A Case of Autoimmune Hepatitis Chronic Liver Disease with Iron Overload
Autoimmune hepatitis (AIH) is a rare autoimmune disorder causing chronic inflammation in liver which affects all ages, both genders, and all ethnicities. It has a heterogenous presentation in which patients may either be asymptomatic, chronically ill or may present with acute liver failure [1]. The diagnosis should be considered in patients with acute or chronic liver dysfunction including patients with graft dysfunction after Liver Transplantation [1]. AIH does not have a signature diagnostic feature, and the diagnosis requires the presence of a constellation of typical features which can vary between patients with the same disease and can occur in other liver diseases. AIH like other inflammatory conditions is associated with increased ferritin levels (acute phase reactant) but normal transferrin saturation level. The presence of excessive ferritin in absence of high transferrin saturation helps differentiate secondary iron overload from hemochromatosis where transferrin saturation is high [2]. There are case reports of chronic liver disease and secondary iron overload. We report a rare case of chronic liver disease due to AIH and secondary iron overload leading to diagnostic dilemma encountered during our clinical practice.
Introduction
Autoimmune Hepatitis is a chronic progressive necro-inflammatory disease associated with circulating autoantibodies and high serum globulin levels. Clinical manifestations are variable ranging from elevated transaminases to liver cirrhosis or fulminant liver failure [3]. Chronic liver diseases due to NAFLD, chronic hepatitis B and C, Primary biliary cholangitis are associated with mild iron overload and near normal transferrin saturation [4]. Elevated ferritin levels being an acute phase reactant is also seen in inflammatory conditions but serum transferrin saturation is essentially normal [5]. Thus, in appropriate clinical setting very high transferrin saturation (>45%) is highly suggestive of Hereditary Hemochromatosis and serves as a threshold for HFE gene testing to diagnose hemochromatosis. Liver biopsy therefore becomes imperative to differentiate between primary hereditary hemochromatosis and secondary iron overload. Herein, we report a rare case of chronic liver disease due to autoimmune hepatitis and secondary iron overload which led to diagnostic dilemma and the therapeutic management in this patient.
Case Study
A 35 year old Indian male, tailor by occupation presented with chief complaints of yellowish discoloration of eyes and urine, easy fatiguability, and generalized weakness for the past one month, diffuse abdominal distension followed by pedal edema for the past 15 days. There was no prior history of fever, or associated pruritus. Patient denied any history of smoking, alcohol abuse, or any intake of complimentary and alternative medication, or, illicit drug abuse. Patient was born out of second degree consanguinuous marriage. The patient was married. On physical examination patient was alert and oriented with normal vital signs. He was icteric with pallor with bilateral pitting pedal edema. No skin pigmentation or brownish discoloration of skin was observed. Abdominal examination revealed hepatomegaly with liver span of 18 cm and moderated splenomegaly with shifting dullness present. Other systemic examination was within normal limit. His initial laboratory analyses revealed hemoglobin -7 gm/dl, TLC-7000 cell/mm3, platelet count of 1,00,000 cells/mm3, total bilirubin 15.6 gm/dl ,direct bilirubin 12.4 gm/dl, AST- 325 IU/ml, ALT-563 IU/ml and ALP-22O IU/ml, blood urea- 15 mg/dl and serum creatinine 0.8 mg/dl. Prothrombin/INR was 19.3/1.77. Viral hepatitis panel was negative and with negative history of alcohol consumption alcoholic hepatitis was ruled out. IgM anti CMV and EBV serology was negative. Direct coombs test and indirect coombs test was negative. Serum LDH -123 IU/ml. Serum ceruloplasmin was 43 mg/ dl, 24 hour urinary copper -10 mcg per 24 hours. Slit lamp examination showed no evidence of KF ring. Hemoglobin electrophoresis revealed normal Hemoglobin pattern with no evidence of hemoglobinopathy. Serum free T4-1.5 µIU/ml, serum T3 -0.7µIU/ml was within normal limit and TSH- 45.4 µIU/ml. Autoimmune hepatitis profile showed Anti-nuclear antibody positive with titre of 1:160 and anti LC-1 positive, other autoimmune markers like anti LKM1, anti-smooth muscle antibody and anti-mitochondrial antibody was negative, Serum Immunoglobulin G was elevated 2952 IU/ ml. Serum IgM, serum IgA, was within normal limit. Ascitic fluid cytology showed cell count 150 cells/mm3 with High SAAG low protein ascites. Urine routine microscopy was normal. Serum iron profile was done total iron-178 mcg/ dl ,Total iron binding capacity -181 mcg/dl, with markedly elevated serum ferritin >2,000 mcg/dl and transferrin saturation -98.3%. His serum vitamin B12 levels were normal. Ultrasound abdomen was done which showed liver size of 19 cm, coarse echoes and nodular liver surface with spleen size of 14.3 cm, portal vein -13.3 mm with peak systolic velocity 29 cm/sec, hepato-fugal flow with no evidence of thrombosis in splenoportal axis with presence of free fluid in the abdomen. The patient denied any history of diabetes, any prior blood transfusion or any similar complaints in the family. 2D Echocardiography was normal with ejection fraction-55%. Upper GI endoscopy showed small esophageal varices with no red colour signs and mild portal hypertensive gastropathy. The above stated laboratory findings now led to a dilemma in diagnosis with elevated transferrin saturation and hereditary hemochromatosis, or, positive autoimmune profile and elevated serum immunoglobulin levels and autoimmune hepatitis.
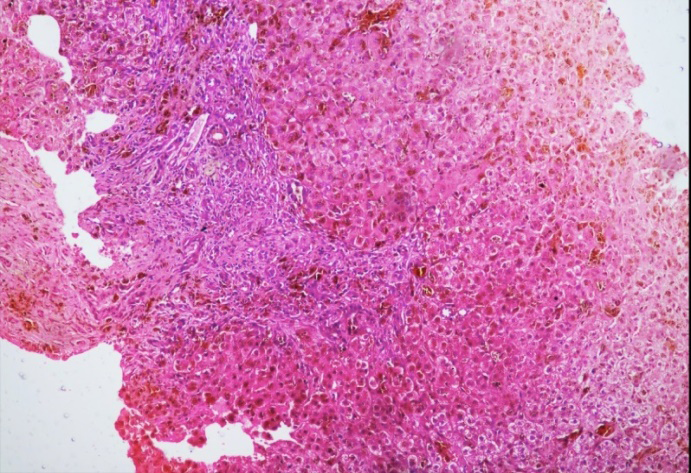
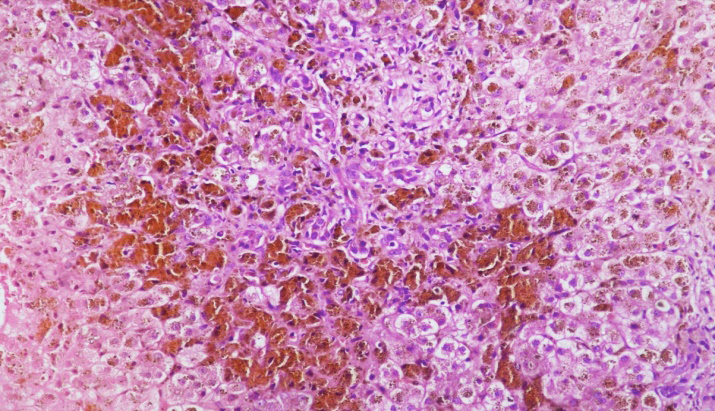
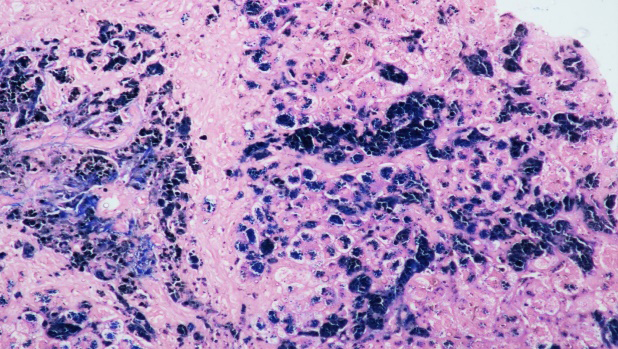
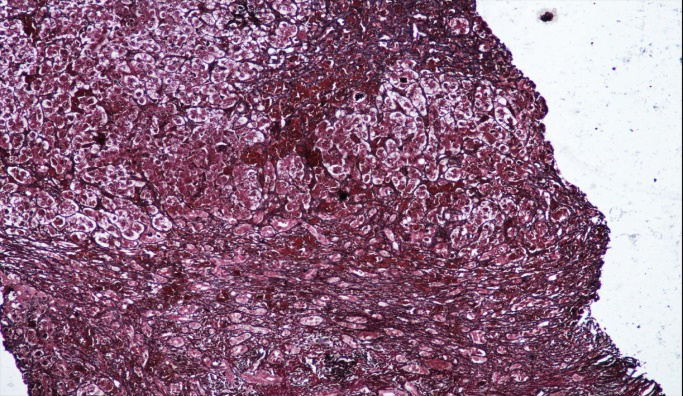
The patient then underwent transjugular liver biopsy which showed marked distortion of lobular architecture with few variably sized fibrous septa and formation of regenerative parenchymal nodules. Fibrous septa and portal areas show bile duct damage with increased inflammatory cells composed of lymphocytes and plasma cells and spill- over into periportal hepatocytes with interface hepatitis. Numerous hemosiderin laden macrophages seen within portal areas. Hepatocytes show intrahepatic granular iron deposition prominently in periportal and midzonal zones (zone 1 and 2). Hepatocytes show feathery degeneration, intrahepatic bile deposition along with canalicular bile, cholestatic and regenerative rosettes. Occasional foci of lobular inflammation are seen. Sinusoids are markedly dilated and distended with hemosiderin laden Kupffer cells. Focus of centrizonal congestion with hepatocytic dropout and perivenular hemosiderin laden macrophages is noted. Intrahepatic, sinusoidal, Kupffer cells, biliary epithelial cell and portal macrophage iron deposition are highlighted on Perl’s Prussian blue stain. So, the biopsy was suggestive of chronic hepatitis with advanced fibrosis (Fibrosis F-4, METAVIR staging), Hepatic and sinusoidal hemosiderosis {Iron stage 3 to 4 (Scheuer’s grading), intrahepatic, canalicular and ductular cholestasis. The biopsy was compatible with autoimmune hepatitis with extensive iron overload (parenchymal and Kupffer cell hemosiderosis). (Figure 1) Low power showing portal inflammation, interface hepatitis and brown pigment. (Figure 2) High power showing balloon degeneration, abundant hemosiderin pigment, rosette formation, ductular proliferation. (Figure 3) Perls stain highlight intrahepatic, sinusoidal, Kupffer cell, biliary epithelial cell and portal macrophage hemosiderin deposition. Figure 4-Reticulin stain showing fibrosis and nodule formation.
The patient also underwent HFE gene mutation analyses but was negative for C282Y and H63D Mutation. Other mutation analyses due to non-HFE hereditary hemochromatosis could not be done due to financial constraints.
So considering high transferrin saturation and elevated ferritin levels with features of hepatic, sinusoidal and Kupffer cell hemosiderosis with positive Antinuclear antibody and anti LC-1 positive with elevated serum immunoglobulin G levels and liver biopsy compatible with autoimmune hepatitis Simplified disease activity index -7, he was diagnosed as chronic liver disease due to AIH with secondary iron overload mixed pattern.
The patient was started on oral corticosteroid tab prednisolone at 1 mg/kg/day. Azathioprine was started one month after initiation of oral steroid therapy. After four months of initiation of steroid therapy his hemoglobin improved to 9 gm/dl and liver function tests improved to total bilirubin -2.3 mg/dl, direct bilirubin-1.8 mg/dl, AST -41 IU/ml, ALT- 44 IU/ml and ALP-141 IU/ml. Total protein 7.3 gm/dl and albumin-4.7 gm/dl.
Discussion
Autoimmune hepatitis is considered rare in Asia-Pacific region. In an Indian study by D Amarapurkar et al the prevalence of autoimmune hepatitis was 1.3% and 8.75% among all liver disease patients and chronic liver disease respectively [6]. AIH is a rare disease which affects all ages and ethnic groups with a female predominance (F:M ratio 3.6:1) [7]. Primary hemochromatosis is also unusual in India. The homeostatic iron regulator (HFE) gene C282Y mutations, common cause for hemochromatosis in Europe is considered almost non-existent in India. In an Indian study by A Koshy et al of the three cases reported with hereditary hemochromatosis only one was associated with C282Y HFE gene mutation and two cases were associated with hemojevulin mutations (HJV) [8]. We conducted an extensive Pubmed based research and found only two previously reported cases of autoimmune hepatitis with elevated transferrin saturation and secondary iron overload. To our knowledge this is an unusual case of autoimmune hepatitis with mixed pattern of iron overload.
Autoimmune diseases are considered in patients with autoantibodies with high ANA titres. Our patient presented with cholestatic pattern of Liver Function Tests. The patient presented with positive anti-nuclear antibody and anti-liver cytosol antibody positive with elevated serum immunoglobulin G levels and liver biopsy showing interface hepatitis, lymphocytes and plasma cell infiltration and rosette formation suggestive of autoimmune hepatitis. Autoimmune hepatitis is a highly treatable condition with response to immunosuppressive therapy. The mixed pattern of iron accumulation in biopsy presented a diagnostic challenge. Although uncommon, mixed pattern of iron accumulation can be seen in cases of severe iron overload and chronic liver diseases.
Autoimmune hepatitis is characterized by autoimmune inflammation of the liver mediated by reactive oxygen species and ferroptosis is associated with reactive oxygen species. Liver is main storage site for iron which is stored in the form of ferritin (major) and iron containing heme (minor). In iron overload states there are large accumulations of both ferritin and heme as seen in hereditary and secondary cases. Ferroptosis is defined as iron dependent cell death regulated by phospholipid peroxidation [9]. It results from abnormal iron metabolism involving the iron-storage protein ferritin. Ferritin has light and heavy hains which possesses iron oxidase activity thus converting iron from ferrous to ferric form and lowering the concentration of free iron in the cell. High levels of free iron are associated with lipid peroxidation. The role of ferritin is to capture free iron within its spacious storage core thus protecting the cell against potential damage caused by reactive oxygen species which further leads to DNA damage, protein denaturation, and lipid peroxidation. Under normal physiological conditions the production of lipid peroxides is inhibited by intracellular antioxidant enzyme selenium peroxidase glutathione peroxidase 4 [9]. In chronic liver disease such as seen in this patient due to reduced hepcidin synthesis from the diseased liver led to unregulated increased intestinal iron absorption with excess free iron further causing cellular death. This is a vicious cycle aggravating the disease process in the above mentioned patient.
Secondary Iron overload in chronic liver diseases is not uncommon. It is seen due to reduced hepcidin synthesis leading to increased intestinal iron absorption. The transferrin saturation of the patient was 98.3% with markedly elevated serum ferritin levels. Ferritin is an acute phase reactant and is elevated in inflammatory conditions but is not seen with raised transferrin saturation above 55% [10]. Serum transferrin saturation levels above 55% is highly suggestive for the diagnosis of hereditary hemochromatosis after secondary causes are ruled out [10].
The patient had high transferrin saturation (>98.3%) with high serum ferritin levels (>2000 mcg/dl). In hereditary hemochromatosis, hepcidin levels are low and hence consecutively excessive iron release from the enterocytes and macrophages [11]. For this reason, transferrin saturation is high (>55%) with non-transferrin bound iron related to toxicity to liver and other organs [5]. In our patient, the iron overload could be due to low hepcidin levels and the release of serum iron from macrophages to extracellular fluid with decrease in transferrin synthesis and iron accumulation within the hepatocytes, sinusoids, Kupffer cells and the biliary epithelial cells. The liver biopsy showed iron deposition within hepatocytes in peri-portal and mid-zonal zones. There was Intrahepatic, sinusoidal, Kupffer cells, biliary epithelial cell and portal macrophage iron deposition highlighted on Perl’s Prussian blue stain suggestive of severe iron overload. The biopsy was suggestive of chronic hepatitis with advanced fibrosis (Fibrosis F-4, METAVIR staging), Hepatic and sinusoidal hemosiderosis {Iron stage 3 to 4 (Scheuer’s grading), intrahepatic, canalicular and ductular cholestasis with interface hepatitis, plasma cell infiltration and rosette formation, compatible with autoimmune hepatitis and mixed pattern of iron overload seen in advanced cases.
Hepatocytes and Kupffer cells store iron in the form of ferritin, heme, and lysosomal hemosiderin, the latter being the predominant form of stainable iron [12]. On routine hematoxylin and eosin staining, hemosiderin deposits as golden brown refractile granules. The most commonly used method, the Perls’ Prussian blue stain, highlights hemosiderin granules in blue.
Two main patterns of iron accumulation have been described: parenchymal iron overload and Kupffer cell hemosiderosis. Parenchymal iron accumulation is the pattern seen in inherited forms of iron overload (also known as primary iron overload) and is characterized by iron accumulation in hepatocytes and bile duct epithelium. In hepatocytes, hemosiderin initially accumulates in a peri-canalicular distribution. In the lobules, hepatocellular iron build up is zonal and first affects periportal (zone 1) hepatocytes, extending toward zones 2 and 3 as iron overload progresses. The grading system described by Scheuer, for instance, scores hepatocellular iron on a scale of 1 to 4, ranging from minimal iron accumulation (grade 1) to diffuse accumulation that involves the entire lobule [13]. This pattern of iron accumulation is characteristic of HH.
Kupffer cell hemosiderosis, or secondary iron overload pattern, refers to hemosiderin accumulation in Kupffer cells, and sometimes portal macrophages and endothelial cells. It can also be seen after hepatocellular injury (e.g., acute hepatitis) because of the increased turnover of injured hepatocytes leading to transient Kupffer cell hemosiderosis. This pattern is also described in HH type 4 (FPN disease) [14]. The liver biopsy in the patient showed parenchymal (hepatocytes and biliary epithelial cells) iron deposition with hemosiderin laden macrophages and sinusoidal hemosiderin deposition, Iron stage 3 to 4 (Scheuer’s grading), with Kupffer cell hemosisderosis consistent with severe iron overload.
The patient was started on oral steroids. Azathioprine was started one month after initiation of steroid therapy. His liver function test normalized after 2 months of initiation of oral steroid. The patient’s ascites responded to diuretic therapy and is off diuretics at the time of reporting of the case.
The genetic analyses of C282Y/H63D was negative in the patient for HH, as C282Y mutation is almost non-existent in India [8]. In the study by A Koshy et al two out of three cases were due to hemojevulin mutation. We could not perform any further genetic analyses for the patient due to financial constraints.
Positive auto-antibodies with markedly elevated transferrin saturation and serum ferritin levels pose diagnostic dilemma which necessitated liver biopsy in the case to make a correct diagnosis. To our knowledge there have been only two case reports described previously with autoimmune hepatitis and secondary iron overload. This is unusual case report of chronic liver disease with autoimmune hepatitis with secondary mixed pattern of iron overload.
Consent
Informed consent is taken for publication.
Conflicts of Interest
None
References
-
Mack CL, Adams D, Assis DN, Kerkar N, Manns MP, et al. (2020) Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines from the American Association for the Study of Liver Diseases. Hepatology 72(2): 671-722.
-
An IC, Tiwari AK, Ameda S, Laird-Fick HS (2013) Autoimmune Hepatitis: Diagnostic Dilemma in the Setting of Suspected Iron Overload. Case Reports in Gastrointestinal Medicine.
-
Krawitt EL (2006) Autoimmune hepatitis. N Engl J Med 354(1): 54-66.
-
Bell H, Skinningsrud A, Raknerud N, Try K (1994) Serum ferritin and transferrin saturation in patients with chronic alcoholic and non-alcoholic liver diseases. Journal of Internal Medicine 236(3): 315-322.
-
Camaschella C, Poggiali E (2009) Towards explaining “unexplained hyperferritinemia”. Haematologica 94(3): 307-309.
-
Amarapurkar D, Dharod M, Amarapurkar A (2015) Autoimmune hepatitis in India: single tertiary referral centre experience. Tropical Gastroenterology 36(1): 36- 45.
-
Czaja AJ, Freese DK (2002) American Association for the Study of Liver Disease. Diagnosis and treatment of autoimmune hepatitis. Hepatology 36(2): 479-497.
-
Koshy A, Mukkada RJ, Chettupuzha AP, Francis JV, Kandathil JC, et al. (2020) Hemochromatosis in India: First Report of Whole Exome Sequencing With Review of the Literature. Journal of Clinical and Experimental Hepatology 10(2): 163-169.
-
Zhu L, Chen D, Zhu Y, Pan T, Xia D, et al. (2021) GPX- 4 regulated ferroptosis mediates S100 induced experimental autoiimune hepatitis associated with Nrf-2/HO-1 signaling pathway. Oxidative medicine and cellular longevity 2021: 6551069.
-
Piperno A (1998) Classification and diagnosis of iron overload. Haematologica 83(5): 447-455.
-
Camaschella C (2005) Understanding iron homeostasis through genetic analysis of hemochromatosis and related disorders. Blood 106(12): 3710-3717.
-
Turlin B, Deugnier Y (1998) Evaluation and interpretation of iron in the liver. Semin Diagn Pathol 15(4): 237-245.
-
Scheuer PJ, Williams R, Muir AR (1962) Hepatic pathology in relatives of patients with haemochromatosis. J Pathol Bacteriol 84: 53-64.
-
Salamao MA (2021) Pathology of Hepatic iron overload. Clinical Liver disease 17(4): 232-237.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient