Cell Proliferation and Cell Death (Apoptosis) in Adjacent Sections of White and African Americans Analyzed in Relation to the Gleason Histological Scores, Immunohistochemical and Immunofluorescence
Introduction: Our objective was to determine whether prostate cancer (PC) grew similarly or differently in White Americans (WA) and African Americans (AA) and race-specific treatment will improve survival of each race as indicated by analysis of data in relation to Gleason histological scores. We hypothesize that cell proliferation and/or apoptosis can occur differentially in the two races. Differential diagnosis can be followed by hormonal, focused beam radiation and/or chemotherapy treatments. Since more AA men with PC than WA, we expect that Gleason l score-based diagnosis and treatments would improve survival of patients. Materials and Methods: We studied 55 WA and 20 AA prostectomy specimens for localization of cell proliferation and cell death markers by immunohistochemical and immunofluorescence techniques. Briefly, formalin fixed, and paraffin-embedded and/or frozen tissues were used in localization of markers. Localization of black and white and coloured images were obtained directly from slides to a Zeiss microscope equipped with a digital Nikon camera. Results: We found that cell proliferation increased in Gleason scores 5 and 7 of white patients and score 6 and 7 of African Americans. Our data indicates need for aggressive treatments in these scores. Our study is supported by three tables, statistics, graphs, histological, Immunohistochemical, and immunofluorescence figures. Discussion: This is the first study to suggest that PC grows differently in WA and AA and s race-specific diagnosis and treatment is expected to improve survival of PC patients using hormonal, radiation and/or chemotherapy treatments. The Author (AAS) had numerous discussions with Urologists, Pathologists, and scientists on the treatments of PC indicate. He has concluded that prostatectomy ought to be followed by focused beam radiation to prostatic fossa and adjacent areas to cure PC. Chemotherapy drugs circulate from head to toe in the body and often do not reach required concentration at cancer sites to kill malignant cells.
Abbreviations
PC: Prostate Cancer; WA: White Americans; AA: African Americans; IRB: Institutional Review Board; ADT: Androgen Deprivation Treatment; BPH: Benign Prostatic Hyperplasia; MIB: Cell Proliferation Antibody.
Introduction
PC does not discriminate between rich and poor and races, yet more AA die of the cancer than WA patients. There are many reasons for the differences, including early and late diagnosis, and treatments. PC is among the diagnosed malignancy in the world [1]. Benign (normal) prostate develops as tubules which drain in prostatic ducts and finally in the ejaculatory duct. Initially, human prostate tumor is of pea size and avascular [2]. Prostate tumor has length, width, and height and it does not grow until vascularized by blood vessels and capillaries [1]. Benign prostate contains numerous acinar glands, and stroma with blood vessels and lymphatics [3, 4]. Distribution of cancerous acini and stromal vascularity varies in cancer as shown by Gleason histological scores [4]. An acinar gland contains basal, stem, niche, and cuboidal/columnar (secretory) cells enclosing a lumen, whereas stroma contains connective tissue, blood vessels, lymphatics, fibroblasts, smooth muscles, collagen, nerves, and macrophages [3, 4, 5]. Homeostatic balance is maintained between cell proliferation and cell death in benign prostate and this balance is greatly altered in PC [6, 7]. Cell proliferation is often involved in the growth of PC, but cancer growth can occur by the decreased cell death [8, 9, 10, 11]. PC is often detected in men of 50 years or older, however it can be detected in younger men. The average age of patients with PC in the VA was 68.5 years.
Numerous studies on cell proliferation alone and cell death have been conducted on benign and PC [8, 9, 10, 11, 12]. Many separate studies on cell proliferation or cell death have not been conducted before but not in adjacent or serial sections and analyzed in relation to Gleason histological scores. Tumor growth usually occurs at the posterior portion of the gland, but it can grow on the underside as well. The relationship between cell proliferation and cell death is complex [8, 9, 10, 11, 12]. Complexity is further increased when PC is not studied in adjacent or serial sections. Complex tissue fixation and processing techniques require separate technique for parathion of samples [8, 9, 10, 11, 12, 13]. These have resulted in incomplete and/or poor understanding of cell proliferation and cell death in PC. We hypothesize that PC can grow by increased cell proliferation, decreased cell death and/or their combinations. Complexity of PC is shown in Gleason score patterns [4]. This complexity is expected to show differences in the two races and treatments using hormonal, cytotoxic and/or radiation. Support for our hypothesis comes from the unregulated progression of PC as shown by the Gleason grades/scores [4].
An acinar gland contains basal, stem, niche, and cuboidal/ columnar (secretory) cells [3, 14]. Cancer stem cells are often associated with the basal cells and possess unique properties of self-renewal [3]. The exact numbers of stem cells and their genes in human prostate are unknown. Stem cells have been partially characterized by surface markers, namely, CD44, CD133, integrin α2 [15, 16, 17], Pluripotency factors like OCT4, NANOG, and SOX2 are present in stem cells. Several signalling pathways are also over-activated in stem cells, including Notch, PTEN/Akt/PI3K, RAS-RAF-MEK-ERK and HH [14, 15, 16, 17]. Many genes have been implicated in PC, namely, BRCA1, BRCA2, ATM, PALB2, CHEK2, MLH1, MSH2, MSH6, and PMS2 [14]. PC stem cells are usually an obstacle in cancer therapy and are a major cause of drug resistance, recurrence, and metastasis [14, 15, 16, 17]. Available treatments, targeting proliferating cancer cells are not effective in eliminating quiescent cells. Stem cells proliferate in prostate and its cancer [3]. Basal, niche, cuboidal/columnar cells usually do not proliferate and its cancer [3]. Columnar and cuboidal cells proliferate in castrated mice treated with testosterone [18]. Organogenesis establishes organ-specific stem cells and their genes during fetal life (such as in prostate, lungs, colon, brain [3]. The exact numbers of stem cells and genes are unknown. They become organ specific during organogenesis and therefore, gene therapy is not expected to be successful [3, 14, 15, 16, 17].
Materials and Methods
The former and current urology surgeons, Drs. Pratap K. Reddy and Eduardo T. Fernandes and their associates selected patients for radical prostatectomy at the Minneapolis Veterans Affairs Medical Center (VAMC). Prostate specimens were submitted to the Surgical Pathology Service and the extra specimens were provided for the research. Patients had not been treated with any hormone or chemotherapy prior to the surgery. All samples were collected after obtaining the consent of the patients and approval of the institutional review board (IRB) according to the guidelines in place at the VA and the University of Minnesota. For this study, we collected prostatectomy samples of 55 White Americans, and 20 African American patients. Our study involved laboratory coordination with surgery, collection of tissues, and processing specimens for distinctly two different techniques. Localizations of cell proliferation and cell death markers were conducted on adjacent sections using appropriately processed specimens. Each localization technique required differential processing of tissues requiring separate techniques. Localization of cell proliferation was conducted using MIB 1 antibody (ABCAM, Cambridge U.K). Cell death required processing by Tunnel assay (Roche Diagnostic
Corporation, Indianapolis, IN, USA) [8, 9, 10, 11, 12]. Initially, we used fresh frozen, acetone or ethanol-fixed specimens which did not provide consistent results. Buffered formalin-fixed specimens required preparation of at least four adjacent sections. Briefly, sections were deparaffined in xylene and processed through graded ethanol to water for localization of cell proliferation antibodies using MIB1 antibody IgG (dilution 1 to 10) using immunohistochemical methods outlined by the company as reported before [3, 9, 10, 11, 13]. After localization, sections were processed prior to mounting using per mount.
We localized cell death using Tunnel localization techniques with protocols provided by Roche Diagnostic Corporation. We also used Apoptag techniques as detailed in the Manual (Invitrogen Company, Purchase, NY, USA). Briefly, formalin-fixed sections required antigen retrieval. Sections were treated with diluted acetic acid of pepsin before conducting localization of cell death marker. Localization was evaluated by light and fluorescence microscopy. Localization of polyclonal antibody IgG against actin (dilution 1: 30) (Dako Corp., Carpentaria, CA, USA) and the reaction product was developed using secondary antibody, as shown in the smooth muscles surrounding acini. Prostatic sections were graded using hematoxylin and eosin-stained sections by the former pathologists at the Minneapolis, Drs. Donald F. Gleason, and Stephen L. Ewing using Gleason histological scores [4, 19]. Prostectomy patients had clinical stages B, C and D [20] (Figures 1A & 1B).
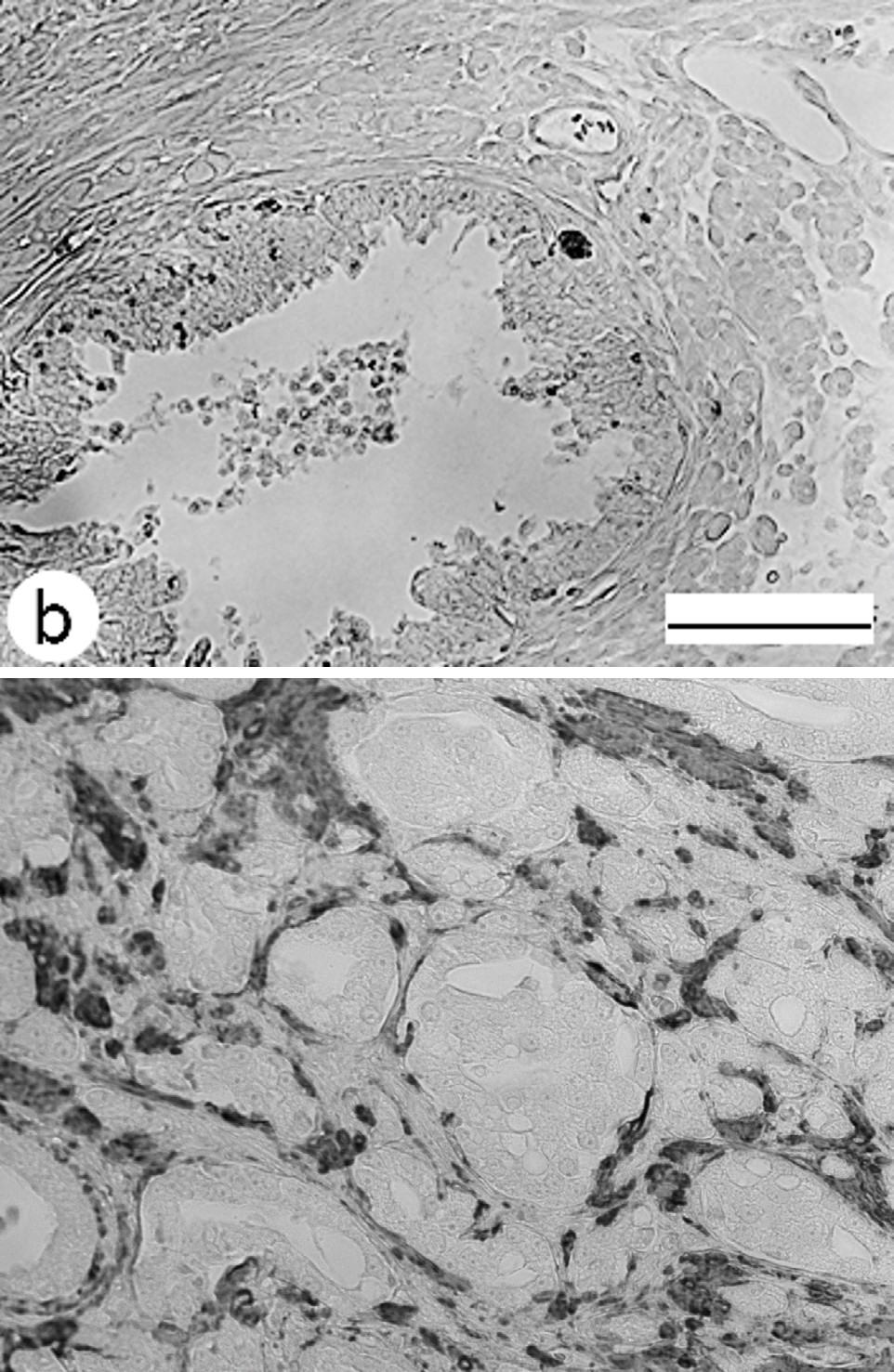
Figure 1(A): Prostate gland shows glandular cells, slooghed cells in the lumen, stroma vascularity and smoothe muscles.
Figure 1(B): Micrograph shows localization of antibody IgG against actin in smooth muscles of the stroma surrounding cancerous prostate glands in cross sections.
Cell proliferation and cell death fluorescence markers have been assessed before [3, 9, 10, 11, 12, 21, 22]. Briefly, fluorescence isothiocyanate (FITC) was obtained (Jackson Research, West Grove, PA) and rhodamine (Cy3) from Oncogene Research (Cambridge, MA). Cell proliferation was localized with antibody (dilution 1:300) and FITC fluorescein produced (green) fluorescence. Cell death was localized with antibody (1:500) as shown by rhodamine Cy3 (red) fluorescence. Sections showing yellow florescence showed colocalization of green and red markers together. Some prostate gland cells did not localize markers indicating that cells were either dormant or inactive (Figures 1C & 1D). Fluorescence techniques required antigen retrieval in formalin-fixed and paraffin-embedded sections. Briefly, sections were treated with xylene followed by graded ethanol to water and phosphate buffer saline (PBS). Paraffin fixed sections required antigen retrieval and were processed via xylene, graded ethanol to water, and PBS before incubation with diluted pepsin for 30 minutes at room temperature.
Sections were washed several times in water and PBS before incubating with the diluted primary antibodies at room temperature and washed with PBS before incubating with the secondary antibodies. Reaction products were developed using peroxidase techniques detailed before [3, 13, 21, 22, 23]. Control studies were incubated with the normal serum of the animals used in preparation of the antibody. Images were acquired directly from the slides to a Zeiss microscope equipped with a Nikon digital camera and/or epifluorescence microscope to a computer. Images were photographed for the study and were adjusted using Photoshop for the uniformity of brightness or darkness as needed. AA samples were not available for immunofluorescence study. The laboratory study was completed before the author retired and the writing was completed after retirement.
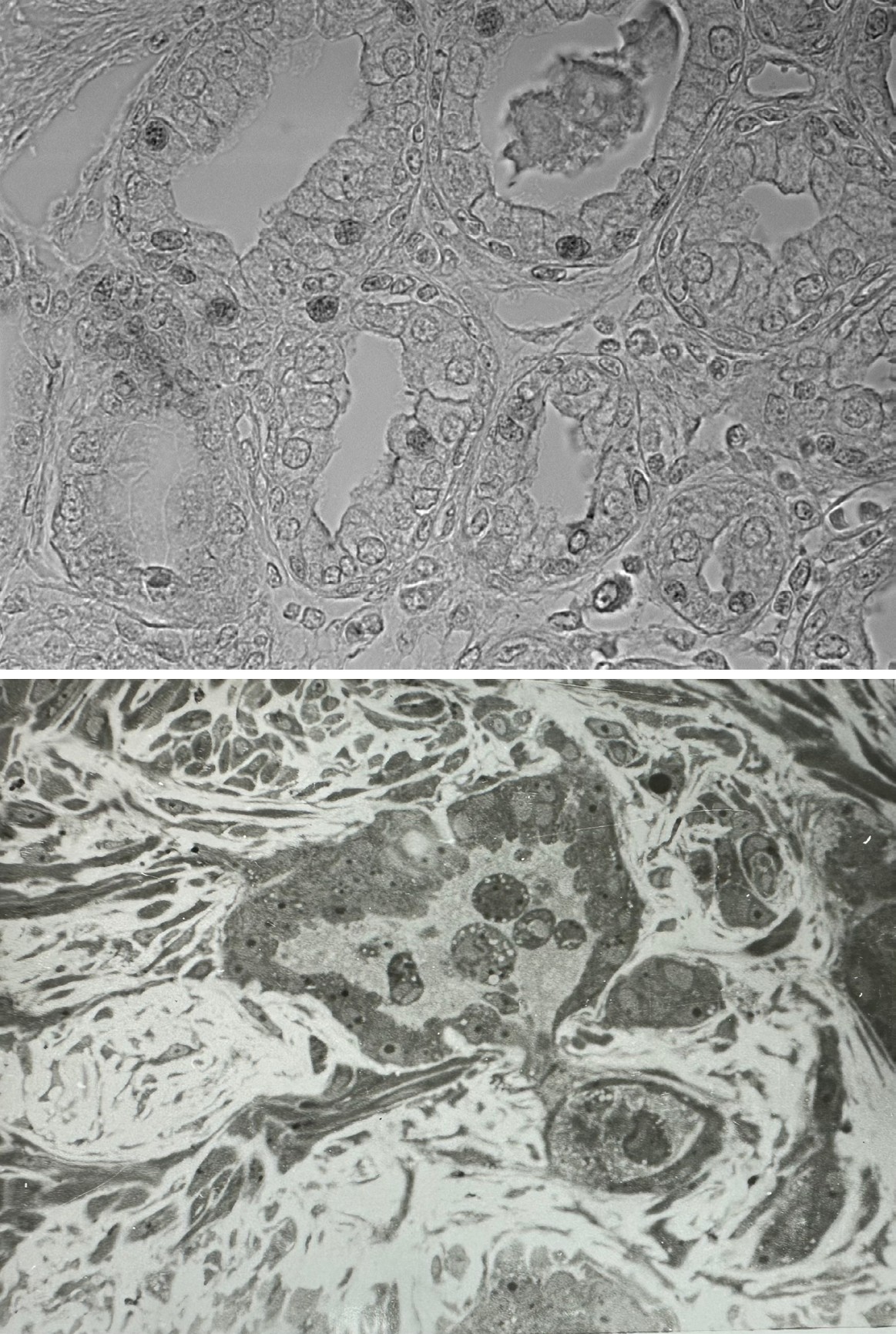
Figure 1(C): Canceous acini show a light cells (androgen-dependent) and dark cells (dark cells (androgen-independent) (see ref # 22). Some cancer cells are intrufing (nigrating) in stroma and forming flandular structure.
Figure 1(D): Cancerous cell is invading prosttic stroma and forming small glands. Lumen has many sloughed cells are present the lumen. Light and dark acinar cells are in the acinus. Gland is surrounded by smoothe muscles and vascular elements. Benign prostate in cross section illustrates normal cells and sloughed cells in the lumen. Stromal conectice tissue surrounds the gland.
Results
We have presented data of WA and AA in three tables and statistics along with graphs. Age of patients ranged from 53.36 to 76.30 years, average age 66.79 years. Earlier study had shown that patients localizing <9ng/ml of PSA respond to treatment and survived longer than those with PSA more than 9ng/ml [24]. Antibody against actin was localized in smooth muscles of prostatic stroma (Figures 2A & 2B). Cell proliferation was localized by MIB 1 IgG antibody l in benign prostate, BPH and PC (Figures 2C & 2D). Localization was conducted on paraffin sections and data was presented, including statistical analysis, and graph figures (Tables 1 & 2 with Statistics, with and Graph Figures 1 & 2).
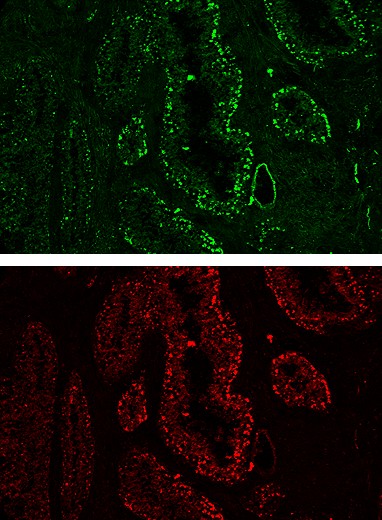
Figure 2(A): Immunofluorescence micrograph shows cell proliferation by green fluorescence of fluorescence isothiocyanate (FITC). Glands show lumina and stroma does not show Immunofluorescence.
Figure 2(B): Immunofluorescence micrograph shows cell death by rhodamine (red) fluorescence. Stroma does not show Immunofluorescence.
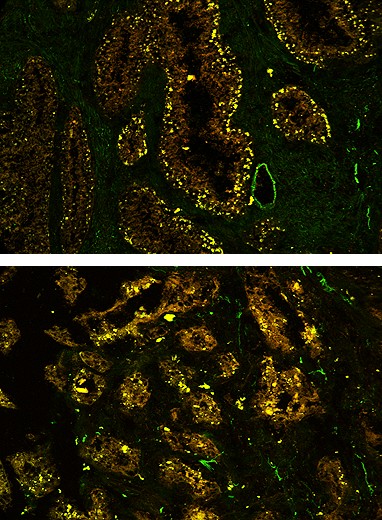
Figure 2(C): Yellow Fluorescence shows when cell proliferation and cell death localizations were combined. Micrograph also shows that many prostate cells did not localize indicating that they were either dormant or inactive. Stroma does not show Immunofluorescence.
Figure 2(D): Another area of the prostate shows yellow fluorescence when cell proliferation and cell death localizations were combined. The micrograph also shows that many prostate cells did not localize indicating that they were either dormant or inactive. Stroma does not show Immunofluorescence.
| Patient # | Gleason | MIB | CD |
|---|---|---|---|
| 346 | 5 | 0.156 | 0.819 |
| 523 | 5 | 0.126 | 0.234 |
| 421 | 5 | 0.142 | 0.202 |
| 427 | 5 | 0.068 | 0.088 |
| 454 | 4 | 0.209 | 0.125 |
| 469 | 5 | 0.081 | 0.044 |
| 473 | 5 | 0.041 | 0.004 |
| 479 | 5 | 0.116 | 0.038 |
| 504 | 5 | 0.198 | 0.104 |
| 373 | 5 | 0.156 | 0.059 |
| 477 | 5 | 0.244 | 0.08 |
| 423 | 5 | 0.342 | 0.163 |
| 403 | 5 | 0.29 | 0.096 |
| 415 | 6 | 0.259 | 0.021 |
| 393 | 6 | 0.355 | 0.072 |
| 526 | 6 | 0.491 | 0.148 |
| MIB | CD | |
|---|---|---|
| # of Cases | 16.000 | 16.000 |
| Total Value | 3.274 | 2.297 |
| Range | 0.041-0.491 | 0.004-0.819 |
| Mean | 0.205 | 0.144 |
| Std Deviation | 0.121 | 0.191 |
| Increases | 12 | 4 |
| Decreases | 4 | 12 |
| # of Cases | 39 | 39 |
| Total value | 9.21 | 17.466 |
| Range | 0.041 - 0.797 | 0.016 - 1.516 |
| Mean | 0.236 | 0.448 |
| Std Deviation | 0.17 | 0.482 |
| Increases | 21 | 18 |
| Decreases | 18 | 21 |
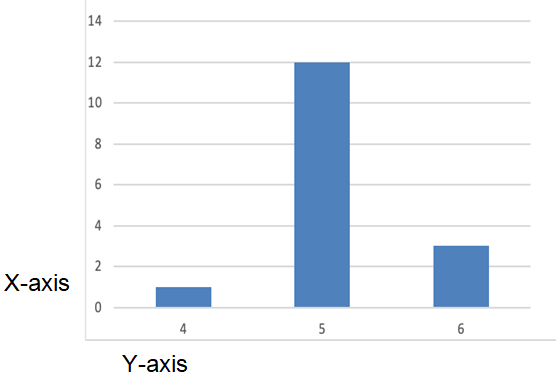
Table 1, Graph Figure 1 and Statistics: Prostate Cell Proliferation & Cell Death in White Americans Gleason scores 4-6, scores 7 and 9.
| Patient # | Gleason | MIB | CD |
|---|---|---|---|
| 419 | 7 | 0.072 | 0.069 |
| 425 | 7 | 0.123 | 0.099 |
| 360 | 7 | 0.048 | 0.023 |
| 445 | 7 | 0.144 | 0.116 |
| 510 | 7 | 0.049 | 0.016 |
| 465 | 7 | 0.105 | 0.066 |
| 7 | 0.074 | 0.034 | |
| 312 | 7 | 0.155 | 0.111 |
| 443 | 7 | 0.288 | 0.222 |
| 321 | 7 | 0.469 | 0.4 |
| 370 | 7 | 0.168 | 0.06 |
| 351 | 7 | 0.194 | 0.071 |
| 453 | 7 | 0.185 | 0.055 |
| 376 | 7 | 0.267 | 0.107 |
| 535 | 7 | 0.451 | 0.228 |
| 500 | 7 | 0.285 | 0.053 |
| 430 | 7 | 0.323 | 0.091 |
| 330 | 7 | 0.439 | 0.046 |
| 503 | 7 | 0.797 | 0.183 |
| 439 | 8 | 0.118 | 0.073 |
| 410 | 9 | 0.593 | 0.153 |
| 537 | 7 | 0.13 | 1.516 |
| 521 | 7 | 0.146 | 1.319 |
| 534 | 7 | 0.162 | 1.213 |
| 498 | 7 | 0.106 | 1.138 |
| 381 | 7 | 0.185 | 1.08 |
| 387 | 7 | 0.505 | 1.35 |
| 491 | 7 | 0.437 | 1.265 |
| 379 | 7 | 0.292 | 0.992 |
| 392 | 7 | 0.317 | 0.898 |
| 475 | 7 | 0.191 | 0.664 |
| 413 | 7 | 0.436 | 0.803 |
| 483 | 7 | 0.16 | 0.513 |
| 412 | 7 | 0.041 | 0.231 |
| 467 | 7 | 0.154 | 0.3 |
| 466 | 7 | 0.153 | 0.249 |
| 518 | 7 | 0.275 | 0.308 |
| 489 | 9 | 0.093 | 1.181 |
| 344 | 9 | 0.079 | 0.17 |
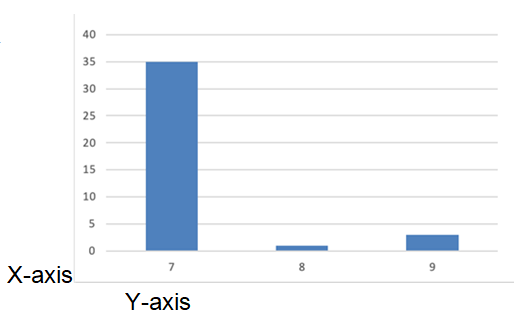
Table 2, Graph Figure 2 and Statistics: Prostate Cell Proliferation & Cell Death in White Americans Gleason 7-9.
| Patient # | Gleason | MIB | CD |
|---|---|---|---|
| 86-41 | 5 | 0.268 | 0.187 |
| 85-13 | 5 | 0.149 | 0.082 |
| 91-65 | 6 | 0.12 | 0.073 |
| 84-43 | 6 | 0.098 | 0.074 |
| 97-02 | 7 | 0.462 | 0.425 |
| 83-36 | 7 | 0.128 | 0.053 |
| 96-52 | 7 | 0.15 | 0.057 |
| 81-10 | 7 | 0.209 | 0.055 |
| 91-55 | 7 | 0.214 | 0.031 |
| 98-08 | 8 | 0.282 | 0.105 |
| 92-35 | 9 | 0.891 | 0.553 |
| X03-04 | 6 | 0.384 | 3.793 |
| 96-23 | 6 | 0.282 | 1.281 |
| X X02-11 | 6 | 0.107 | 0.54 |
| X 02-21 | 6 | 0.106 | 0.527 |
| Feb-13 | 6 | 0.094 | 0.365 |
| X00-71 | 6 | 0.177 | 0.351 |
| 97-66 | 7 | 0.193 | 1.947 |
| 01-Aug | 7 | 0.198 | 0.952 |
| X01-38 | 7 | 0.241 | 0.669 |
| MIB | CD | |
|---|---|---|
| # of Cases | 20 | 20 |
| Total value | 4.753 | 12.12 |
| Range | 0.094 - 0.891 | 0.031 - 3.793 |
| Mean | 0.238 | 0.606 |
| Std Deviation | 0.182 | 0.895 |
| Count of Increases | 11 | 9 |
| Count of Decreases | 9 | 11 |
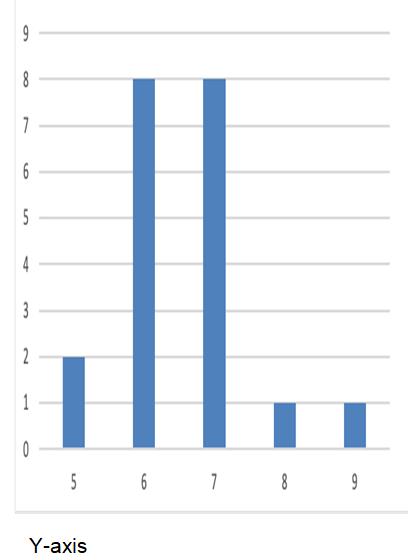
Table 3, Graph Figure 3 and Statistics: Prostate Cell Proliferation & Cell Death in African Americans.
Morphology of prostatic acini in cross sections is shown by histology, histochemistry, immunohistochemistry, and immunofluorescence by light microscopic study [3, 13, 21, 22, 23, 25, 26, 27] (Table 3). The prostate glands are separated from prostatic stroma by the acinar basement membrane (Graph Figure 1). Antibody IgG against actin localizes in smooth muscles in the stroma separating cancerous acini (Graph Figure 1). Many acini show light and dark cells and acinar lumen (Graph Figure 2). Previous study had shown that light cells were androgen-dependent (or sensitive) and dark cells were androgen- insensitive (androgen -independent) [28]. Micrograph shows cancer cells invading prostatic stroma and the acinar lumen shows sloughed prostatic cells (Graph Figure 3). Benign prostate has intact basement membrane and stroma. Green fluorescence of FITC shows cell proliferation, whereas rhodamine (red) fluorescence shows cell death. When cell proliferation and cell death localizations are combined yellow fluorescence is observed.
Discussion
The relationship between cell proliferation and cell death is poorly understood when studied separately. We did not get consistent results on cell proliferation and cell death for nearly 10 years. Others have studied cell proliferation and cell death separately [3, 18, 21, 22, 23, 25, 29, 30]. Adjacent and/or serial sections are required for consistent localization results of cell proliferation and cell death markers. We have shown that PC grows by cell proliferation in WA with Glasson scores 5 and 7 whereas, it grows AA with scores 6 and 7 tumors. Differences in the two races require differential diagnosis and treatment [31, 32, 33]. Specific reasons for differences are unknown, but could be related to food habits, herbicides and pesticides in foods and water, education, poverty, etc. Utilization of Gleason score-based diagnosis and treatment is expected to improve survival in each race. Current study in WA, AA races differs from our previous study of cathepsin B (a proteolytic enzyme) in Japanese Americans, and Japanese in Japan [23, 26]. Cathepsin B was similar in the above races. Cell proliferation and cell death study support the need for differential diagnosis and treatment in each race. We also suggest that aggressiveness of cancers ought to be determined prior to using hormonal, cytotoxic and/or radiation treatments.
We studied the ultrastructure of acinar secretory cells in benign prostate and benign prostatic hyperplasia (BPH) [28]. Study of untreated and DES-treated cases showed two types of PC, namely, androgen-dependent (sensitive) and androgen-independent (insensitive) [25]. Androgen deprivation treatment (ADT) treats only androgen- dependent (androgen-sensitive) cancer and not androgen independent cancer which is dependent on estrogen [25]. Androgen-independent (insensitive) PC can be treated by antiestrogen drug such as Tamoxifen. Subsequent study showed androgen-dependent PC has androgen-specific stem cells, and estrogen dependent PC has estrogen-specific-stem cells and their receptors [21]. As a reproductive biologist, the Author (AAS) studied pluripotential cells in blastocysts and found that these cells become organ-specific during organogenesis (3). For example, pluripotential cells in prostate, including stem cells and genes, become organ- specific including during organogenesis [3, 6, 8, 9, 15, 16, 17, 34, 35, 36]. Such specificity precludes application of gene therapy via unrelated organs. This may have been the reasons for the failure of gene therapy so far. Gleason study prostate tumor led to five patterns and the Gleason grading system [4, 19]. Gleason grading system is being used worldwide in diagnosis of PC.
The above discussion indicate that other solid organs cancers (such as, lungs, liver, colon, breast, pancreas, brain) can be dissected using a variety of techniques, namely, markers, phase contrast, light, and electron microscopy, etc. in the hope of finding variants in each solid organ cancer. Each variant could be readily targeted resulting in improved survival. Since President Richard Nixon declared war on cancer in 1971, numerous cancer patients have died throughout the world despite over several trillion dollars of expenses. Additional efforts are in dissecting solid organ cancers can result in improved diagnosis and treatments resulting improved survival of some PC patients in the two races.
Conclusion
PC grows due to the increased cell proliferation in scores 5 and 7in WA and scores 6 and 7 in AA when data is analyzed in relation to the Gleason scores. Our conclusion is supported by data in tables, statistical analysis, histological, Immunohistochemical and immunofluorescence figures. The differential growth of PC in the two races requires race-specific hormonal, radiation and/or chemo therapy treatments. The sequence and dosage have been determined in clinical trials.
Postscript comments: Black men are diagnosed with PC more than WA and die at a higher rate than WA. The reasons are complex and not fully understood. Some of the reasons may be associated with foods contaminated by herbicides and pesticides in food, and water. Disparity health care for AA men, women and children in the USA and the world, including the VA Medical System may contribute to the problem. Active efforts and surveillance are expected to reduce mortality in AA and other low income patients. There is a general mistrust in men and women of AA origin than in the VA Healthcare system. Efforts of surgeons and their associates did not result in obtaining consents of many AA patients. Inclusion of veterans’ family in the VA Health Care system has the possibility of improving the situation.
Scientist (AAS) published cell biology of benign (normal) prostate and benign prostatic hyperplasia (BPH) in 1973. He has had numerous discussions with Urologists, Pathologist, and prostate scientists including Dr. Donald F. Gleason on the treatments of prostate cancer. AAS has concluded that the best treatment for PC is prostatectomy followed by focused beam radiation to prostatic fossa and surrounding area between 4 and 8 months after sugary.
Acknowledgements
Conflicts of Interest
The authors have no conflict of interest.
No grant fund was used to complete this manuscript.
Disclaimer
The opinion expressed in this article is that of the author and not of the U.S. Government, Department of Veterans Affairs, or the University of Minnesota.
The Research Service of Minneapolis Veterans Affairs Medical Center provided laboratory and other research facilities. The VA did not pay any salary to AAS. The VA provided laboratory and office space. The Author retired on December 31, 2019. The Authors are grateful to Drs. Donald F. Gleason and Stephen L. Ewing for grading the prostate cancer sections, former staff pathologists at the Minneapolis VA Medical Center. We are also grateful to Drs. Pratap K. Reddy and Eduardo T. Fernandes and their associates for prostatectomy specimens. We are grateful to Ms. Jenifer Schwarzhoff (Morgan) and Ms. Kongit Betre for immunohistochemical and immunofluorescence studies. The author greatly appreciates the help of Mr. Don Frederiksen used photoshop for the uniformity of figures as needed and prepared tables and graph figures. Dorothy Sinha for proof reading and helpful Editorial Comments.
References
-
Siegel RL, Giaquinto AN, Jemal A (2024) Cancer statistics. CA Cancer J Clin 74(1): 12-49.
-
Ribatti D (2008) Judah Folkman, a pioneer in the study of angiogenesis. Angiogenesis 11(1) : 3-10.
-
Sinha AA (2022) Cell Proliferation in the Gleason Scores, Immunogold Localization of CD133 in the Stem Cells of Human Prostate, and Analysis of Embryonic Stem Cells, Including Organogenesis. IJBP 7(2): 1-10.
-
Gleason DF (1966) Classification of prostatic carcinomas. Cancer Chemotherapy Rep 50(3): 125-128.
-
Levesque C, Nelson PS (2018) Cellular constituents of the prostate stroma: key contributors to prostate cancer progression and therapy resistance. Cold Spring Harb Prospect Med 8(8):1-15.
-
Hall PA, Levison DA (1990) Review: Assessment of cell proliferation in histological material. J Clin Physiol 43(3): 184-192.
-
Carvalhal GF, Daudi SN, Kan D, Dana M, Stacy L, et al. (2010) Correlation between serum PSA and cancer volume in prostate glands of different sizes. Urology 76(5): 1071-1076.
-
Birnie R, Bryce SD, Roome C, Vincent D, Alastair D, et al. (2008) Gene expression profiling of human prostate cancer stem cells reveals a pro-inflammatory phenotype and the importance of extracellular matrix interactions. Genome Biology 9: 1-13.
-
Romar GA, Kupper TS, Divito SJ (2016) Research techniques made simple: Techniques to assess cell proliferation. J. Invest. Dermatology 136(1): 61-67.
-
Kerr JFR, Wyllie AH, Currie AR (1972) Apoptosis: a basic biological phenomenon with wide-ranging implications is tissue kinetics. Br J Cancer 26(4): 239-257.
-
Gold R, Schmie M, Giegerich G, Brietschopf H, Hartung HP, et al. (1994) Differentiation between cellular apoptosis and necrosis by combined use of in situ tailing and nick translation techniques. Lab Invest 71(2): 219-225.
-
Roche (2004) in situ Cell Death Detection Kit. Intergen.
-
Sinha AA, Hagen KA, Sibley RK, Wilson MJ, Reddy PK, et al. (1986) Analysis of fixation effects immunohistochemical localization of prostatic specific antigen in human prostate. J Urol 136(3): 722-727.
-
Cowen D, Troncoso P, Khoo VS, Zagars GK, Eschenbach AC, et al. (2002) Ki-67 staining is an independent correlate of biochemical failure in prostate cancer treated with radiotherapy. Clin Cancer Res 8(5): 1148-1154.
-
Houlahan KE, Livingstone J, Fox NS, Kurganovs N, Helen Z, et al. (2023) A polygenic two-hit hypothesis for prostate cancer. J Natl Cancer Inst 115(4): 468-472.
-
Verrma P, Shukla N, Kumari S, Ansari MS, Kumar N, et al. (2023) Review, Cancer stem cells (CSCs) in progression, progression metasesis, and metastasis and therapy resistance. Biochemica Cancer pp: 188887
-
Koukourakis IM, Platoni M, Kouloulias V, Arelaki S, Zygogianni A (2023) Prostate Cancer Stem Cells: Biology and Treatment Implications. Int J Mol Sciences 24(19): 14890.
-
Sinha AA, Bentley MD (1984) the relationship of epithelial cell types in the ventral prostate glands of castrated mice treated with testosterone. Anat Rec 208: 533-544.
-
Gleason DF (1977) Histologic grading and clinical staging of prostatic carcinoma. In: Tannenbaum M, et al. (Edn.), Urologic Pathology: The Prostate. Philadelphia pp: 171-213.
-
Ellis WJ, Lange PH (1994) Prostate cancer. EndocrinoL Metab Clin North Am 23(4): 809-824.
-
Sinha AA, Wilson MJ (2018) Identification of two types of stem cells in methylene blue-stained sections of untreated and diethylstilbestrol-treated human prostate cancer and their characterization by immunogold localization of CD133. Anticancer Res 38(10): 5725- 5732.
-
Sinha AA, Quast BJ, Wilson MJ, Reddy PK, Gleason DF, et al. (1998) Co-distribution of pro- cathepsin B and mature cathepsin B forms in human prostate tumors detected by confocal and immunofluorescence microscopy. Anat Rec 252(2): 281-289.
-
Sinha AA, Wilson MJ, Gleason DF (1987) Immunoelectron microscopic localization of prostatic-specific antigen in human prostate by the protein A-gold complex. Cancer 60(6): 1288-1293.
-
Stamey TA, Ekman PE, Blankenstein MA, Cooper EH, Kontturi M, et al. (1994) Tumor markers. Consensus Conference on Diagnosis and Prognostic Parameters in Localized Prostate Cancer. Stockholm, Sweden, May 12- 13, 1993. Scand J Urol Nephrol Suppl 162: 73-87.
-
Kyprianou N, Bruckheimer EM, Guo Y (2000) Cell proliferation and apoptosis in prostate cancer: significance in disease progression and therapy. Histol Histopathol 15(4): 1211-1223.
-
Sinha AA, Morgan JL, Buus RJ, Ewing SL, Fernandes ET, et al. (2007) Cathepsin B Expression is Similar in African American and Caucasian Prostate Cancer Patients. Anticancer Res 27(5A): 3135-3142.
-
Sinha AA, Morgan JL, Betre K, Wilson MJ, Le C, et al. (2008) Cathepsin B expression in Native Japanese and Japanese American prostate cancer patients: An immunohistochemical study. Anticancer Res 28: 2271- 2277.
-
Sinha AA, Blackard CE (1973) Ultrastructure of prostatic benign hyperplasia and carcinoma. Urology 2(2): 114- 120.
-
Sinha AA, Blackard CE, Seal US (1977) A critical analysis of tumor morphology and hormone treatments in the untreated and estrogen-treated responsive and refractory human prostatic carcinoma. Cancer 40(6): 2836-2850.
-
Aihara M, Scardino PT, Truong LD, Wheeler TM, Goad JR, et al. (1995) The frequency of apoptosis correlates with the prognosis of Gleason Grade 3 adenocarcinoma of the prostate. Cancer 75(2): 522-529.
-
Wang Y, Ma Y, Jiang K (2023) The role of ferroptosis in prostate cancer: a novel therapeutic strategy. Prostate Cancer and Prostatic Diseases 2023: 26: 25-29.
-
Zellweger T, Kim Chi K, Miyake, H, Adomat H, Kiyama S, et al (2002) Enhanced radiation sensitivity in prostate cancer by inhibition of the cell survival protein clusterin. Clin Cancer Res 8(10): 3276-3284.
-
Guo Y, Sigman DB, Borkowski A. Kyprianou N (2000) Racial differences in prostate cancer growth: apoptosis and cell proliferation in Caucasian and African-American patients. Prostate 42(2): 130-126.
-
Xu J, Stolk JA, Zhang X, Silva SJ, Houghton RL (2000) Dentification of Differentially Expressed Genes in Human Prostate Cancer Using Subtraction and Microarray. Cancer Res 60(6): 1677-1682.
-
Mei W, Lin X, Kapoor A, Gu Y, Zhao Y, et al. (2019) The Contributions of Prostate Cancer Stem Cells in Prostate Cancer Initiation and Metastasis. Cancer (Basel) 11(4): 434.
-
Wolf I, Gratzke C, Wolf P (2022) Prostate Cancer Stem Cells: Clinical Aspects and Targeted Therapies. Genitourinary Oncologyy: Front Oncol 12: 935715.
- Superposition of Cryo-EM and AlphaFold Predictions of Dengue Antigen-Antibody Complexes
- Jugular-Applied Coherent Low-Level Laser Therapy Enhances Systemic Mitochondrial Metabolic Function and Antioxidant Response
- Role of OMC32 Polypeptide in Acrosin-Mediated Exocytosis during the Bovine Sperm Acrosome Reaction
- Association of Galectin-3 but not Laminin in Tamoxifen-Induced Growth Suppression in Breast Cancer MCF-7 Cells
- Effect of Different Wavelengths of Light on the Rate of Photosynthesis
- Nutritional, Therapeutic, and Environmental Effect of Oyster Mushrooms: An Editorial