Tardive Dyskinesia: Addressing the Challenges of an Iatrogenic Movement Disorder
Tardive dyskinesia (TD) is a potentially irreversible and disabling iatrogenic movement disorder characterized by involuntary, repetitive movements, predominantly affecting the orofacial region, trunk, and limbs. This severe adverse effect is associated with prolonged exposure to dopamine receptor blocking agents, particularly antipsychotic medications used in the treatment of psychiatric conditions such as schizophrenia and bipolar disorder. The pathophysiology of TD involves complex interactions between dopaminergic dysregulation, oxidative stress, neuroinflammation, and neuronal degeneration. Genetic factors, including variations in dopamine receptor genes, antioxidant pathways, and neuronal plasticity-related genes, contribute to individual susceptibility and symptom severity. While preventive measures, such as judicious use of antipsychotics and regular monitoring, remain the most effective strategies, once TD develops, management becomes challenging. Current pharmacological interventions, including vesicular monoamine transporter 2 (VMAT2) inhibitors, antioxidants, and alternative antipsychotics, provide symptomatic relief but do not consistently reverse the underlying pathology. Non-pharmacological approaches, such as deep brain stimulation, botulinum toxin injections, and rehabilitative therapies, can complement pharmacological interventions and improve functional outcomes and quality of life. Ongoing research efforts aim to elucidate the complex molecular mechanisms underlying TD and develop more targeted and personalized therapeutic strategies.
Introduction
Tardive dyskinesia (TD) is a potentially irreversible and disabling movement disorder characterized by involuntary, repetitive, and abnormal movements, predominantly affecting the oro facial region, trunk, and limbs. This condition is a severe adverse effect associated with prolonged exposure to dopamine receptor blocking agents, particularly antipsychotic medications used in the treatment of schizophrenia, bipolar disorder, and other psychiatric conditions. The prevalence of TD is a significant concern, with estimates suggesting that up to 20-30% of patients receiving long-term antipsychotic treatment may develop this disorder [1]. The risk increases with longer duration of antipsychotic exposure, higher dosages, and advanced age [2]. While both typical (first-generation) and atypical (second-generation) antipsychotics can induce TD, the risk is generally higher with typical antipsychotics, such as haloperidol and fluphenazine, due to their higher affinity for the dopamine D2 receptor [3]. The pathophysiology of TD is complex and multifactorial, involving dopaminergic dysregulation, oxidative stress, and neuronal degeneration.
The super sensitivity of dopamine receptors, particularly the D2 receptor subtype, is a central mechanism proposed to underlie TD development [4]. Chronic blockade of these receptors by antipsychotics leads to compensatory up regulation and hypersensitivity, resulting in involuntary movements upon withdrawal or continued treatment. Additionally, oxidative stress and neurotoxicity play crucial roles in the pathogenesis of TD. Antipsychotics have been shown to induce oxidative damage and mitochondrial dysfunction, leading to neuronal injury and degeneration [5]. Genetic factors, such as variants in the dopamine receptor genes (DRD2, DRD3), antioxidant enzyme genes (e.g., superoxide dismutase, glutathione peroxidase), and other susceptibility genes, may also contribute to individual variability in TD risk [6]. The pathogenesis of TD involves complex relationship between dopaminergic dysregulation, oxidative stress, neuroinflammation, and neuronal degeneration. While the precise mechanisms remain an area of active investigation, several key processes have been implicated in the development of this iatrogenic movement disorder. The dopamine supersensitivity hypothesis is a central theory proposed to explain the pathogenesis of TD.
Chronic exposure to dopamine receptor blocking agents, particularly the first-generation or typical antipsychotics like haloperidol, fluphenazine, and chlorpromazine, leads to compensatory up regulation and supersensitivity of dopamine receptors, predominantly the D2 subtype [7]. This supersensitivity results in dysregulated dopaminergic neurotransmission in the nigrostriatal and mesolimbic pathways, which manifests as involuntary movements upon continued antipsychotic treatment or withdrawal. Mounting evidence from preclinical and clinical studies suggests that oxidative stress and neuronal degeneration play crucial roles in the development of TD. Antipsychotics, both typical and atypical agents like risperidone and olanzapine, have been shown to induce oxidative damage by promoting the formation of reactive oxygen species (ROS) and impairing antioxidant defense mechanisms. This oxidative stress can lead to mitochondrial dysfunction, neuroinflammation, and neuronal injury, particularly in the basal ganglia and other brain regions involved in movement control [8] (Figure 1) schematically represents the pathophysiology of drug induced TD.
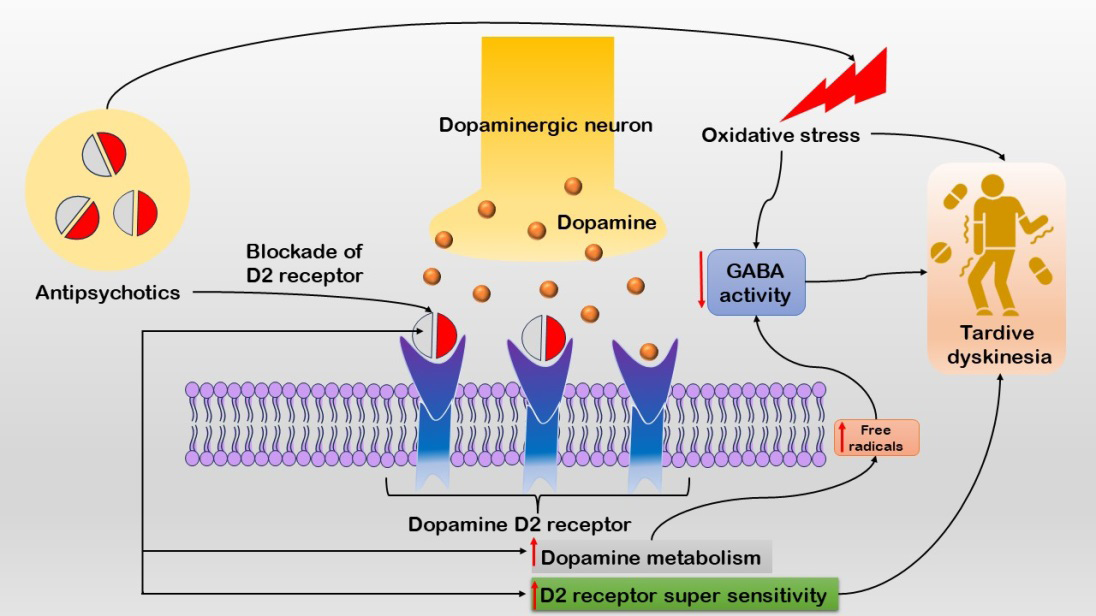
Figure 1: The figure illustrates the mechanisms underlying TD. Chronic exposure to dopamine receptor blocking agents, especially first-generation antipsychotics, leads to dopamine receptor up regulation and supersensitivity, resulting in dysregulated neurotransmission in the nigrostriatal and mesolimbic pathways. Additionally, antipsychotics induce oxidative stress by promoting reactive oxygen species (ROS) formation and impairing antioxidant defenses, leading to reduced GABA activity.
Several well-established and emerging risk factors contribute to an increased susceptibility to developing TD. Both typical (first-generation) and atypical (second- generation) antipsychotics can induce TD, with the risk generally being higher for typical agents like haloperidol, fluphenazine, and chlorpromazine due to their stronger affinity for the D2 receptor and higher propensity for causing extrapyramidal side effects [9]. However, atypical antipsychotics are not entirely risk-free, with agents like risperidone and paliperidone exhibiting a higher TD risk compared to others like clozapine and quetiapine [10]. The risk of TD increases with prolonged exposure to antipsychotics, with estimates suggesting a 5% risk after one year of treatment and up to 30% risk after five years or more. This risk appears to be dose-dependent, with higher cumulative doses of antipsychotics associated with a greater likelihood of developing TD [11]. Advanced age and female sex have been consistently associated with a higher risk of developing TD, potentially due to age- related changes in dopamine receptor sensitivity, hormonal factors, and increased susceptibility to oxidative stress [12]. Genetic variations in several genes have been implicated in TD susceptibility, including dopamine receptor genes (DRD2, DRD3), antioxidant enzyme genes (e.g., superoxide dismutase, catalase, glutathione peroxidase), and genes involved in neuronal plasticity and degeneration (e.g., brain- derived neurotrophic factor, α-synuclein) [13]. However, the specific contributions of these genetic factors and their interactions with environmental and clinical risk factors remain an area of active research.
Tardive dyskinesia is characterized by a diverse range of involuntary, repetitive, and abnormal movements, primarily affecting the orofacial region, trunk, and limbs. The clinical manifestations and diagnostic approach for TD are as follows:
Symptoms and Presentations
Orofacial Dyskinesia
The most common presentation of TD involves involuntary movements of the orofacial region, including lip smacking, tongue protrusion, chewing or sucking movements, and grimacing [14]. These movements can be disfiguring and can interfere with speech, swallowing, and social interactions.
Limb and Truncal Dyskinesia
In addition to orofacial dyskinesia, TD can also manifest as involuntary movements of the limbs and trunk, such as chorea (irregular, unpredictable movements), athetosis (slow, writhing movements), and dystonia (sustained muscle contractions) [15]. These movements can affect the upper and lower extremities, as well as the trunk, and can impair activities of daily living and mobility.
Other Associated Symptoms
In some cases, TD may be accompanied by additional symptoms, such as respiratory dyskinesia (irregular breathing patterns), blepharospasm (involuntary eye blinking or closure), and vocalizations or grunting sounds [16].
Diagnostic Criteria and Evaluation
The diagnosis of TD is primarily based on clinical presentation and a thorough medical history, including the duration and type of antipsychotic exposure. The Abnormal Involuntary Movement Scale (AIMS) and the Dyskinesia Identification System: Condensed User Scale (DISCUS) is widely used standardized rating scales for assessing the presence and severity of TD [17].
Differential Diagnosis
TD must be distinguished from other movement disorders, such as Parkinson’s disease, Huntington’s disease, and other drug-induced movement disorders (e.g., akathisia, parkinsonism). Neuroimaging techniques, such as magnetic resonance imaging (MRI) and positron emission tomography (PET), can aid in the differential diagnosis by evaluating structural and functional brain abnormalities associated with specific movement disorders [18].
The management of TD presents significant challenges due to its complex pathophysiology and the potential irreversibility of the condition. Current strategies involve a multifaceted approach, encompassing preventive measures, pharmacological interventions, and non-pharmacological therapies. Ongoing research efforts aim to develop more effective and targeted treatments. Once TD has developed, pharmacological interventions aim to alleviate symptoms and potentially reverse the underlying pathophysiology. In some cases, discontinuation or reduction of the antipsychotic medication responsible for inducing TD may lead to symptom improvement or remission. However, this approach is often challenging due to the risk of psychiatric relapse [19]. Switching to an atypical antipsychotic with a lower propensity for causing TD, such as clozapine or quetiapine, may be beneficial in some cases [20]. However, the risk of TD is not entirely eliminated with atypical agents. Several pharmacological agents have been investigated for the symptomatic management of TD, with varying degrees of efficacy and tolerability:
• Vesicular monoamine transporter 2 (VMAT2) inhibitors, such as valbenazine and deutetrabenazine, have shown promising results in reducing TD severity [21].
- Antioxidants, such as vitamin E and melatonin, may exert neuroprotective effects and alleviate TD symptoms by reducing oxidative stress [22].
- Other agents, including clonazepam, amantadine, and levetiracetam, have been explored with mixed results [23].
In addition to pharmacological interventions, non- pharmacological approaches can provide symptomatic relief and improve functional outcomes. Deep brain stimulation (DBS), involving the surgical implantation of electrodes in specific brain regions (e.g., globus pallidus interna), has shown promising results in reducing TD severity in some patients [24]. However, this invasive approach is typically reserved for severe, refractory cases. Injections of botulinum toxin into affected muscles can alleviate focal dyskinesias, particularly in the orofacial region [25]. Though, this approach is limited to specific muscle groups and requires repeated injections. Rehabilitative therapies, such as speech therapy, swallowing exercises, and occupational therapy, can help manage functional impairments associated with TD and improve quality of life [26].
Conclusion and Future Prospective
TD is a severe and potentially irreversible movement disorder associated with prolonged exposure to dopamine receptor blocking agents, particularly antipsychotic medications. This condition poses a significant burden on patients, caregivers, and healthcare systems, underscoring the importance of addressing its prevention, early detection, and effective management. The pathophysiology of TD involves complex interactions between dopaminergic dysregulation, oxidative stress, neuroinflammation, and neuronal degeneration. Genetic factors, including variations in dopamine receptor genes, antioxidant pathways, and neuronal plasticity-related genes, contribute to individual susceptibility and symptom severity. While preventive measures, such as judicious use of antipsychotics, regular monitoring, and minimizing risk factors, remain the most effective strategies, once TD develops, management becomes challenging. Current pharmacological interventions, including vesicular monoamine transporter 2 (VMAT2) inhibitors, antioxidants, and alternative antipsychotics, provide symptomatic relief but do not consistently reverse the underlying pathology. Non-pharmacological approaches, such as deep brain stimulation, botulinum toxin injections, and rehabilitative therapies, can complement pharmacological interventions and improve functional outcomes and quality of life for patients with TD. Ongoing research efforts are focused on elucidating the complex molecular mechanisms underlying TD, with the aim of developing more targeted and personalized therapeutic strategies. Advancements in genetic and biomarker studies, novel pharmacological agents, and emerging technologies like gene therapy and regenerative medicine hold promise for improving the prevention and treatment of this debilitating condition.
Conflict of Interest
Authors declare no conflict of interest.
References
-
Vasan S, Padhy RK (2023) Tardive Dyskinesia. StatPearls.
-
Cornett EM, Novitch M, Kaye AD, Kata V, Kaye AM (2017) Medication-Induced Tardive Dyskinesia: A Review and Update. Ochsner J 17(2): 162-174.
-
Chokhawala K, Stevens L (2023) Antipsychotic Medications. StatPearls.
-
Takeuchi H, Mori Y, Tsutsumi Y (2022) Pathophysiology, prognosis and treatment of tardive dyskinesia. Ther Adv Psychopharmacol 12:20451253221117313.
-
Caroff SN (2020) Recent Advances in the Pharmacology of Tardive Dyskinesia. Clin Psychopharmacol Neurosci 18(14): 493-506.
-
Zai CC, Maes MS, Tiwari AK, Zai GC, Remington G, et al. (2018) Genetics of tardive dyskinesia: Promising leads and ways forward. J Neurol Sci 389: 28-34.
-
Adams JD (2019) Tardive Dyskinesia and Dopamine Oxidation, Cumulative Effects. J 2(2): 138-141.
-
Uludag K, Wang DM, Zhang XY (2022) Tardive Dyskinesia Development, Superoxide Dismutase Levels, and Relevant Genetic Polymorphisms. Oxid med cell longev 2022: 5748924.
-
Carbon M, Kane JM, Leucht S, Correll CU (2018) Tardive dyskinesia risk with first- and second-generation antipsychotics in comparative randomized controlled trials: a meta-analysis. World Psychiatry 17(3): 330-340.
-
Grinchii D, Dremencov E (2020) Mechanism of Action of Atypical Antipsychotic Drugs in Mood Disorders. Int J Mol Sci 21(24): 9532.
-
Cloud LJ, Zutshi D, Factor SA (2014) Tardive dyskinesia: therapeutic options for an increasingly common disorder. Neurotherapeutics 11: 166-176.
-
Wu Q, Yuan F, Zhang S, Liu W, Miao Q, et al. (2022) Correlation of Blood Biochemical Markers with Tardive Dyskinesia in Schizophrenic Patients. Dis Markers 2022: 1767989.
-
Tsermpini EE, Redenšek S, Dolžan V (2021) Genetic Factors Associated With Tardive Dyskinesia: From Pre- clinical Models to Clinical Studies. Front Pharmacol 12: 834129.
-
Anusa AM, Thavarajah R, Nayak D, Joshua E, Rao UK, et al. (2018) A Study on Drug-Induced Tardive Dyskinesia: Orofacial Musculature Involvement and Patient’s Awareness. J Orofac Sci 10(2): 86-95.
-
Hauser RA, Meyer JM, Factor SA, Comella CL, Tanner CM, et al. (2022) Differentiating tardive dyskinesia: a video-based review of antipsychotic-induced movement disorders in clinical practice. CNS Spectr 27(2): 208-217.
-
Kiliç A, Erten E, Özdemir A (2015) Tardive Blepharospasm and Meige Syndrome during Treatment with Quetiapine and Olanzapine. Noro Psikiyatr Ars 52(2): 207-209.
-
Jackson R, Brams MN, Citrome L, Hoberg AR, Isaacson SH, et al. (2021) Assessment of the Impact of Tardive Dyskinesia in Clinical Practice: Consensus Panel Recommendations. Neuropsychiatr Dis Treat 17: 1589- 1597.
-
Ward KM, Citrome L (2018) Antipsychotic-Related Movement Disorders: Drug-Induced Parkinsonism vs. Tardive Dyskinesia-Key Differences in Pathophysiology and Clinical Management. Neurol Ther 7(2): 233-248.
-
Ricciardi L, Pringsheim T, Barnes TRE, Martino D, Gardner D, et al. (2019) Treatment Recommendations for Tardive Dyskinesia. Can J Psychiatry 64(6): 388-399.
-
Mathews M, Gratz S, Adetunji B, George V, Mathews M, et al. (2005) Antipsychotic-induced movement disorders: evaluation and treatment. Psychiatry (Edgmont) 2(3): 36-41.
-
Golsorkhi M, Koch J, Pedouim F, Frei K, Bondariyan N, et al. (2024) Comparative Analysis of Deutetrabenazine and Valbenazine as VMAT2 Inhibitors for Tardive Dyskinesia: A Systematic Review. Tremor Other Hyperkinet Mov (N Y) 14:13.
-
Filograna R, Beltramini M, Bubacco L, Bisaglia M (2016) Anti-Oxidants in Parkinson’s Disease Therapy: A Critical Point of View. Curr Neuropharmacol 14(3): 260-271.
-
Cloud LJ, Zutshi D, Factor SA (2014) Tardive dyskinesia: therapeutic options for an increasingly common disorder. Neurotherapeutics 11: 166-176.
-
Szczakowska A, Gabryelska A, Gawlik-Kotelnicka O, Strzelecki D (2023) Deep Brain Stimulation in the Treatment of Tardive Dyskinesia. J Clin Med 12(5): 1868.
-
Yoshida K (2022) Botulinum Toxin Therapy for Oromandibular Dystonia and Other Movement Disorders in the Stomatognathic System. Toxins (Basel) 14(4): 282.
-
Caroff SN (2019) Overcoming barriers to effective management of tardive dyskinesia. Neuropsychiatr Dis Treat 15: 785-794.
- Superposition of Cryo-EM and AlphaFold Predictions of Dengue Antigen-Antibody Complexes
- Jugular-Applied Coherent Low-Level Laser Therapy Enhances Systemic Mitochondrial Metabolic Function and Antioxidant Response
- Role of OMC32 Polypeptide in Acrosin-Mediated Exocytosis during the Bovine Sperm Acrosome Reaction
- Association of Galectin-3 but not Laminin in Tamoxifen-Induced Growth Suppression in Breast Cancer MCF-7 Cells
- Effect of Different Wavelengths of Light on the Rate of Photosynthesis
- Nutritional, Therapeutic, and Environmental Effect of Oyster Mushrooms: An Editorial