A Two Year Autopsy Study on Coronary Artery Stenosis
Sudden cardiac death is a medicolegally challenging autopsy. One may wonder, why? Even as coronary artery disease is the reigning cause of sudden death throughout the world, it was found that most of the literature available has emphasized either on correlation between increasing coronary artery stenosis with increasing age or increased incidence of myocardial ischemia with increasing coronary artery stenosis. In the autopsies carried out in Sri Aurobindo Medical College & P.G.I, Indore, it has been found that there has been a shift of increasing incidence of coronary artery stenosis and myocardial ischemia in younger age groups [31-40 yrs]. Myocardial ischemia was present even when there was only 10-15% stenosis of the right coronary artery. It was also deduced that there has been an increasing incidence of coronary artery stenosis in thin to average built males while in obese people the coronaries were found to be fully patent establishing no significant correlation between body mass index and degree of coronary artery stenosis.
Introduction
Coronary artery disease, popularly quoted as `The Captain of the Men of death’ is the most common cause of unanticipated deaths [1]. 17.7 million people die each year from cardiovascular disease, an estimated 31% of all deaths worldwide of which more than 75% occur in low- income and middle-income countries [2]. This reveals the magnanimity of the problem. These deaths are categorised as natural deaths but they carry medicolegal significance as they may cause death in young and asymptomatic individuals raising suspicion of foul play. In some cases, especially geriatric population where some degree of coronary artery stenosis is nearly always present, the cause of death can be inaccurately concluded as “coronary artery disease”. Road traffic accidents and death due to assault may be complicated by concurrent presence of coronary artery stenosis, making the inference regarding cause of death similar to the question- ‘the egg came first or the hen’.
Material and Methods
The study was conducted in a span of two years on 120 autopsies performed at Sri Aurobindo Medical College & P.G.I, Indore. The aim of this research was to note the severity of coronary artery stenosis and its relation with parameters like age, body mass index and association with myocardial ischemia.
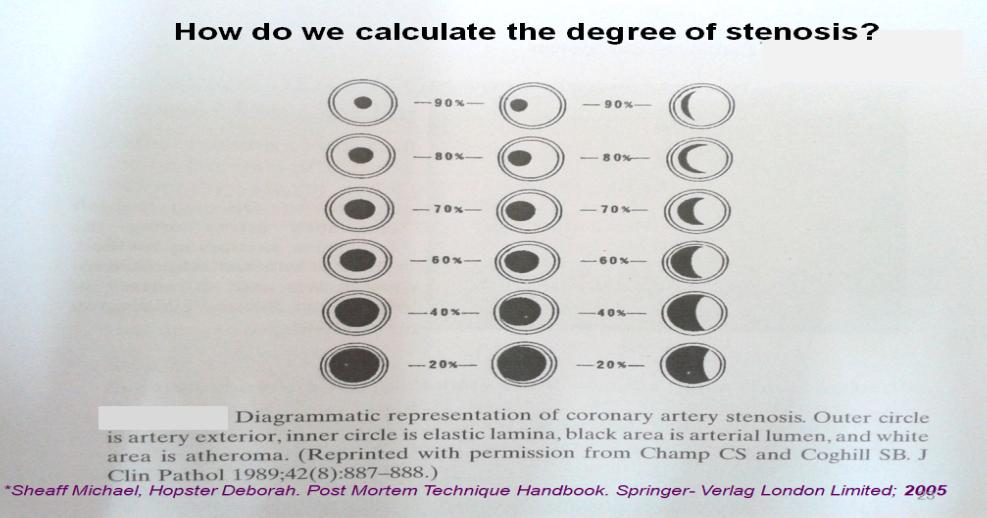
An elaborate history was taken from the relatives, data from hospital records was procured and a detailed autopsy was conducted where the heart and its coronaries were meticulously observed and dissected. The left main, the left circumflex, the anterior descending, the right main and the posterior descending coronaries were examined by cutting at regular intervals (2-3 mm) for the degree of stenosis, atheromatous plaque, superimposed thrombus, calcification or hemorrhage.
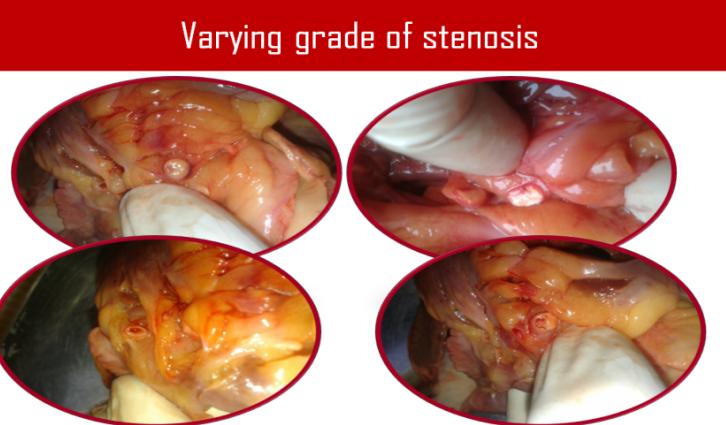
Figure 1: Section of heart stained by T.T.C method reveals a part of normal myocardium which reacts with the buffered oxidation reduction reagent in solution and gets stained. The stained myocardium is red. There is loss of endogenous substrates, coenzymes and dehydrogenases in the infracted tissue and therefore there is no reaction with the regents and hence the infarcted area remains unstained.
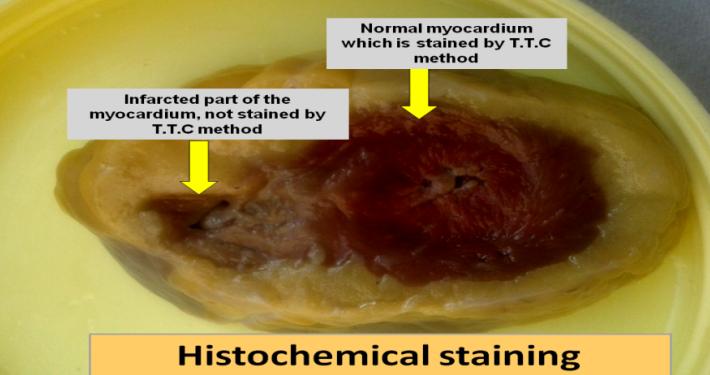
This was followed by cutting the heart into transverse slices 10 mm thick, proceeding upwards from apex to valve and examining them for gross signs of ischemia like hyperemia, yellowing, mottling, scarring. If ischemia was suspected on gross examination, T.T.C test or N.B.T test was performed (Figures 1-4), which is based on the principle that the normal myocardium reacts with TTC reagent to give red stain and with Nitro B.T to give reddish blue stain in solution. However due to the loss of enzymes and vital reaction, the infracted myocardium does not react with the reagent and hence remains unstained.
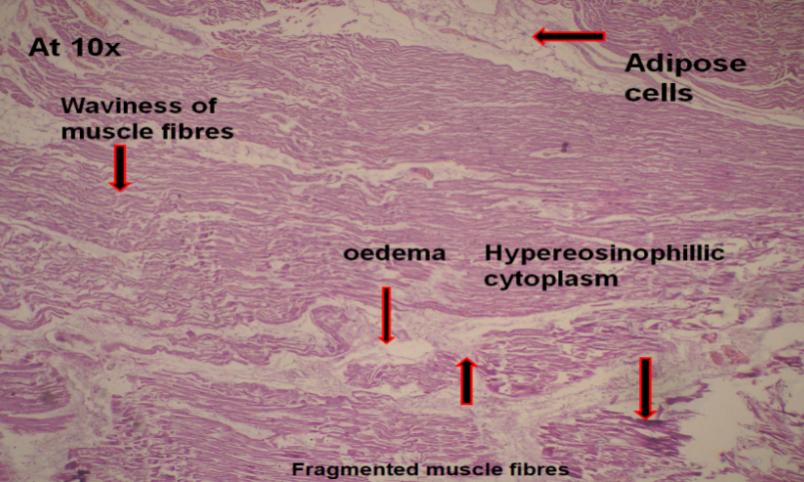
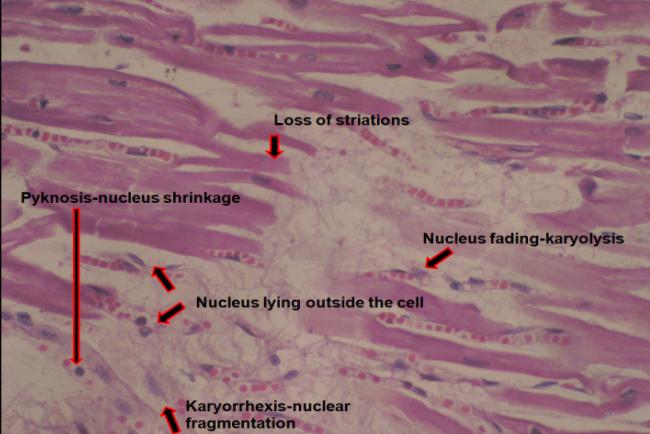
Figure 3 (a, b, c): Histopathology of the hyperemic areas of myocardium reveals ischemic changes.
Observation
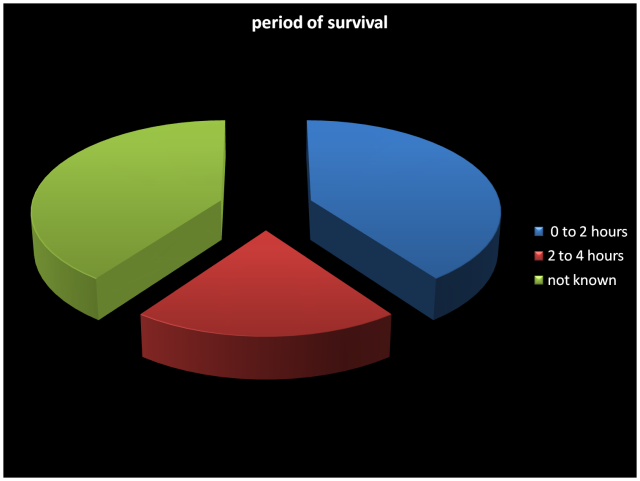
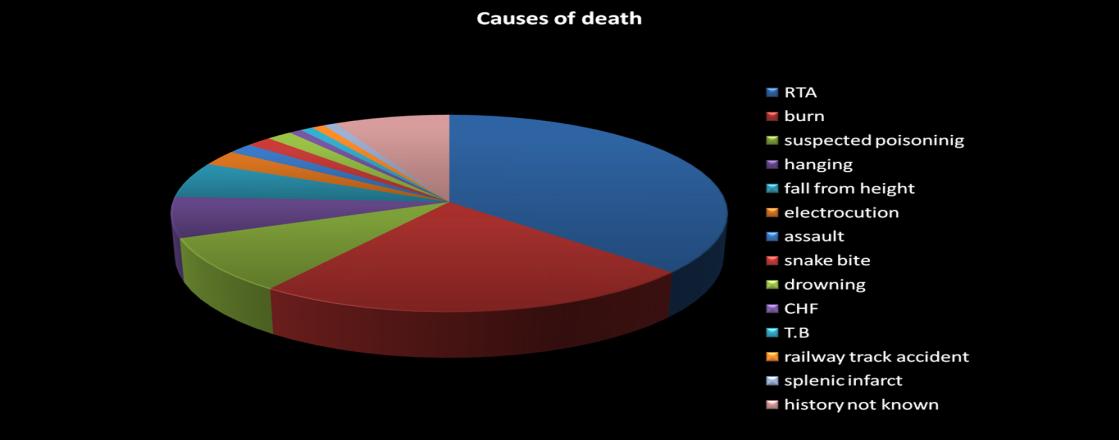
Amongst the 120 cases studied in the present research, 90 were male victims and the rest 30 were females. (Tables 1-3) where the causes of death documented were widely varied (Figure 5). The luminal narrowing of coronaries was graded from 0-5, ( Grade 0 no stenosis; Grade 1 stenosis occluding less than 25% of the lumen; Grade 2 stenosis occludes 25 to 50% of the lumen; Grade 3 stenosis occludes 50 to 75% of the lumen; Grade 4 stenosis occludes more than 75% of the lumen) (Figure 2 & 5). Incidence of stenosis of the various arteries for all the subjects was noted (Table 4). Ischemic changes in the myocardium were detected by gross histochemical staining in a total of 5 cases out of the 120 hearts studied (Table 5). All five were males in the age group of 35 to 40 years. In one case the subject was underweight, in 3 cases the subjects were within normal limits of BMI while one subject was obese (Figure 7). The periods of survival taken from the onset of the episode chest pain leading up to death ranged from ½ an hour to 4 hours (Figure 6). Weight of the hearts in 4 cases where ischemic changes were found was 300-400 gm and 400- 500 gm in 1 case.
BMI
less than 18.5
18.5-25 more than 25 $$ = \frac {1}{2} $$
$$ = \frac {1}{2} $$ $$ = \frac {1}{2} $$
20%
20%
60% Figure 5: Body mass index of the study subjects.
| Age group | Males | Females | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 21-30 | 29 | 16 | 45 | ||||||||
| 31-40 | 28 | 8 | 36 | ||||||||
| 41-50 | 20 | 4 | 24 | ||||||||
| 51-60 | 10 | 2 | 12 | ||||||||
| 61-70 | 2 | 0 | 2 | ||||||||
| 71-80 | 0 | 0 | 0 | ||||||||
| 81-90 | 1 | 0 | 1 | ||||||||
| Total | 90 | 30 | 120 |
Table 2: Of the 120 cases studied 90 were males and 30 were females. The age wise distribution of cases is given.
- Arteries
- Grade of Stenosis
- Total
- %
- 0
- 1
- 2
- 3
- 4
- R1
- 9
- 20
- 1
- 0
- 0
- 21
- 70%
- R2
- 13
- 17
- 0
- 0
- 0
- 17
- 56%
- R3
- 20
- 10
- 0
- 0
- 0
- 10
- 33%
- L1
- 9
- 18
- 1
- 2
- 0
- 21
- 70%
- L2
- 7
- 21
- 1
- 1
- 0
- 23
- 76%
- L3
- 29
- 1
- 0
- 0
- 0
- 1
- 3%
Table 1: Incidence of stenosis of the various arteries in the
origin
- R2- Right coronary artery for a distance of 2cm from origin
- R3- Right coronary artery for a distance of 3cm from origin
- L1- Left common coronary artery
- L2- Left anterior descending artery
- L3-Left circumflex artery
- Grade 0 – No stenosis
- Grade 1- 0-25% stenosis
- Grade 2- 25-50% stenosis
- Grade 3- 50-75% stenosis
- Grade 4- 75-100% stenosis
| Arteries | Grade of Stenosis | Total | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | No | % | |||||||
| R1 | 53 | 37 | 6 | 1 | 0 | 37 | 41.1 | ||||||
| R2 | 58 | 32 | 0 | 1 | 0 | 32 | 35.5 | ||||||
| R3 | 63 | 27 | 0 | 0 | 0 | 27 | 30 | ||||||
| L1 | 33 | 57 | 2 | 6 | 4 | 57 | 63.3 | ||||||
| L2 | 40 | 50 | 7 | 5 | 8 | 50 | 55.5 | ||||||
| L3 | 53 | 37 | 3 | 6 | 1 | 37 | 41.1 |
Table 3: Incidence of stenosis of the various arteries in male cases.
| Arteries | Grade of Stenosis | Total | % | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | |||||||||||
| R1 | 62 | 57 | 7 | 1 | 0 | 65 | 54.2% | ||||||||
| R2 | 71 | 49 | 0 | 1 | 0 | 50 | 41.7% | ||||||||
| R3 | 83 | 37 | 0 | 0 | 0 | 37 | 30.8% | ||||||||
| L1 | 42 | 75 | 3 | 8 | 4 | 90 | 75% | ||||||||
| L2 | 47 | 71 | 8 | 6 | 8 | 93 | 77.5% | ||||||||
| L3 | 82 | 38 | 3 | 6 | 1 | 48 | 40% |
Table 4: Incidence of stenosis of the various arteries for all subjects.
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | Grade 4 | Total | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R1 | 0 | 4 | 1 | 0 | 0 | 5 | ||||||||||||
| R2 | 0 | 4 | 0 | 1 | 0 | 5 | ||||||||||||
| R3 | 2 | 3 | 0 | 0 | 0 | 3 | ||||||||||||
| L1 | 2 | 1 | 0 | 0 | 2 | 3 | ||||||||||||
| L2 | 2 | 1 | 1 | 1 | 0 | 3 | ||||||||||||
| L3 | 2 | 1 | 1 | 1 | 0 | 3 |
Table 5: The Incidence of coronary artery stenosis in the cases revealing ischemic changes after staining.
Complete occlusion of the lumen in RCA was not encountered in any of the cases. In the LAD it was seen in 4 cases out of which a thrombus was found in 1 case. Overt valvular lesions were found in 3 cases. Only in 1 case did gross examination reveal mottled hemorrhagic appearance of infarct which was stained histochemially. In the other 4 cases gross examination did not reveal any evidence of fresh infarction, which were revealed only by staining. 3 cases out of 5 showed only subendocardial infarcts. 2 cases had revealed transmural infarct (Figure 8). Location of the infracted areas was noted (Figure 9).
Frequency of type of infarcts
40% trasmural $$ \square $$ subendocardial
60% Figure 8: Frequency of type of infarcts.
Location of infarcts in LV after staining
Correlation of Grade of stenosis of R1, R2, R3, L1, L2, L3 and ischemic changes detected by staining is described in Tables 6-11.
| 0 | 1 | 2 | 3 | 4 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ischemic | 62 | 53 | 6 | 1 | 0 | ||||||
| changes absent | (100%) | (92.9%) | (85.7%) | (100%) | (100%) | ||||||
| Ischemic | 0 | 4 | 1 | 0 | 0 | ||||||
| changes present | (0%) | (7%) | (14.3%) | (0%) | (0%) |
Table 6: Correction of grade of stenosis of R1 and ischemic changes detected by staining.
| 0 | 1 | 2 | 3 | 4 | ||||
|---|---|---|---|---|---|---|---|---|
| lschemic | 71 | 45 | 0 | 0 | 0 | |||
| Changes absent | (100%) | (91.8%) | (100%) | (0%) | (100%) | |||
| lschemic | 0 | 4 | 0 | 1 | 0 | |||
| changes present | (0%) | (8.2%) | (0%) | (100%) | (0%) |
Table 7: Correction of grade of stenosis of R2 and ischemic changes detected by staining.
| 0 | 1 | 2 | 3 | 4 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Ischemic | 81 | 34 | 0 | 0 | 0 | |||||
| Changes absent | (97.6%) | (91.9%) | (100%) | (100%) | (100%) | |||||
| Ischemic | 2 | 3 | 0 | 0 | 0 | |||||
| Changes Present | (2.4%) | (8.1%) | (0%) | (0%) | (0%) |
Table 8: Correction of grade of stenosis of R3 and ischemic changes detected by staining.
| 0 | 1 | 2 | 3 | 4 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Ischemic | 40 | 74 | 3 | 8 | 2 | ||||
| Changes absent | (95.2%) | (98.7%) | (100%) | (100%) | (50%) | ||||
| Ischemic | 2 | 1 | 0 | 0 | 2 | ||||
| Changes Present | (4.8%) | (1.3%) | (0%) | (0%) | (50%) |
Table 9: Correction of grade of stenosis of L1 and ischemic changes detected by staining.
| 0 | 1 | 2 | 3 | 4 | ||||
|---|---|---|---|---|---|---|---|---|
| Ischemic | 45 | 70 | 7 | 5 | 8 | |||
| Changes absent | (95.7%) | (98.6%) | (87.5%) | (83.3%) | (100%) | |||
| Ischemic | 2 | 1 | 1 | 1 | 0 | |||
| Changes Present | -4.3% | -1.4% | -12.5% | -1.7% | (0%) |
Table 10: Correction of grade of stenosis of L2 and ischemic changes detected by staining.
| 0 | 1 | 2 | 3 | 4 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Ischemic | 80 | 37 | 2 | 5 | 1 | ||||
| Changes absent | (97.60%) | (97.40%) | (66.70%) | (83.30%) | (100%) | ||||
| Ischemic | 2 | 1 | 1 | 1 | 0 | ||||
| Changes Present | (2.4%) | (2.6%) | (33.3%) | (1.7%) | (0%) |
Table 11: Correction of grade of stenosis of L3 and ischemic changes detected by staining.
Discussion
Some degree of stenosis was noted in all victims above the age of 30 years, the youngest male and female subjects being 21 years of age. This is in agreement with Strong & McGill [3]. Morris who concluded that there is no straightforward association between atherosclerosis and ischaemic heart disease, which was also found in our study [4]. This however is in conflict with studies by Crawford, Dexter, Teare Strong and McGill [3, 5]. A direct link was noted between the sex of the subject (more in males) and myocardial ischemia, which is similar to findings by Strong and McGill3 while this is contrary to a study by Roberts, Moses and Wilkins [6, 7].
While trying to correlate myocardial ischemia with the grade of stenosis in the coronary arteries, no simple correlation could be deduced, as even with just 25% coronary artery stenosis, ischemic changes were found.
In the current study, T.T.C staining technique gave a positive reaction for 5 out of 120 hearts studied, thus revealing infracted area of myocardium in these 5 hearts, with the earliest infarct to be detected being of half hour duration, which was similar to Fine & also Andersen and Hensen [8, 9]. Sandritter and Jestadt, Mc Vie, Nachals and Shnikta and Ramkisson, studies could detect ischemic changes 8 hours after onset of symptoms [10, 11, 12, 13].
4 hearts out of 120 cases in the current study, weighed more than 400 gms, of which 2 hearts did not reveal ischemic changes, while the other two had transmural infarcts in left ventricle.
Results & Conclusion
Ischemic changes in the myocardium were detected by gross histochemical staining & histopathology in a total of 5 cases out of the 120 hearts studied.
All five were males in the age group of 35 to 40 years. In 1 case the subject was underweight, in 3 cases within normal limits of BMI.
Hence, increasing incidence of stenosis and ischemic changes is seen in young, thin built males with no significant correlation between degree of stenosis and ischemic changes.
Through this paper we want to highlight the uptrend in cases of sudden death from coronary artery disease in seemingly healthy young males. In such cases, imminent death from cardiac cause is phantasmal. Thus ante mortem investigations for a timely diagnosis which could possibly be life saving are missed and the same continues after death, leading to an obscure autopsy. Perspicacity is the need of the hour.
References
-
Marzilli M, Merz CN, Boden WE, Bonow RO, Capozza PG, et al. (2012) Obstructive Coronary Atherosclerosis and Ischemic Heart Disease. JACC 60(11): 951-956.
-
http://www.who.int/cardiovascular_diseases/public ations/en/
-
Strong JP, McGill HC (1962) The Natural History of Coronary Atherosclerosis. Am J Pathol 40: 37-49.
-
Morris JN, Crawford MD (1958) Coronary Heart Disease and Physical Activity of Work. Br Med J 2(5111): 1485-1496.
-
Crawford T, Dexter D, Teare RD (1961) Coronary- Artery Pathology in Sudden Death from Myocardial Ischaemia. The Lancet 1: 181-185.
-
Roberts JC Jr, Moses C, Wilkins RH (1959) autopsy studies in atherosclerosis. I. Distribution and severity of atherosclerosis in patients dying without morphologic evidence of atherosclerotic catastrophe. Circulation 20: 511-519.
-
McGill HC (1968) Fatty Streaks in the Coronary Arteries and Aorta. Lab Invest 18(5): 560-564.
-
Fine G, Moreales A, Screpella JR (1966) Experimental myocardial infarction. A histochemical study. Arch Path 82(1): 4-8.
-
Hansen BF (1978) Heart autopsy in ischaemic heart disease. An autopsy protocol. Acta Path Microbiol Scand A 86(3): 241-244.
-
Sanditter, Jestadt (1958) TTC als Reduktionsidikater Makroscopik diagnosedes frischen herzinfarktes Zent. Allg Pathol 97: 188-189.
-
McVie JG (1970) Postmortem detection of in apparent myocardial infarction. J Clin Path 23: 203-209.
-
Nachlas MM, Shnikta TK (1963) Macroscopic identification of early myocardial infarcts by alterations in dehydrogenase activity. Am J Path 42(4): 379-405.
-
Ramkisson RA (1966) Macroscopic identification of early myocardial infarction by dehydrogenase alteration. J Clin Path 19(5): 479-481.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review