Antegrade Gastric Variceal Embolization Simultaneously With Tips in Treatment of Patients with Acute Gastric Variceal Bleeding Having Unfavorable Gastric Variceal Anatomy
Gastric varices bleed at a lower Porto systemic pressure, have more catastrophic consequences and associated with large Porto systemic shunts. Occluded retrograde Trans-venous obliteration (RTO) is the mainstay of therapy for gastric variceal bleeding refractory to endoscopic therapy. A favorable afferent (Kiyosue type 1) and efferent (Kiyosue type A) anatomy of gastric varices is required for successful and safe RTO. Complex modifications in the RTO procedure are required for unfavorable afferent and efferent anatomies with high failure rates. RTO is not feasible in a type D efferent anatomy. RTO may aggravate potential complications associated with portal hypertension (ascites, catastrophic esophageal variceal bleeding). Antegrade gastric variceal embolization in adjunct to TIPS placement offers a safe, easier and effective alternative to modified RTO for gastric varices with unfavorable afferent and efferent anatomy. Concomitant placement of a TIPS stent leads to portal decompression and diminishes the risks associated with aggravation of portal hypertension. In this review, we discuss the anatomic and hemodynamic classification of gastric varices and describe the advantages of antegrade embolization (+TIPS) over RTO for management of gastric variceal bleeding in patients with complex variceal anatomies.
Introduction
Acute gastric variceal (GV) bleeding is one of the dreaded complications of portal hypertension. Pharmacological and endoscopic control of bleed is the desired first line of management [1]. Trans-jugular Intrahepatic Porto systemic Shunt (TIPS) and Retrograde Trans venous Obliteration (RTO) are reserved for refractory bleeding [2]. GV are redundant embryonic Porto systemic collaterals which become functional in patients with portal hypertension [3].
Type 2 gastro esophageal varices (GOV-2) and type 1 isolated gastric varices (IGV-1) [Sarin Classification] are located in the bare area of the stomach and drained via left inferior phrenic vein (LIPV) into the left renal vein (LRV) with formation of large shunts. However, alternate efferent drainage directly into inferior vena cava (IVC) via catheterizable shunts (gastrocaval shunts) or small non-catheterizable veins may also be seen [4]. Kiyosue, et al. classified these varices based on their afferent (types 1,2&3) and efferent anatomy(types A-D) (Table 1) [5].
| Anatomy | Description | Problems faced in conventional RTO | Modified techniques of RTO proposed | Advantages of TIPS + Antegrade embolization over modified RTO |
|---|---|---|---|---|
| Afferent | ||||
| A | Single afferent gastric vein (LGV/PGV/SGV) | None, provided there is feasible efferent anatomy | Reduction in portal pressure due to TIPS placement. BRTO may lead to worsening of ascites and catastrophic esophageal variceal bleeding | |
| B | Multiple afferent gastric veins | Persistent flow in the varices after efferent embolization through the high pressure afferent vein. The low pressure afferent vein acts as the new efferent. | embolization of the afferent system via antegrade route | Entire procedure can be done with a single antegrade transjugular access. Separate antegrade access (transjugular/trans hepatic) required in modified BRTO in addition to the retrograde trans femoral access. |
| C | A separate afferent vein drains directly into the shunt without communication to the gastric varices. | Administered sclerosant will flow into the low pressure afferent vein rather than the gastric varices and cause reflux into the portal system | Separate afferent vein that drains directly into the shunt has to be embolized by antegrade route | Entire procedure can be done with a single antegrade transjugular access. Separate antegrade access (transjugular/trans hepatic) required in modified BRTO in addition to the retrograde trans femoral access. |
| Efferent | ||||
| 1 | Single draining shunt (gastro renal >gastrocaval) which drains directly into the LRV/IVC | None, provided there is feasible afferent anatomy, feasible efferent and left renal vein orientation. | Reduction in portal pressure due to TIPS placement. BRTO may lead to worsening of ascites and catastrophic esophageal variceal bleeding | |
| 2 | A single shunt, and one or multiple collateral veins. The collateral veins drain into the right atrium (supra diaphragmatic) or IVC (infra diaphragmatic), but do not form a catheterizable shunt. | Non target embolization into the systemic circulation through the efferent collaterals | 1) For small collaterals, the occlusion balloon can be advanced beyond the draining shunt before injection of sclerosant | Advancing occlusion balloon beyond collaterals/ separate catheterisation and coil embolization of collateral veins is tedious and time consuming. Partial embolization may lead to systemic embolization of sclerosant. Afferent embolization of varices has less risk of systemic embolization of sclerosant |
| 2) For large collaterals, separate coil embolization of the collateral is done before injection of sclerosant | ||||
| 3 | Efferent drainage of varices by both gastro renal and gastrocaval shunts | Non target embolization into the systemic circulation through the gastrocaval shunt | 1) Smaller gastrocaval shunts may be embolised with coils via the gastro renal shunt prior to injection of sclerosant | Separate catheterisation and coil/balloon occlusion of gastrocaval shunt is tedious and time consuming. Partial embolization may lead to systemic embolization of sclerosant. Afferent embolization of varices has less risk of systemic embolization of sclerosant |
| 2) Larger gastrocaval shunts has to be catheterized separately from IVC via IJV route and separately occluded with a balloon prior to injection of sclerosant via the gastro renal shunt | ||||
| 4 | Efferent drainage via multiple small collateral veins into right atrium (supra diaphragmatic) or IVC (infra diaphragmatic) | No catheterizable efferent is present | Retrograde obliteration cannot be done. Antegrade embolization is the only available treatment modality | Retrograde catheterisation is not feasible. Antegrade embolization is the only available treatment |
Table 1: Anatomical description of Kiyosue afferent and efferent anatomies of gastric varices, problems faced with conventional R
Table 1: Anatomical description of Kiyosue afferent and efferent anatomies of gastric varices, problems faced with conventional Retrograde transvenous obliteration (RTO), various modified retrograde modalities of obliteration described and advantage of Transjugular intrahepatic portosystemic shunt (TIPS) + antegrade embolization over modified retrograde obliteration [RTO = retrograde transvenous obliteration, TIPS = Transjugular intrahepatic portosystemic shunt].
GV are large diameter venous channels with a propensity to bleed even in low portal pressure (HVPG<12mmHg) [6]. TIPS alone is not an effective modality to control bleeding from these varices. RTO has gained much success in recent years. However, shunt closure without portal decompression may lead to worsening of portal hypertension and associated symptoms (ascites, catastrophic esophageal variceal bleeding) [7].
In RTO, a compliant balloon/ plug are used to occlude the outflow of the shunt prior to sclerosant injection into the varices. Stasis of the sclerosant within the varices without portal/ systemic non-target embolization is critical. Placement of an afferent occlusion device requires a favorable afferent GV anatomy. An unfavorable afferent anatomy makes cannulation and long sheath placement time- consuming and inconvenient. Additionally, they may require adjunctive placement of micro-catheters and embolization coils to prevent non-target embolization (modified RTO) [8]. A Kiyosue type D efferent anatomy has no catheterizable efferent and RTO is not feasible [9]. Presence of multiple afferents (Kiyosue type 2) or direct shunt bypassing the varices (Kiyosue type 3) increases the chances of incomplete variceal obliteration and non-target embolization.
Antegrade embolization (AE) of GV can be done via a percutaneous or a trans-jugular route (trans-TIPS). Concomitant placement of a TIPS stent with AE leads to control of GV bleeding with no significant increase in portal pressure [10]. AE may be performed in unfavorable variceal anatomies where performing modified RTO may not be feasible or is cumbersome.
Endoscopic Classification of Gastric Varices
Based on anatomical location and association with esophageal varices (EV), GV is classified into four types (Sarin’s classification) [11]. GOV consists of GV that are associated with EV and may be located along the lesser curvature (GOV-1) or along the greater curvature (GOV-2) of stomach. IGV may be present along the greater curvature (IGV-1) or the pylorus (IGV-2) of stomach.
Hemodynamic Anatomy of Gastric Varices
Decision regarding interventional approach requires a proper knowledge of the afferent and efferent anatomy of the concerned GV. Afferent supply to the GV is from the portal vein via one or multiple gastric veins. The efferent drainage is via draining veins/shunts into the systemic circulation.
Drainage Pathway for GOV-1: GOV-1 drain via the gastro esophageal venous plexus into the superior vena cava (SVC). The major afferent supply of these varices is from the left gastric vein (LGV) Figure 1. These are uphill varices and bleeding from these varices can be attributed to high portal pressure (Wall Tension = Pressure x Radius of vessel). Reduction of portal pressure (placement of a TIPS stent) may be sufficient for controlling refractory bleed from these varices.
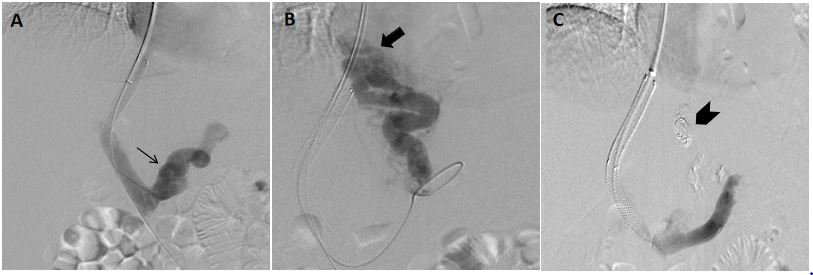
Figure 1: A patient with active variceal bleeding with endoscopy suggestive of large type 1 gastroesophageal varices (GOV-1). A,B) Post TIPS stent deployment antegrade splenoportogram revealed persistence of varices with predominant afferent supply from the left gastric vein (LGV) (arrow). [Type 1 afferent anatomy]. The drainage of the varices is via the gastro esophageal venous plexus. GOV-1 is high pressure low flow systems and generally decompresses after TIPS placement. However, there was persistence of flow in the varices after TIPS deployment in this case. Afferent glue and coil embolization of the varices was done. C) Post embolization splenoportogram showed non-opacification of the varices. (Arrowhead - coil and glue cast) [TIPS = Transjugular Intrahepatic Porto systemic Shunt].
Drainage Pathway for GOV-2 and IGV-1: GOV-2 and IGV-1 are unique in the fact that they are located in the bare area of stomach. Efferent drainage is via LIPV which may drain directly into the LRV (gastro-renal shunt), IVC (gastrocaval shunt/ non- catheterizable collaterals) (Figures 2-5). Afferent supply is by one or multiple gastric veins [posterior (PGV) & short (SGV) gastric veins are more common afferent draining veins]. They are downhill low pressure varices and bleeding may be attributed to large diameter of the varices (Wall Tension = Pressure x Radius of vessel). RTO is the treatment of choice for refractory bleed from these varices.
![Figure 2: A patient with active variceal bleeding with endoscopy suggestive of large type 2 gastroesophageal varices (GOV- 2). A) Antegrade splenoportogram showed the predominant afferent supply of the gastric varices in the cardio-fundal region (GOV-2) to be arising from the short gastric vein (SGV). Also multiple smaller afferent branches were seen arising directly from the splenic vein with formation of varices in the body and pylorus of stomach suggestive of type 2 isolated gastric varices (IGV-2) (arrow). The presence of IGV-2 suggests sinistral portal hypertension as the etiology. However, no evidence of portal vein thrombosis was seen. B) Delayed portography images show absence of catheterizable shunt with efferent drainage of the varices (GOV-2 and IGV-2) via left inferior phrenic vein and small direct branches into IVC. (Block arrows) A type D efferent anatomy makes retrograde obliteration of varices not feasible in this case. C) Post TIPS placement splenoportogram showed persistent opacification of the GOV-2 varices. Note the active extravasation of contrast agent seen from the GOV-2 varices (arrowhead). D) No contrast opacification of gastric varices was seen on the splenoportography images after glue injection and TIPS placement. Glue cast is seen in the SGV. [TIPS = Transjugular Intrahepatic Portosystemic Shunt].](/fulltextimages/10504/fig_2.png)
Figure 2: A patient with active variceal bleeding with endoscopy suggestive of large type 2 gastroesophageal varices (GOV- 2). A) Antegrade splenoportogram showed the predominant afferent supply of the gastric varices in the cardio-fundal region (GOV-2) to be arising from the short gastric vein (SGV). Also multiple smaller afferent branches were seen arising directly from the splenic vein with formation of varices in the body and pylorus of stomach suggestive of type 2 isolated gastric varices (IGV-2) (arrow). The presence of IGV-2 suggests sinistral portal hypertension as the etiology. However, no evidence of portal vein thrombosis was seen. B) Delayed portography images show absence of catheterizable shunt with efferent drainage of the varices (GOV-2 and IGV-2) via left inferior phrenic vein and small direct branches into IVC. (Block arrows) A type D efferent anatomy makes retrograde obliteration of varices not feasible in this case. C) Post TIPS placement splenoportogram showed persistent opacification of the GOV-2 varices. Note the active extravasation of contrast agent seen from the GOV-2 varices (arrowhead). D) No contrast opacification of gastric varices was seen on the splenoportography images after glue injection and TIPS placement. Glue cast is seen in the SGV. [TIPS = Transjugular Intrahepatic Portosystemic Shunt].
![Figure 3: Retrograde obliterated venogram and obliteration done in two patients with acute gastric variceal bleeding with endoscopy suggestive of large type 2 gastro esophageal varices (GOV-2). A,B) A small diameter collateral vein (arrow) was seen arising from the large gastro renal shunt (block arrow) suggestive of a type B1 efferent anatomy. Sclerosant injection was done after advancing the tip of the catheter distal to the origin of the collateral vein. C,D,E) In a different patient, a large diameter collateral vein (arrow) was seen arising from the gastro renal shunt (block arrow) suggestive of a type B2 efferent anatomy. Coil embolization (arrowhead) of the collateral vein was done prior to injection of sclerosant (curved arrow). These modified BRTO techniques are time consuming and have increased chances of non-target systemic sclerosant embolization. [BRTO = Balloon occluded retrograde transvenous obliteration].](/fulltextimages/10504/fig_3.png)
Figure 3: Retrograde obliterated venogram and obliteration done in two patients with acute gastric variceal bleeding with endoscopy suggestive of large type 2 gastro esophageal varices (GOV-2). A,B) A small diameter collateral vein (arrow) was seen arising from the large gastro renal shunt (block arrow) suggestive of a type B1 efferent anatomy. Sclerosant injection was done after advancing the tip of the catheter distal to the origin of the collateral vein. C,D,E) In a different patient, a large diameter collateral vein (arrow) was seen arising from the gastro renal shunt (block arrow) suggestive of a type B2 efferent anatomy. Coil embolization (arrowhead) of the collateral vein was done prior to injection of sclerosant (curved arrow). These modified BRTO techniques are time consuming and have increased chances of non-target systemic sclerosant embolization. [BRTO = Balloon occluded retrograde transvenous obliteration].
![Figure 4: A patient with active variceal bleeding with endoscopy suggestive of large type 2 gastroesophageal varices (GOV-2). A) Antegrade splenoportography images depicted the predominant afferent supply of the gastric varices from left gastric vein (LGV), posterior gastric vein (PGV) and short gastric vein (SGV) (arrows). B,C) The efferent drainage of the varices were via a large gastro renal shunt as well as large collateral veins (block arrows). A type B3 efferent anatomy increases the chances of systemic non-target embolization of sclerosants during conventional BRTO. D) Embolization of the afferents was done using multiple coils (arrowhead) and glue (triangle). E) Post TIPS post embolization splenoportogram showed non opacification of gastric varices. However, a smaller afferent (arrow) was seen arising directly from the splenic vein and draining directly into and opacifying the gastro renal shunt. This was suggestive of a type 3 afferent anatomy. A type 3 afferent anatomy has increased chances of embolization of sclerosant into the portal vein during retrograde obliteration. [TIPS = Transjugular Intrahepatic Portosystemic Shunt].](/fulltextimages/10504/fig_4.png)
Figure 4: A patient with active variceal bleeding with endoscopy suggestive of large type 2 gastroesophageal varices (GOV-2). A) Antegrade splenoportography images depicted the predominant afferent supply of the gastric varices from left gastric vein (LGV), posterior gastric vein (PGV) and short gastric vein (SGV) (arrows). B,C) The efferent drainage of the varices were via a large gastro renal shunt as well as large collateral veins (block arrows). A type B3 efferent anatomy increases the chances of systemic non-target embolization of sclerosants during conventional BRTO. D) Embolization of the afferents was done using multiple coils (arrowhead) and glue (triangle). E) Post TIPS post embolization splenoportogram showed non opacification of gastric varices. However, a smaller afferent (arrow) was seen arising directly from the splenic vein and draining directly into and opacifying the gastro renal shunt. This was suggestive of a type 3 afferent anatomy. A type 3 afferent anatomy has increased chances of embolization of sclerosant into the portal vein during retrograde obliteration. [TIPS = Transjugular Intrahepatic Portosystemic Shunt].
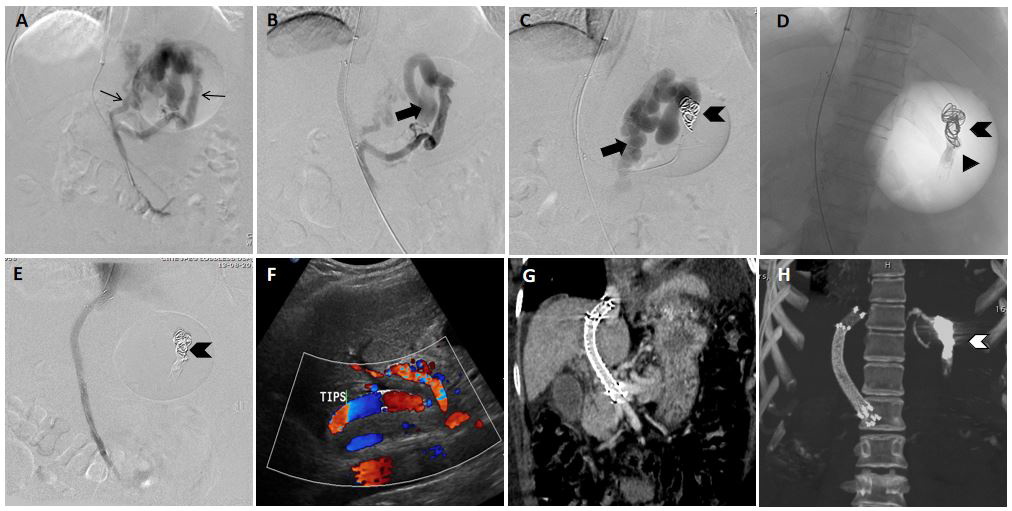
Figure 5: A patient with active variceal bleeding with endoscopy suggestive of large type 2 gastroesophageal varices (GOV- 2). A) Antegrade splenoportography images depicted the predominant afferent supply of the gastric varices from left gastric vein (LGV), posterior gastric vein (PGV) and short gastric veins (SGV) (arrows) suggestive of a type 2 afferent anatomy. A type 2 afferent anatomy may have persistence of flow into the gastric varices after retrograde obliteration B) Efferent drainage of the varices was via a large gastrorenal shunt (GRS) (type A efferent anatomy) C) Post coil (arrowhead) deployment splenoportography images show persistent opacification of gastric varices and gastro renal shunt (block arrow). D) Spot image post glue embolization showing glue cast proximal to the deployed coil. E) Post glue and coil deployment portography images show no contrast opacification of gastric varices. F,G,H) Follow up Doppler and CECT scan after one month shows normal flow and contrast opacification of the stent. Note the coil and glue cast (white arrowhead).
Drainage Pathway of IGV-2: IGV-2 is present in the pylorus of stomach and the first part of duodenum. They generally develop in the setting of isolated splenic vein hypertension (due to portal vein thrombosis). Efferent drainage is generally via small venous channels into the IVC. Afferent supply to these varices is via the SGV/gastroepiploic vein/other small collateral veins directly originating from the distal splenic vein in Figure 2. Relieving the portal vein occlusion is the treatment modality of choice to control refractory bleed from these varices.
Hemodynamic Classification of Gastric Varices
In 2003, Kiyosue classified gastric varices based on their afferent and efferent drainage pattern [5].
Classification Based on Afferent Anatomy
Three types of gastric variceal afferent anatomy were described:
Type 1: The simplest anatomical variant comprising of a single afferent vein supplying the gastric varices (LGV/PGV) in Figure 1 RTO can be easily done provided the efferent anatomy is conducive.
Type 2: Multiple afferent veins supply the gastric varices in Figure 5. The pressure in the afferents is different as they originate from different points in spleno-portal axis. Retrograde venography is unable to demonstrate all the afferents and will only opacify the afferent with least pressure. Even after efferent obliteration, there will be persistent flow in the GV with low pressure afferent vein acting as the new efferent. A follow up adjunctive embolization of afferents using a portal venous access (afferent route) is necessary.
Type 3: A direct shunt bypassing the varices is present between the spleno-portal axis (afferent) and the systemic shunt (efferent) in addition to a type 1 or type 2 afferent anatomies Figure 4. This additional shunt is the pathway of least resistance and acts as the conduit for non-target embolization of sclerosant into the portal vein during RTO. Afferent embolization of the direct shunt is essential prior to RTO. TIPS in adjunct to antegrade embolization can treat gastric varices with Type 2 and Type 3 anatomy in a single sitting while RTO requires multistage treatment (antegrade embolization of varices in addition to retrograde occlusion of shunt).
Classification Based On Efferent Anatomy
Four types of gastric variceal efferent anatomy have been described.
Type A: A single shunt (more commonly, a gastro renal shunt) acts as the soul outflow conduit for the varices. Figure
5 unfavorable orientation of the efferent vein in relation to the renal vein poses challenge in cannulation and long sheath placement.
Type B: A single shunt and one or multiple collateral veins act as the outflow tract. The collateral veins drain into the systemic circulation via the pericardiophrenic collateral pathway (supra diaphragmatic) or into IVC (infra- diaphragmatic), but do not form a catheterizable shunt. The veins may be small (B1) in Figure 3, medium (B2) in Figure 3 or large (B3) in Figure 4 but do not form a catheterizable shunt. In cases with high flow draining veins (B2, B3), the draining vein has to be occluded first (coils preferably) before sclerosant injection. In cases of insufficient embolization, there are high chances of sclerosant embolization into the systemic circulation.
Type C: Efferent drainage of varices is via both gastro renal and gastrocaval shunts. This requires occlusion of both the shunts (both trans-jugular and trans-femoral routes are used, one for each shunt) prior to injection of sclerosant. In cases of insufficient occlusion of one/both shunts, there are high chances of sclerosant embolization into the systemic circulation.
Type D: Efferent drainage of the varices is via multiple small collateral veins with no catheterizable shunts Figure 2. Retrograde obliteration cannot be done in these cases. Antegrade embolization is the only available treatment modality. In Type B and Type C efferent anatomies, TIPS + ATE does not require the additional challenging step of occlusion of the additional efferent and has reduced chances of systemic embolization. In Type D efferent anatomy, antegrade embolization is the only feasible modality.
Problems Faced with Modified Occluded Retrograde Balloon Obliteration Techniques
Various modified techniques of RTO have been described for challenging variceal anatomies [8]. However, the described techniques may require additional access, tedious collateral cannulation and the placement of coils may not completely prevent systemic non target embolization via large collaterals. In Kiyosue Type D efferent, retrograde obliteration of varices is not feasible. Retrograde trans- venous embolization of gastric varices leads to a sudden increase in portal pressure which may culminate into worsening of ascites or a fatal episode of upper GI bleeding from new/existing esophageal varices.
AE in Adjunct to Tips For GV
AE in adjunct to TIPS is a novel modality which involves placement of a TIPS stent in adjunct to variceal embolization from the portal venous side. The embolising agent is selected based on the afferent anatomy of the varices. Various recent studies have shown that TIPS in adjunct to antegrade embolisation has better outcomes in management of variceal bleeding in patients with gastric as well as gastroesophageal varices with increased survivability, reduced rebleeding rates and increased time to rebleed [10, 12, 13]. TIPS placement and variceal embolization act as synergistic processes. Increase in portal pressure due to shunt embolization is relieved by the TIPS stent placement. There are increased chances of TIPS dysfunction and liver failure after TIPS placement in patients with large Porto systemic shunts. AE leads to diversion of shunt flow towards the TIPS stent and normal liver parenchyma with reduced chances of post TIPS liver failure and TIPS dysfunction. Varied embolising agents may be used for AE based on the patient’s variceal anatomy. The procedure is safe with no significant incidence of non- target embolization [14]. The advantages of AE + TIPS over modified RTO for individual anatomic variants have been summarized in Table 1.
Conclusion
RTO is the treatment of choice for active GV bleeding that is refractory to endoscopic therapy. GV may be associated with afferent/efferent anatomies that are unfavorable for performing RTO. TIPS with AE may be adopted as an effective therapeutic modality for GV bleeding in patients with variceal anatomy unfavourable for performing RTO.
References
-
Garcia-Pagán JC, Barrufet M, Cardenas A, Escorsell A (2014) Management of gastric varices. Clin Gastroenterol Hepatol 12(6): 919-928.
-
Rajesh S, George T, Philips CA, Ahamed R, Kumbar S, et al. (2020) Transjugular intrahepatic portosystemic shunt in cirrhosis: An exhaustive critical update. World J Gastroenterol 26(37): 5561-5596.
-
Henry Z, Uppal D, Saad W, Caldwell S (2014) Gastric and ectopic varices. Clin Liver Dis 18(2): 371-388.
-
Kiyosue H, Ibukuro K, Maruno M, Tanoue S, Hongo N, et al. (2013) Multidetector CT anatomy of drainage routes of gastric varices: a pictorial review. Radiographics 33(1): 87-100.
-
Kiyosue H, Mori H, Matsumoto S, Yamada Y, Hori Y, et al. (2003) Transcatheter obliteration of gastric varices. Part 1. Anatomic classification. Radiographics 23(4): 911- 920.
-
Morrison JD, Mendoza-Elias N, Lipnik AJ, Lokken RP, Bui JT, et al. (2018) Gastric Varices Bleed at Lower portosystemic Pressure Gradients than Esophageal Varices. J Vasc Interv Radiol 29(5): 636-641.
-
Park JW, Yoo JJ, Kim SG, Jeong SW, Jang JY, et al. (2020) Change in Portal Pressure and Clinical Outcome in Cirrhotic Patients with Gastric Varices after Plug- Assisted Retrograde Transvenous Obliteration. Gut Liver 14(6): 783-791.
-
Kiyosue H, Mori H, Matsumoto S, Yamada Y, Hori Y, et al. (2003) Transcatheter obliteration of gastric varices: Part 2. Strategy and techniques based on hemodynamic features. Radiographics 23(4): 921-937.
-
Kiyosue H, Matsumoto S, Yamada Y, Hori Y, Okino Y, et al. (2004) Transportal intravariceal sclerotherapy with N-butyl-2-cyanoacrylate for gastric varices. J Vasc Interv Radiol 15(5): 505-509.
-
Yu J, Wang X, Jiang M, Ma H, Zhou Z, et al. (2019) Comparison of transjugular intrahepatic portosystemic shunt (TIPS) alone and combined with embolization for the management of cardiofundal varices: a retrospective study. Eur Radiol 29(2): 699-706.
-
Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK (1992) Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology 16(6): 1343-1349.
-
Gaba RC, Bui JT, Cotler SJ, Kallwitz ER, Mengin OT, et al. (2010) Rebleeding rates following TIPS for variceal hemorrhage in the Viatorr era: TIPS alone versus TIPS with variceal embolization. Hepatol Int 4(4): 749-756.
-
Qi X, Liu L, Bai M, Chen H, Wang J, et al. (2014) Transjugular intrahepatic portosystemic shunt in combination with or without variceal embolization for the prevention of variceal rebleeding: a meta-analysis. J Gastroenterol Hepatol 29(4): 688-696.
-
Schultheiß M, Giesler M, Maruschke L, Schmidt A, Sturm L, et al. (2019) Adjuvant Transjugular Variceal Occlusion at Creation of a Transjugular Intrahepatic Portosystemic Shunt (TIPS): Efficacy and Risks of Bucrylate Embolization. Cardiovasc Intervent Radiol 42(5): 729-736.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient