Management of Paragangliomas in Neck - A Case Report
Carotid body tumors are rare neoplasm arising from the chemoreceptive tissue of the carotid body, which typically presents as a slow growing, painless neck mass found along the anterior border of the sternocleidomastoid muscle. They are also known as intercarotid paragangliomas; these tumors are benign in general but have a aggressive local growth potential. Therefore, complete surgical resection is the preferred treatment of choice.
Introduction
The carotid body is a neural crest cell-derived chemoreceptor located in the medial portion of the carotid bifurcation. When tumors develop from these cells, they are referred to as extra-adrenal neuroendocrine neoplasm’s [1]. Carotid body tumors are distinctly uncommon highly vascular neck tumors [2]. They are also known as intercarotid paragangliomas, which are derived from neural crest paraganglion cells and are most commonly found at the carotid bifurcation. Carotid body tumor also constitutes majority of head and neck paragangliomas (60-70%) [3]. The term paraganglia was first used by Kohn in the early twentieth century and is the most appropriate nomenclature from the embryological standpoint [3].
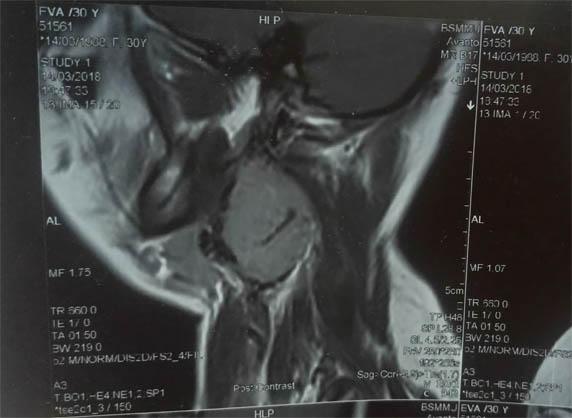
A 30 year old non-diabetic, normotensive, female patient was admitted in Bangabandhu sheikh mujib medical university, DHAKA, BANGLADESH in may 2018 with the complaints of swelling on left side of the neck, which had progressively been increasing in size over the past 2 years. She had two bouts of fainting attacks in last 1 year. On examination, there was a 3cm × 2cm pulsatile mass in the upper third of the sternocleidomastoid muscle, which was mobile side to side but not vertically, having smooth surface, no fixity to the muscle or either skin. There was no cranial nerve involvement. There was no lymphadenopathy and contralateral neck examination was normal. Patient was HBsAg positive but HBV DNA found to be negative. On magnetic resonance imaging (MRI) of the neck, an enhancing mass lesion was evident at the left carotid artery bifurcation, splaying internal and external carotid branches. Based on presentation and imaging, diagnosis of a carotid body tumor (shambling class ӀӀ) was made. Duplex ultrasound was done and characteristic splaying of the internal and external carotid artery with the mass of the carotid body tumor were found.
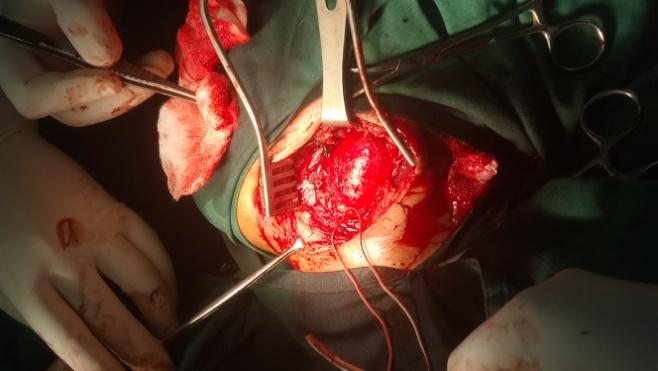
It was decided to operate the patient. Initially the tumor tissue was identified after a longitudinal incision along the anterior border of sternocleidomastoid muscle. When the tumor exposed, it was decided to take control of left common carotid artery. Further dissection was carried out during this process multiple feedings arteries mostly from left external carotid artery and internal carotid artery. These feedings arteries were ligated. Proper care was also taken to avoid any injury to adjoining structures i.e., nerve, vessels etc. Finally after meticulous dissection and preventive measures were taken to avoid injury to vessels and nerves, the carotid body tumor was taken out after ligating the stalk of tumor. Wound was closed in layers. The patient was discharged uneventfully without any complications.
Discussion
In 1743, Von Haller first described the carotid body [4]. The carotid body is small, vascular, tan-brown, oval structure, located within adventitia posteromedial to bifurcation of the common carotid artery. The healthy gland measures 3-5 mm in diameter and weight less than 15mg on average [4]. The gland is highly vascular and is attached by a thin strand of adventitia known as Meyers ligament which also carries its blood supply from feeder vessels, primarily from the external carotid artery, typically the ascending pharyngeal artery. The carotid body acts as a chemoreceptor, this receptor detect change in oxygen, carbondioxide and pH concentration and are involved in neurogenic physiologic adaptation to changes in these parameters [1]. Henceforth they alternatively named chemodectomas [2].
Carotid body tumors are usually asymptomatic and discovered to be a painless mass or fullness in the neck at the level of the carotid bifurcation [1]. A recent review of carotid body tumors identified diagnosis at a mean age of 55 years (range 14-94 years) and a male to female ratio of 1:1.9. More tumors (57%) were on the right side, whereas 25% were on left, 17% were bilateral, only 1 tumor was functional and 4.3% were malignant [1]. Some studies further emphasized the higher prevalence of women affected by these tumors [1]. As in our case we found it in the left side. This patients age and gender is on favour of diagnosis. Carotid body tumors are classified into sporadic, familial, and hyperplastic forms. Among these sporadic form is the most common type, representing approximately 85%. The familial type (10-50%) is more common in younger patients. The hyperplastic form is very common in patients with chronic hypoxemia, which include living in high altitudes (>5000 feet above sea level-like in Peru, Mexico etc), smoking, chronic obstructive pulmonary disease or other respiratory conditions that result in hypoxia [1]. Malignancy occurs in 6-12.5% of cases, which ranks carotid body paraganglioma as the most frequently occurring malignant head and neck paraganglioma [3]. Malignancy in CBTs is not determined on a histological background as the cellular appearance is relatively uniform and most of the tumor has microscopic evidence of capsular invasion. As such, malignancy can only be diagnosed according to clinical behaviour of the tumor: local invasion, recurrence, or evidence of metastasis [1]. Because of its location in close approximation to carotid vessels and X- X11 cranial nerves, tumors enlargement causes progressive symptoms such as dysphagia, odynophasia, hoarseness of voice or other cranial nerve deficits but in general condition CBTs are typically painless, slow growing tumors that are often present for years prior to the patient seeking medical attention which explain the large sizes found in literature some have reported tumors as large as 10cm3. There is no report of spontaneous regression. Fever is an uncommon sign of carotid body tumor, although the literature has reported it as one of the causes of fever of unknown origin [4]. The patient may give a history suggestive of symptoms associated with catecholamine production such as fluctuating hypertension, blushing, obstructive sleep apnea and palpitations. The differential diagnosis includes lymphadenopathies, bronchial cleft cysts, salivary gland tumors, neurogenic tumors, aneurysms of the carotid artery as well as HNPs [3]. Neuroendocrine tumors such as medullary thyroid carcinoma and neuroendocrine carcinoma are some other differential diagnosis. Size of the tumor bears a great importance not only for the clinical presentation, but also for taking decision on treatment. Shamblin, et al. introduce a classification (in 1971) scheme based on the tumor size, which reflects the degree of technical challenge in tumor excision. Small tumors could easily be resected from the vessel as Group 1. Group 2 includes tumors that are intimately associated with and also compress the carotid vessels, but can be resected with careful sub adventitial dissection. Group 3 consists of tumors that are large and typically encase the carotid artery, requiring complete or partial vessel resection and replacement [2]. CBTs are usually identified by clinical examination or found incidentally on imaging studies [1]. Ultrasound studies in both sides of the neck, may exclude the presence of lymph nodes, thyroid or branchial cysts. In majority of the cases Duplex ultrasound evaluates the hypervascularity and upward intratumoral blood flow in a neck mass at carotid angle, suggesting a CBT. Accurate diagnosis is based on angiographic criteria, the most reliable of these being the separation and splaying of external and internal carotid arteries. Axial imaging either CT angiography or MRI is the preffered modality for surgical planning of tumor resection because it best defines the relation of the tumor with the artery bifurcation and possible location of the cranial nerves [1]. For diagnosis, needle biopsy is unnecessary and complications may arise as often these hyper vascular masses will develop bleeding that is sometimes difficult to control. Because CBTs can be bilateral and paragangliomas can be multicentric, especially in familial cases, an octreotide scan is recommended for all patients once the diagnosis of a CBT has been made [1]. For Paragangliomas having less than 1cm size PET scan is recommended by some of the authors, but it may be less specific. Historically, preoperative angiography was the gold standard diagnostic procedure for carotid body tumors and was considered mandatory, both to confirm the diagnosis and to provide accurate preoperative delineation of the vascular supply [1]. The treatment of choice for most carotid body paragangliomas is surgical excision with careful subadnentitial dissection, concerning bleeding, clamping of all carotid arteries is useful, and with placement of internal carotid shunt. Some other articles recommend angiographic embolization preoperatively; these can be performed using ethanol or polyvinyl alcohol. Complete devascularization is the final result. With complete surgical resection overall prognosis is quite good. Regular follow up is necessary, however as recurrence and metastasis may occur after many years later [3]. Radiotherapy is helpful for nonsurgical candidates, as an adjacent for partially excised tumor or for patients with metastatic disease. Articles suggest that chemotherapy has no role in this tumor.
Conclusion
The carotid body tumor is a rare vascular tumor of the neck which must be diagnosed by imaging and not by biopsy. Surgical excision is planned after having a good road map using angiography or MRI. More the preoperative functional assessment the lesser will be the post operative complications. Meticulous and step by step dissection is very much helpful for successful removal of paragangliomas and has had good prognosis.
References
-
Muraglia GML, Patel VI Carotid artery: Carotid body tumor and other disorders. Rutherford’s Vascular Surgery 8th (Edn.), Elsevier Saunders, Philadelphia, Chapter 104, pp: 1598-1614.
-
Hoque R, Sharmeen HS, Md Abdul QC, Md Alauddin, Swadesh RS, et al. (2012) Carotid body tumor- A case report. University Heart Journal 8(1): 58-61.
-
Lezrag M, Aboulfadl M, Baghdadi T, Abada R, Rouadi S, et al. (2016) Carotid Body Tumor- Case Report and Review of The Literature. Journal of Case Reports and Studies 4(4): 2348-9820.
-
Luther A, Mahajan A (2014) Carotid Body Tumor - A Rare Case Report. JIMSA 27(40): 205.