No | 49 (0.0%) | 40 (97.6%) | 89 (95.2%) | |
| Yes | 1 (100.0%) | 1 (2.4%) | 2 (4.8%) | |
| Gross findings in stomach | 0.1493 | |||
| N | 50 | 41 | 91 | |
| Normal | 22 (44.0%) | 19 (46.3%) | 41 (45.1%) | |
| Erosive gastritis | 16 (32.0%) | 11 (26.8%) | 27 (29.7%) | |
| Superficial ulcers | 8 (16.0%) | 2 (4.9%) | 10 (11.0%) | |
| Portal hypertensive | 3 (6.0%) | 6 (14.6%) | 9 (9.9%) | |
| Varices | 0 (0.0%) | 2 (4.9%) | 2 (2.2%) | |
| Cobblestone appearance | 1 (2.0%) | 0 (0.0%) | 1 (1.1%) | |
| Fundal tumour | 0 (0.0%) | 1 (2.4%) | 1 (1.1%) | |
| Gross findings in duodenum | 0.1633 | |||
| N | 50 | 41 | 91 | |
| Normal | 43 (86.0%) | 34 (82.9%) | 77 (84.6%) | |
| Erosions | 4 (8.0%) | 3 (7.3%) | 7 (7.7%) | |
| Hyperemia | 3 (6.0%) | 0 (0.0%) | 3 (3.3%) | |
| Ulceration | 0 (0.0%) | 2 (4.9%) | 2 (2.2%) | |
| Bile reflux | 0 (0.0%) | 1 (2.4%) | 1 (1.1%) | |
| Polyps | 0 (0.0%) | 1 (2.4%) | 1 (1.1%) | |
| 0.0373 | ||||
| N | 8 | 15 | 23 | |
| Normal | 8 (100.0%) | 6 (40.0%) | 14 (60.8%) | |
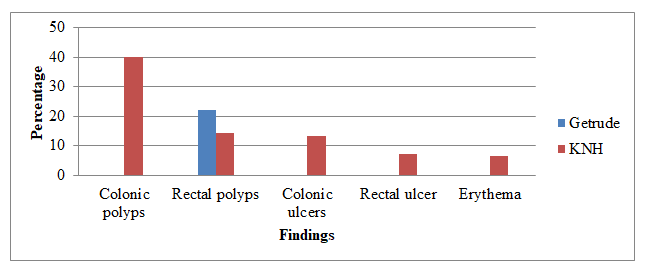
| Polyps | 0 (0.0%) | 6 (40.0%) | 6 (26.1%) | |
| Mucosal ulceration | 0 (0.0%) | 2 (13.3%) | 2 (8.7%) | |
| Erythema | 0 (0.0%) | 1 (6.7%) | 1 (4.3%) | |
| Gross findings in rectum | 0.7573 | |||
| N | 9 | 14 | 23 | |
| Normal | 7 (77.8%) | 11 (78.6%) | 18 (78.3%) | |
| Polyp | 2 (22.2%) | 2 (14.3%) | 4 (17.4%) | |
| Ulcers | 0 (0.0%) | 1 (7.1%) | 1 (4.3%) | |
| Biopsy results | < 0.0012 | |||
| N | 55 | 55 | 110 | |
| Absent | 8 (14.5%) | 33 (60.0%) | 41 (37.3%) | |
| Present | 47 (85.5%) | 22 (40.0%) | 69 (62.7%) | |
| Variable | Hospital | Total | P-value | |
| Getrude (N=55) | KNH (N=55) | |||
| Freq (Col %) | Freq (Col %) | |||
| Histological findings in esophagus | < 0.0013 | |||
| N | 42 | 4 | 46 | |
| Normal | 38 (90.5%) | 0 (0.0%) | 38 (82.6%) | |
| Esophagitis | 3 (7.1%) | 3 (75.0%) | 6 (13.0%) | |
| Eosinophilic esophagitis | 1 (2.4%) | 0 (0.0%) | 1 (2.2%) | |
| Squamous cell carcinoma | 0 (0.0%) | 1 (25.0%) | 1 (2.2%) | |
| Histological findings in stomach | < 0.0013 | |||
| N | 42 | 14 | 55 | |
| Normal | 25 (61.0%) | 0 (0.0%) | 25 (45.5%) | |
| Superficial gastritis | 15 (36.6%) | 13 (92.9%) | 28 (50.9%) | |
| Atrophic gastritis | 0 (0.0%) | 1 (7.1%) | 1 (1.8%) | |
| Erosions | 1 (2.4%) | 0 (0.0%) | 1 (1.8%) | |
| Histological findings in duodenum | 0.0123 | |||
| N | 40 | 2 | 42 | |
| Normal | 37 (92.5%) | 0 (0.0%) | 37 (88.1%) | |
| Duodenitis | 1 (2.5%) | 2 (100.0%) | 3 (7.1%) | |
| Atrophic enteropathy | 1 (2.5%) | 0 (0.0%) | 1 (2.4%) | |
| Lymphoid hyperplasia | 1 (2.5%) | 0 (0.0%) | 1 (2.4%) | |
| Histological findings in colon | 0.0213 | |||
| N | 5 | 8 | 13 | |
| Normal | 4 (80.0%) | 0 (0.0%) | 4 (30.8%) | |
| Chronic ulcerative colitis | 1 (20.0%) | 3 (37.5%) | 4 (30.8%) | |
| Juvenile polyp | 0 (0.0%) | 3 (37.5%) | 3 (23.1%) | |
| Lymphonodular hyperplasia | 0 (0.0%) | 2 (25.0%) | 2 (15.4%) | |
| Histological findings in rectum | 0.4293 | |||
| N | 6 | 2 | 8 | |
| Normal | 4 (66.7%) | 0 (0.0%) | 4 (50.0%) | |
| Juvenile Polyp | 2 (33.3%) | 2 (100.0%) | 4 (50.0%) | |
| H. pylori status | 0.4363 | |||
| N | 47 | 22 | 69 | |
| Positive | 8 (17.1%) | 6 (27.3%) | 14 (20.3%) | |
| Negative | 39 (82.9%) | 16 (72.7%) | 55 (79.7%) |
Table 2: Gross findings by hospital.
| Gertrude | KNH | Total | |
|---|---|---|---|
| N | 50 | 41 | 91 |
| Banding | 2 (4%) | 9 (22%) | 11 (12.1%) |
| Dilatation | 0 (0%) | 8 (19.5%) | 8 (8.8%) |
| PEG tube insertion | 1 (2%) | 3 (7.3%) | 4 (4.4%) |
| FB removal | 2(4%) | 7 (17.1%) | 9 (9.9%) |
| No procedure | 45 (90%) | 14 (33.3%) | 59 (64.8%) |
Table 3: Therapeutic procedures in OGD.
| Gertrude | KNH | Total | ||
|---|---|---|---|---|
| N | 8 | 15 | 23 | |
| Polypectomy | 1 (13.5%) | 6 (40%) | 7 (30.4%) | |
| No procedure | 7 (87.5%) | 9 (60%) | 16 (69.6) | |
| Variable | Hospital | Total (N=110) | p value | |
| Variable | Getrude (N=55) Freq (Col%) | Total (N=110) | p value | KNH (N=55) Freq (Col%) |
| Therapeutic procedure | 0.2733 | |||
| N | 6 | 33 | 39 | |
| Banding varices | 2 (33.3%) | 9 (27.3%) | 11 (28.2%) | |
| Polypectomy | 1 (16.7%) | 6 (18.2%) | 7 (18.0%) | |
| Dilatation | 0 (0.0%) | 8 (24.2%) | 8 (20.5%) | |
| PEG tube insertion | 1 (16.7%) | 3 (9.1%) | 4 (10.3%) | |
| FB removal | 2 (33.3%) | 7 (21.2%) | 9 (23.1%) |
Table 4: Therapeutic procedures in Colonoscopy.
Discussion
Sociodemographic Characteristics
There was no statistically significant difference between the mean ages of the children seen in the two facilities (p=0.477). There was also no significant difference between the two genders of the children in both facilities (p=0.445). The total number of males was 58 (52.7%) while the remaining 52(47.3%) were females. This is comparable to a 5 year retrospective study in Ethiopia where 55.3% of the study participants were male children [3]. There was no significant difference in gender distribution between the two facilities.
In both KNH and Gertrude’s children hospital, OGD were performed more than Colonoscopy (79.1% versus 17.3 %). This is in keeping with findings in other centers which offer GI endoscopy [4, 5, 6, 7].
Indications
In KNH, the indications for OGD in decreasing order of occurrence were upper GI bleed (20.2 %), dysphagia (16.4%), recurrent abdominal pain (14.5%), foreign body ingestion (9.1 %), recurrent emesis (7.3%) and others (convulsive disorder, hypoxic brain Injury, small for age and failure to thrive) (7.3 %). In Gertrude’s hospital, the indications for OGD were recurrent abdominal pain (54.5%), recurrent emesis (18.2%), FB ingestion (7.3%), upper GI bleed (5,5%), dysphagia (3.6%) and others. The pattern of the indications differed significantly in the two facilities with a p-value of <0.001. This is similar to findings from studies done in Nigeria where epigastric pain (37.3%), haematemesis (28.8%) and dysphagia (15.3%) were the predominant indications for OGD [6]. A total of 16 (14.5 %) patients had ingested a material with more presenting at KNH compared to Gertrude. The main materials they had ingested were button battery and caustic substances with each hospital having
7 (43.8%) children presenting with each. This is different from what is observed in other studies with a Taiwan study showing that most of the foreign bodies ingestion was coins (56.8%), button batteries (21.6%), sharp objects (12.2%) then chicken bones (n = 2, 2.7%) [8]. In another study in India, coins were the most frequent offending agents in children (87.5%) [9]. The number of children by diagnoses of material ingestion seen at endoscopy (button battery, caustic ingestion and coins) stood at 16 as compared to the 9 children who came with FB ingestion as an indication for OGD. This observation demonstrates that in this study, the number of children with a FB in their upper digestive tract was more than the number who presented with FB ingestion as an indication for OGD.
In KNH, hematochezia and chronic diarrhoea were the indications for colonoscopy at 12(85.7%) and 2(14.3%) of the study participants, respectively. In Gertrude’s hospital, colonoscopy was done for hematochezia and chronic diahhoea at 4(80%) and 2 (20%) of the study participants, respectively. These findings are comparable to findings of a similar study in Sudan where the predominant indications for colonoscopy were rectal bleeding (87%), diarrhoea (19%) and anaemia (10%) [7]. In our study, only 1 out of 14 children (7.1%) and 3 out of 8 children (37.5%) had colonoscopy for recurrent abdominal pain in KNH and Gertrude’s children hospital, respectively. Colonoscopy is likely not warranted in children with recurrent abdominal pain without bleeding, weight loss, or altered bowel habit.
Endoscopic Findings
Oesophagogastroduodenoscopy
The commonest gastroscopic findings in our study were Gastritis which were findings in 27 (29.7%) of the patients followed by Esophagitis seen in 26 (28.6%) of them and varices in 13 (14.3%), This observation concurs with that of the Pakistan study [10], where gastritis is the commonest finding accounting for 14.5% of the observations. There were 6 participants with a gross finding in the pharynx. This represents 5.5% of all children in both hospitals. Of these, majority were Erythema 5(83.3%) and there was no statistically significant difference in the two hospitals. 3 (50%) of children who had caustic ingestion had erythema or mouth ulcers and this finding contrasts with a finding of a study in Poland where 23.3% of children who ingested caustic substances had lesions in the pharynx from the ingestion [11]. The pattern of the differences in gross findings in oesophagus in the two hospitals was statistically significant with a p-value of <0.001. Regarding findings in the oesophagus, there were more with normal findings in Gertrude 26 (52%) compared to KNH 14 (34.1%). This could be probably because of more children with disease needing therapeutic procedures being brought to KNH where the endoscopy services are cheaper compared to the more expensive services at the Gertrude’s children hospital where endoscopy is done in a surgical theatre set up. The main finding in the oesophagus was oesophagitis. The findings under ‘Others’ included oesophageal candidiasis seen in a 7 years old child and congenital stenosis which was noted in an 8 months child in KNH each representing 0.9% of the study participants. This finding is similar to a finding in a study in Romania where paediatric infectious oesophagitis was seen in only 2.11% of patients and was attributed to Candidiasis, cytomegalovirus infection and Herpes simplex virus infection [12].
Congenital esophageal stenosis is a rare cause of childhood dysphagia encountered in OGD as confirmed by a case report in India [13]. In both facilities, a higher proportion had normal findings 41(45.1%) in the stomach and of those with abnormal finding the main finding was erosive gastritis, 27(29.7%) while in the duodenum the main finding was erosions 7 (7.7%). Hiatus hernia was seen in only 4.8% of the children in this study and this is comparable to a study done in Nepal where the prevalence of hiatus hernia was found to be 3% amongst children up to 15 years who underwent OGD [14].
Colonoscopy
There were 8 participants with colonoscopy findings in Gertrude hospital and all of them had a normal finding in the colon while in KNH there were 15 participants with colonoscopy findings and of these 6(40%) had polyps. Regarding the commonest colonoscopic findings in this study, 6 (26.1%) had colonic polyps followed by 4 (18.2%) with rectal polyps then 2 (8.7%) with colonic ulcers and another 2 (8.7%) with both rectal ulcers erythema. These findings resemble those in a study done in China where polyps (42.9%) and IBD (16.5%) were the two most common positive findings [15].
Histology Findings
A total of 69(62.7%) of the patients had results of biopsies taken with Gertrude having a higher proportion 47 (85.5%) in compared to 22(40.0%) in KNH. This was a statistically significant finding. In terms of procedure, majority of the existing biopsy results were among those who underwent OGD 52 (76.5%). Possible reasons for the higher proportion of absent histology results amongst patients in KNH include firstly, biopsy not being taken in cases where urgent OGD was done like in emergency foreign body removal and banding of bleeding oesophageal varices in unstable patients and secondly, loss of the biopsy specimen or histology results. A similar scenario was seen in a study of pediatric GI endoscopy in Brazil where biopsies were done in 120 (60.3%) of the children [16]. In this study, normal histology was observed from the biopsies taken in the esophagus and duodenum at 82.6% and 88.1% respectively and this is similar to findings in a study in Greece where 68% of the histology from biopsies in the OGD done in children were reported as normal and the study participants were considered to have functional dyspepsia [17]. Our study also showed that the commonest histological finding in the stomach of the children who underwent OGD was superficial gastritis as seen in 28 (50.9%) of the children, a finding that was also reflected in a study in Pakistan where the commonest histological finding was gastritis (antral biopsies) [18]. Regarding histological findings on colonoscopy in this study, the commonest findings were chronic ulcerative colitis, juvenile polyps and lympho- nodular hyperplasia seen in 30.8%, 23.1% and 15.4% of the study participants respectively. This is comparable to findings in a study in Ethiopia where the commonest histological findings on colonoscopy were hyperplastic polyps and juvenile polyps in 32% and 27% respectively [3]. In KNH, out of the 15 children who had Colonoscopy, 12 (80%) had gross lesions on endoscopic findings and 10 (66.7%) had positive histology findings. In Gertrude’s hospital, out of the 8 children who had Colonoscopy 2(25%) had gross lesions at endoscopy and 3 (37.5%) had positive histology findings.
Helicobacter Pylori Status
In this study, 14 (20.3%) of the study participants whose biopsy results were accessible were positive for H.pylori infection which differs from a study in Brazil where biopsies of the esophagus, stomach and duodenum were performed in 60% of the patients and in 13.1% of the patients, the H. pylori test was positive [16].
Therapeutic Procedures
In our study, oesophageal dilatation, PEG tube insertion and FB removal were done in 8.8%, 4.4% and 9.9% respectively in the patients who underwent OGD. This is comparable to a retrospective audit of paediatric OGD in Brazil where esophageal dilatation, PEG tube insertion and FB removal were done in 0.5%, 2% and 6% of the study participants, respectively [16]. In Gertrude’s children’s hospital, both cases of FB removal involved coins lodged in the oesophagus and in KNH, all of the 7 children with button batteries ingested had removal of these objects. This finding in KNH is similar to a finding in Chile where 22(88%) of the children with ingestion of button batteries had these foreign bodies removed [19]. Most of the therapeutic procedures for the children were done in KNH as compared to Gertrude’s children hospital probably because of less expense needed for treatment at KNH. In contrast to our study where overall 12.1% of the children who had OGD in the two hospitals needed banding for oesophageal varices, 3.4% of the study participants needed banding in a study in Nigeria [6]. In this study, 30.4% of the children who had colonoscopy had polypectomy which is similar to a study in Taiwan where 20.4% of children who underwent colonoscopy had polypectomy [20].
Conclusions
- The higher percentages of normal gross and histologic findings indicate more a functional than organic etiology to the gastrointestinal presentations in children who undergo endoscopy in our population.
- Hiatus hernia in children is uncommon in our set up.
- Juvenile polyps are more common than ulcerative colitis as a cause of hematochezia in children.
- The higher rates of esophageal dilatations and banding for varices in KHN as compared to Gertrude’s children hospital reflect the higher overall costs of treatment needed for repeat procedures.
Recommendations
- Considerations for higher possibility of functional diagnoses should be made for patients with recurrent abdominal pains and recurrent emesis.
- Emphasis should be made for parents/guardians of children who require biopsy that histology forms a crucial part of management.
- Because of the wider variety of therapeutic procedures in KNH compared to Gertrude’s children hospital, gastroenterology training would benefit more from public than from private hospitals.
References
-
Franciosi JP, Fiorino K, Ruchelli E, Shults J, Spergel J, et al. (2010) Changing indications for upper endoscopy in children during a 20-year period. J Pediatr Gastroenterol Nutr 51(4): 443-447.
-
Tringali A, Thomson M, Dumonceau JM, Tavares M, Tabbers MM, et al. (2017) Pediatric gastrointestinal endoscopy: European Society of Gastrointestinal Endoscopy (ESGE) and European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) Guideline Executive summary. Endoscopy 49(1): 83-91.
-
Tamire AH (2020) Clinical Profile and Outcome of Pediatric Patients undergoing gastroscopic and Colonoscopic procedures at Tikur Anbessa Specialized Hospital: A five-year endoscopy trend analysis. Ethiop Med J 58(1): 29-32.
-
Hayat JO, Sirohi R, Gorard DA (2008) Paediatric endoscopy performed by adult-service gastroenterologists. Eur J Gastroenterol Hepatol 20(7): 648-652.
-
Friedt M, Welsch S (2013) An update on pediatric endoscopy. Eur J Med Res 18(1): 24.
-
Alatise OI, Anyabolu HC, Sowande O, Akinola D (2015) Paediatric endoscopy by adult gastroenterologists in Ile-Ife, Nigeria: A viable option to increase the access to paediatric endoscopy in low resource countries. Afr J Paediatr Surg 12(4): 261-265.
-
Mudawi HMY, Tahir MAE, Suleiman SH, Eltaybe NH, Gamer NM, et al. (2009) Paediatric gastrointestinal endoscopy: Experience in a Sudanese university hospital. East Mediterr Health J 15(4): 1027-1031.
-
Lin CH, Chen AC, Tsai JD, Wei SH, Hsueh KC, et al. (2007) Endoscopic removal of foreign bodies in children. Kaohsiung J Med Sci 23(9): 447-452.
-
Shivakumar AM, Naik AS, Prashanth KB, Yogesh BS, Hongal GF (2004) Foreign body in upper digestive tract. Indian J Pediatr 71(8): 689-693.
-
Khan MR, Ahmed S, Ali SR, Maheshwari PK, Jamal MS (2014) Spectrum of upper GI endoscopy in Pediatric Population at a Tertiary Care Centre in Pakistan. Open Journal of Pediatrics 4(3): 180-184.
-
Niedzielski A, Schwartz SG, Pietrzyk KP, Niedzielska GM (2020) Caustic Agents Ingestion in Children: A 51-Year Retrospective Cohort Study. Ear Nose Throat J 99(1): 52- 57.
-
Bordea MA, Pîrvan A, Gheban D, Silaghi C, Lupan I, et al. (2020) Infectious Esophagitis in Romanian Children: From Etiology and Risk Factors to Clinical Characteristics and Endoscopic Features. J Clin Med 9(4): 939.
-
Rastogi R, Majid A, Singh VP, Joon P, Gupta Y (2016) Congenital Esophageal Stenosis: A Rare Case of Childhood Dysphasia. J Gastrointest Dig Syst 6(2): 407.
-
Joshi MR, Sharma SK, Baral MR (2005) Upper GI endoscopy in children in an adult suite. Kathmandu Univ Med J (KUMJ) 3(2): 111-114.
-
Lei P, Gu F, Hong L, Sun Y, Li M, et al. (2014) Pediatric Colonoscopy in South China: A 12-Year Experience in a Tertiary Center. PLoS One 9(4): e95933.
-
Coca DS, Santos CM, Oliveira OSGD, Pereira DA, Furuya CJK, et al**.** (2018) Upper gastrointestinal endoscopy applied in pediatrics: Endoscopic and histological findings, including Helicobacter pylori. Rev Gastroenterol Peru 38(1): 40-43.
-
Spiroglou K, Paroutoglou G, Nikolaides N, Xinias I, Giouleme O, et al. (2004) Dyspepsia in childhood: Clinical manifestations and management. Annals of Gastroenterology 17(2): 173-180.
-
Khurram M, Khaar HTB, Hasan Z, Umar M, Javed S, et al. (2003) A 12 years audit of upper gastrointestinal endoscopic procedures. J Coll Physicians Surg Pak 13(6): 321-324.
-
Ríos G, Rodríguez L, Lucero Y, Miquel I, Arancibia ME, et al. (2020) Endoscopic Findings Associated With Button Battery Ingestion in Children: Do We Need to Change the Protocol for Managing Gastric Location? Pediatr Emerg Care 36(11): 523-526.
-
Wu CT, Chen CA, Yang YJ (2015) Characteristics and Diagnostic Yield of Pediatric Colonoscopy in Taiwan. Pediatr Neonatol 56(5): 334-338.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient