Incidental Finding of Late Metastasizing Melanoma to the Duodenum by PET-CT: About a Case Report
Three years later after primary resection from skin melanoma with right inguinal lymphadenectomy, a Caucasian 62-year old female patient underwent at Helios Hospital Pforzheim investigations because of persistent high grade fever episodes. A very high suspicious mass of tumor was incidental identified and described in the descending duodenum and head of pancreas after PET-CT scan. Upper endoscopic examination with ultrasonography showed a 30 mm tumor mass arising from the descending part of the duodenum, which had invaded the head of pancreas and caused loop obstruction. Endoscopic biopsy revealed neoplastic cells with melanin granules and positive for Melan-A/SOX10 staining, indicating the presence of a metastatic malignant melanoma. It showed no BRAF-Mutation. These additional staining’s were evaluated after surgery. The colonoscopy showed not tumor finding. After tumor board procedure we strongly recommended surgical resection, and the patient accepted surgery. She underwent in Department of General Surgery at Helios Hospital Pforzheim the pylorus preserving pancreatico-duodenectomy. In the surgically resected Whipple specimen, the mass was 5x4 cm large, solid and ulcerated. Histologically the tumor infiltrated all duodenal layers and the tissue around them. Immunocytochemistry and electronic microscopy findings confirmed the diagnosis of malignant melanoma; similar to the skin specimen from the right thigh; therefore, the duodenal lesion was considered to be a metastasizing skin melanoma from the right thigh. The post operatory evolution was good, and was released from the hospital after 13 days. She underwent immunotherapy with Ipilimumab and Nivoluma. No recur was registrated during 5 months close follow-up. The history of the patient began three years earlier. She underwent a resection of skin melanoma. The initial skin melanoma was localized on anterior side of the right thigh (lower limb). At that time pathological specimen confirmed as malignant melanoma Clark level IV, pT2aN1bM0 as TNM-Staging, positive for BRAF-Wild-type by Mutation Analysis. Our patient also underwent another removal of skin melanoma from the back area just a couple of months after the first surgery. Pathological results from the second specimen confirmed as skin melanoma Clark level II, pT1a as TNM-Staging. She received chemotherapy and heavy particle radiotherapy after surgery. No suspect mass was identified on regular follow-up during 12 months after primary operation. Recurrence was registrated in the scar on the right thigh (lower limb) and right inguinal site, two years later. No suspect mass was identified on follow-up CT-Scan’s from head, lung and abdomen. She received immunotherapy and no additional chemotherapy or radiotherapy.
Introduction
Melanomas are uncommon malignancy that arise from melanocytes and often metastasize to several organs. Metastatic melanoma to gastrointestinal tract is unexpected identity which manifested asymptomatic course or nonspecific symptoms, that commonly remains undiagnosed in living patients. However, duodenal metastasis from skin melanoma with pancreas invasion remains uncommon [1, 2]. Melanoma metastasis could befall in the liver (42.9%), gastrointestinal region (20.7%), adrenal glands (8.5%), pancreas (2.3%), spleen (6.7%), or multiple spots (18.8%). Metastasis from stage IV melanoma was demonstrated to be the secondary malignancies as for abdominal organ [3]. We describe the case of duodenal metastasis with pancreas head invasion from the right thigh (lower limb) skin melanoma (Clark level IV) which was resected 3 years ago. Melanoma excision was associated with a right inguinal lymphadenectomy. Our findings will be present in this matter. The result is discussed and was reviewed in reference to other publications.
Case Report
Caucasian 62 elderly female was registrated in our hospital and underwent investigations because of persistent high grade fever episodes. A very high suspicious mass of tumor was incidental identified and described to the descending duodenum and head of pancreas in screening PET-CT scan, after extended surgical removal of skin melanoma located on the right thigh (lower limb). Removal of the melanoma was associated with a right inguinal lymphadenectomy, when she was 59 years old. At that time pathological specimen confirmed as malignant melanoma Clark-Level 4, pT2aN1bM0 as TNM-Staging, positive for BRAF-Wild-type by Mutation Analysis. After a couple of months after the first surgery she also underwent removal of malignant skin melanoma from the back area. Pathological results from the second specimen confirmed as skin melanoma Clark-Level 2, pT1a as TNM-Staging. She received chemotherapy and heavy particle radiotherapy after surgery. No suspect mass was identified on regular follow-up. Two years later it showed a recurrence in the scar on the right thigh (lower limb) and right inguinal site. No suspect mass was identified on follow-up CT-Scan’s from head, lung and abdomen. She received immunotherapy and no additional chemotherapy or radiotherapy. Three years later after the first melanoma removal, with the age of 62, she underwent investigations because of uncommon persistent high grade fever episodes. From PET-CT scan was observed a tumor mass arising descending part of duodenum and pancreatic head (Figure 1).
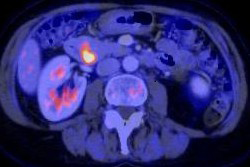
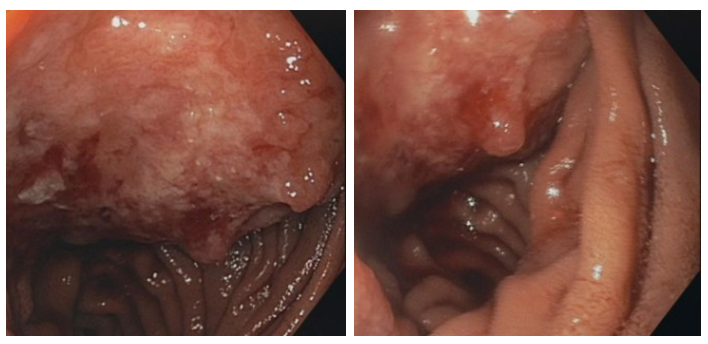
Endoscopic examination with ultrasonography showed a 30 mm tumor mass arising from the descending portions of the duodenum which had invaded the head of pancreas and caused loop obstruction (Figure 2).
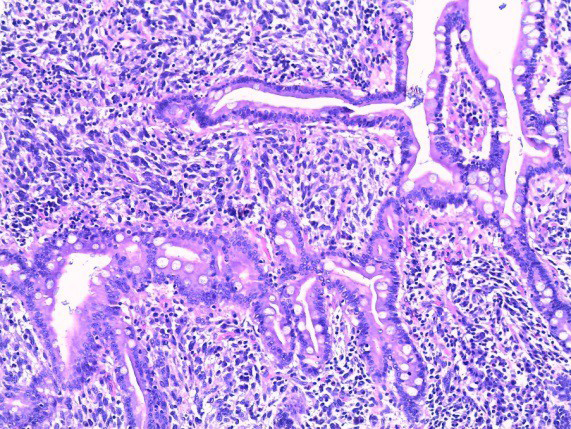
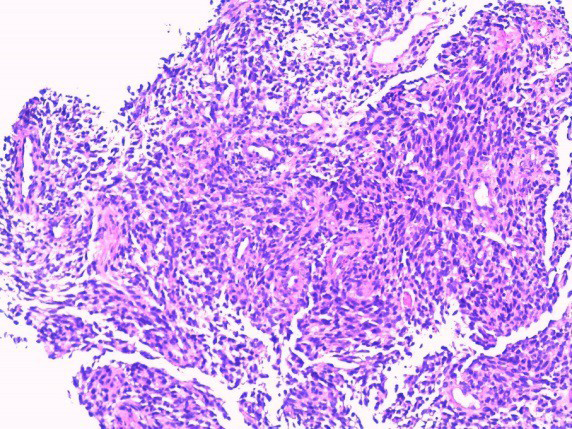
The biopsy revealed neoplastic cells with melanin granules and positive for Melan-A staining and SOX10 staining, suggesting existence of a metastatic skin melanoma. It was discovered no BRAF-Mutation. The colonoscopy showed not tumor finding. After tumor board procedure we strongly recommended surgical resection, and the patient accepted surgery. She underwent pylorus preserving pancreatico-duodenectomy. In the surgically resected Whipple specimen, the tumor in duodenum and head of pancreas was approximate to 4 x 5 cm large, solid and ulcerated, with invasion and alteration of all duodenal layers and invasion of pancreatic parenchyma. The mass was high solid and based of multiple nodules, although most of them were grayish and brownish. Hematoxylin-eosin staining revealed an infiltration by tumor cells inside duodenal mucosa (Figures 3 & 4). Histologically the tumor infiltrated all duodenal layers and the tissue around them.
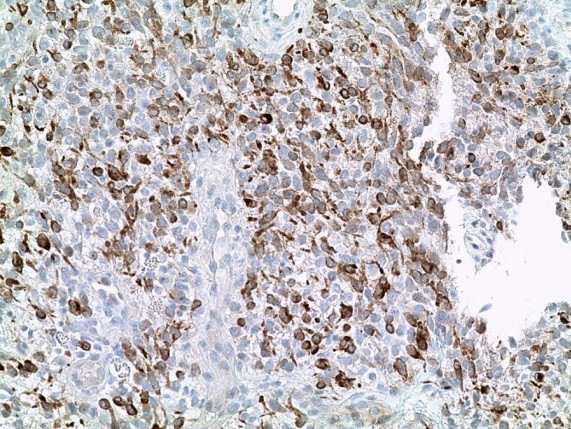
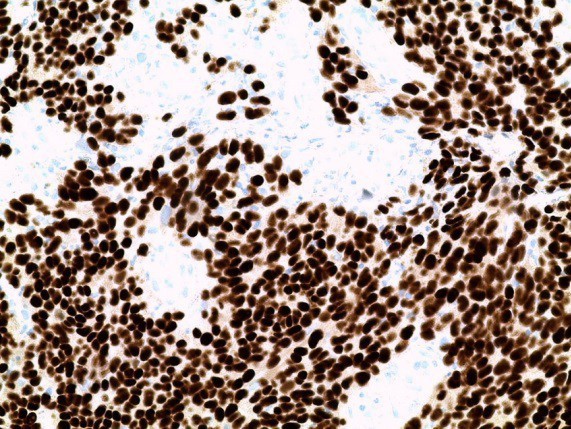
A high performance histological examination was performed to reach a valid and successful value of histology in the diagnosis of melanoma. Neoplastic cells were positive for expressing melanoma markers SOX10 and Melan-A staining’s (Figure 5 & 6). Immunocytochemistry and electronic microscopy findings confirmed the diagnosis of malignant melanoma, similar to the skin specimen from the right thigh. Therefore, the duodenal lesion was considered to be cutaneous melanoma metastasis from the right thigh. In conclusion, it can be said that melanoma was pathologically confirmed after intense workout. Resulting in a diagnosis of a late metastasizing skin melanoma to duodenum with pancreatic. Outpatient was well informed about final histological results.
The post operatory evolution was good. Patient could be released from the hospital after 13 days. Adjuvant chemotherapy was not performed because of previous immunotherapy. In this case we considered the therapy with adjuvant chemotherapy less worthy. It was decided to put forward an immunotherapy and she underwent the therapy with Ipilimumab and Nivoluma. No recur was registrated during 5 months close follow-up.
Discussion
Because patient access to health care in Europe and USA, the incidence diagnosis of skin melanoma is rapidly increasing in last decade; mortality still remains high [4].
The incidence rate in Asia, especially in Japan was reported to be 1-2 cases of melanoma per 100,000 persons per year [3, 5]. Pathological origin of melanoma arising from pigment- containing cells, mainly located in the cutaneous tissue. The very high aggressive malignancy of primary tumors was strong associated with excessive sunlight exposure, commonly over 90% occur on the skin. Gastrointestinal tract, mucosa eyes and meninges containing melanocytes, so melanoma can also develop from those tissues [6, 4]. Melanoma commonly metastasizes to skin, lymph nodes, and the digestive system. Metastasizing to a lung, the liver, the brain, and a bone are very exceptionally [7]. Stage 4 is the most advanced phase of the tumor, and means the cancer has spread to distance regions of the body, beyond the regional lymph nodes. The most commonly sites to abdominal organ metastasis from stage 4 melanoma were registrated to the liver with 42.9%, gastrointestinal tract 20.7%, adrenal gland tissue 8.5%, pancreas 2.3%, spleen 6.7%, or multiple sites 18.8% [3]. Metastasizing to gastrointestinal system ordinarily has an asymptomatic course or careless symptoms; frequently, clinical presentation is related when complications occur. Corresponding to post-mortem evidence, metastasizing melanoma to small bowel, colon or stomach are the most frequent localizations represent 50-60% of cadaveric studies, and usually suggest the expression of an advanced and widespread disease [6, 4]. Alone 1-9% of overall metastasizing cutaneous melanoma to gastrointestinal organs are diagnosed during lifetime [4, 8, 9]. All along of diagnosis, in more than 50% of patients, extra intestinal metastases are already recorded [10]. Supposing, intestinal metastases frequently arise 3-6 years after primary excision of skin melanoma.
In our patient, some lymph nodes from the right inguinal region were positive at the time of primary cutaneous excision on the right thigh (lower limb). This report described a duodenal metastasis from melanoma, 3 years later after primary skin melanoma excision. Gastrointestinal metastases are from time to time already present at primary skin examination or in every way 6 months after detection. [10, 11, 12]. Symptomless period between surgical skin excision of primary melanoma and the diagnosis of gastrointestinal metastases lasts between 6-90 months [13, 14]. This report described recurrent unclear episodes of fever, without digestive manifestation. Those episodes were described three years later after the primary melanoma excision. Because of persistent high grade fever episodes, our patient underwent a screening investigation using PET-CT- scan. A very high suspicious mass of tumor was incidental identified and described in the descending duodenum and head of pancreas after PET-CT scan. Diagnosis of duodenal metastasis from skin melanoma was confirmed after tissue sample during upper endoscopy. Colonoscopy was performed and showed not tumor finding. Detection of metastasizing skin melanoma to gastrointestinal organs it is better realized performing whole- body PET-CT imaging with fluorodeoxyglucose, because of higher sensitivity and specificity than does conventional CT [15].
Many specialists recommend that PET-CT should be the main staging study for recurrent disease [16]. The sensitivity rate of CT scan for detection of intestinal melanoma lay by 60-70% [12]. Complete endoscopic examination of the duodenum associated with endo-sonography and biopsy is non-invasive, and is a mandatory procedure for diagnosis of duodenal tumors [17]. Colonoscopy is also mandatory to exclude other conditions. Anyway, the small bowel tract is not easily examined by endoscopy. The sensitivity to detect metastatic tumors to the small bowel is every so often limited [18, 19]. An appropriate combination of imaging techniques and endoscopy is suggested to raise the sensitivity and specificity of diagnosis, and patients benefit from it. The process of determining the nature of disease is finally made by histological examination. Immunohistochemistry is the most common application of immunostaining. Immunohistochemistry staining, such as SOX10 and Melan- A, are used in histology to detect the presence of specific protein markers, which can assist the high accurate tumor classification, and certifying the diagnosis of metastatic melanoma. Precise preoperative diagnosis and evaluation of the extent to intestinal metastases, including neighboring organ invasion such pancreas, is essential when selecting patients for surgery , or planning the surgical procedure [12]. Surgical removal is the treatment of choice in all patients with respectable metastasizing melanoma to the gastrointestinal tract. Immunotherapy is the first-line non- surgical therapeutic approach. It is recommended by eligible patients with histologically confirmed metastatic melanoma and positive BRAF-mutant. A durable clinical benefit was demonstrated with combination of immunotherapy and chemotherapy, radiotherapy, or targeted molecular therapy . Immunotherapy is better tolerated compared to common chemotherapy [20]. Immunotherapy with Nivolumab, vemurafenib, ipilimumab, and trametinib (mekinist) has been authorized in Europe for therapy of metastasizing melanoma.
Even if our patient did not undergo supporting chemotherapy because she was encountered before such compliance, these medical agents have raised prognosis in comparable patient. Regular follow-up care is mandatory. It involves regular medical checkups, which may include a physical exam, blood tests, and imaging tests. The early diagnosis of intestinal metastasizing skin melanoma is deciding. Despite modern diagnostic techniques, premature detection of melanoma metastasis to small-bowel still remains a laborious challenge for medicine. Patients with a history of cutaneous melanoma who present unspecific clinical picture should be investigated to prevent gastrointestinal metastases. Metastasizing intestinal skin melanoma to the small bowel exposes late set of symptoms in evolution of the disease, estimating a low chance of recovery and survival.
Conclusion
Given the latest development in radiology, imaging and endoscopy, preoperative assessment of duodenal metastases extent using superior endoscopy with biopsy, associating CT- scan and PET-CT are very important for determining clinical tactics. However, to date, the treatment for advanced cutaneous melanoma is still unclear; although surgical removal is the treatment of choice in all patients with respectable metastasizing to the gastrointestinal tract. A high degree of suspicion is required to make an advanced pre-operative diagnosis of metastasizing skin melanoma to the duodenum, even if other acute accompanying symptom was reported.
PET-CT scan should be done in patients with a history of metastasizing cutaneous melanoma and nonspecific symptoms.
Conflict of Interest
No conflict of interest was declared. All authors read and approved the final manuscript.
Ethical Standards Compliance
The patient was informed according with the ethical standards laid down in the 1964 Declaration of Helsinki andits later amendments. Human rights All procedures have been performed and the patient gave her permission.
Fund
Exist no source of funds.
References
-
Schuchter LM, Green R, Fraker D (2000) Primary and metastatic diseases in malignant melanoma of the gastrointestinal tract. Curr Opin Oncol 12(2): 181-185.
-
Serin G, Doganavsargil B, Caliskan C, Akalin T, Sezak M, et al. (2010) Colonic malignant melanoma, primary or metastatic? Case report. Turk J Gastroenterol 21(1): 45- 49.
-
Tamaki T, Dong Y, Ohno Y, Sobue T, Nishimoto H, et al. (2014) The burden of rare cancer in Japan: application of the RARECARE definition. Cancer Epidemiol 38(5): 490-495.
-
King DM (2006) Imaging of metastatic melanoma. Cancer Imaging 6(1): 204-208.
-
Tomizuka T, Namikawa K, Higashi T (2017) Characteristics of melanoma in Japan: a nationwide registry analysis 2011-2013. Melanoma Res 27(5): 492- 497.
-
Ettahri H, Elomrani F, Elkabous M, Rimani M, Boutayeb S, et al. (2015) Duodenal and gallbladder metastasis of regressive melanoma: a case report and review of the literature. J Gastrointest Oncol 6(5): E77-81.
-
Barth A, Wanek LA, Morton DL (1995) Prognostic factors in 1,521 melanoma patients with distant metastases. J Am Coll Surg 181(3): 193-201
-
Kandemır NO, Bahadir B, Bektas S, Barut F, Yurdakan G, et al. (2011) Malignant melanoma associated with congenital melanocytic nevus and diagnosed with intestinal metastases: two case reports. Turk J Gastroenterol 22(1): 77-82.
-
Lo AA, Peevey J, Lo EC, Guitart J, Rao MS, et al. (2015) Isolated gallbladder intramucosal metastatic melanoma with features mimicking lymphoepithelial carcinoma. Int J Surg Pathol 23(5): 409-413.
-
Retsas S, Christofyllakis C (2001) Melanoma involving the gastrointestinal tract. Anticancer Res 21(2B): 1503- 1507.
-
Elsayed AM, Albahra M, Nzeako UC, Sobin LH (1996) Malignant melanomas in the small intestine: a study of 103 patients. Am J Gastroeneterol 91(5): 1001-1006.
-
Bender GN, Maglinte DD, McLarney JH, Rex D, Kelvin FM (2001) Malignant melanoma: patterns of metastasis to the small bowel, reliability of imaging studies, and clinical relevance. Am J Gastroenterol 96(8): 2392-2400.
-
Wade TP, Goodwin MN, Countryman DM, Johnson FE (1995) Small bowel melanoma: extended survival with surgical management. Eur J Surg Oncol 21(1): 90-91.
-
GG Caputy, Donohue JH, Goellner JR, Weaver AL (1991) Metastatic melanoma of the gastrointestinal tract: results of surgical management. Arch Surg 126(11): 1353-1358.
-
Tatlidil R, Mandelkern M (2001) FDG-PET in the detection of gastrointestinal metastases in melanoma Melanoma Res 11(3): 297-301.
-
Swetter SM, Carroll LA, Johnson DL, Segall GM (2002) Positron emission tomography is superior to computed tomography for metastatic detection in melanoma patients. Ann Surg Oncol 9(7): 646-653.
-
Tarantino L, Nocera V, Perrotta M, Balsamo G, Schiano A, et al. (2007) Primary small-bowel melanoma: color Doppler ultrasonographic, computed tomographic, and radiologic findings with pathologic correlations. J Ultrasound Med 26(1): 121- 127.
-
Crippa S, Bovo G, Romano F, Mussi C, Uggeri F (2004) Melanoma metastatic to the gallbladder and small bowel: report of a case and review of the literature. Melanoma Res 14(5): 427-430.
-
Washington K, McDonagh D (1995) Secondary tumors of the gastrointestinal tract: surgical pathologic findings and comparison with autopsy survey. Mod Pathol 8(4): 427-433.
-
Ralli M, Botticelli A, Visconti IC, Angeletti D, Fiore M, et al. (2020) Immunotherapy in the Treatment of Metastatic Melanoma: Current Knowledge and Future Directions. J Immunol Res 2020: 9235638.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient