Poisons and Drugs Used in Homicidal Poisoning: A Systematic Review
Homicidal poisoning defined as the application of toxic agents by a person to kill human beings. Historically, some conventional homicidal poisons were including arsenic, cyanide, mercury, strychnine, aconite and atropine. In general, homicidal poisonings are among the least frequently detected crimes and difficult to establish, across the world. Lack of suspicion of this type of poisoning and clinical presentations in this poisoning are often misdiagnosed as natural disease, especially if the crime is occurred in a hospital setting are the limitations for detection of homicidal poisonings. The aim of this article is to review of drugs and poisons used in recently reported homicidal poisoning cases. The results showed that the contemporary poisons and drugs used in homicidal poisonings are based in combinations of old and well-described poisons and drugs and natural or synthetic drugs and poisons from the group of organophosphorus agents, tetrodotoxin, radioactive substances and polydrug pattern of antipsychotics with antidepressants and sedativehypnotics. Forensic autopsy and postmortem histopathological and toxicological analysis have a critical role in investigation on homicidal poisoning fatal cases. The sophisticated instrumental analysis (usually using tandem mass spectrometry) can be used for toxicological analysis of trace levels of drugs and poisons in routine and alternative samples in the victims of homicidal poisoning.
Introduction
Homicidal poisoning defined as the application of toxic substance(s) by a person to kill human beings [1].
Historically, poisons are the favorite tool for murder and known as “Secret Weapons”. The ideal characteristics of a homicidal poison is that it should be odorless, tasteless, colorless, well solubility in water (capability of substance administered via food or drink of victim), cheap, easily available, highly toxic (can be lethal in small doses), produces similar signs and symptoms of natural diseases, no antidote available, delayed action, chemically stable and shows no postmortem changes. Also, it is most important that poison should not be detected in the postmortem samples [2, 3].
Historically, some conventional homicidal poisons can be categorized in herbal, animal and minerals types were including arsenic, cyanide, mercury, strychnine, aconite and atropine [2]. In addition, drugs like opium, digitalis and henbane have been used in assassination since ancient times [3, 4].
Most of victims of homicidal poisoning are the end- stage and psychopathic patients, drug addicts, unwanted spouses, lovers, the elderly and the children [2]. Usually, the perpetrator is personally involved with the victim and is often assume the role of a medical staff or caregiver. Caregiver access to restricted drugs or chemicals and when the victim received medical treatment. Poisoners often deduce pleasure from suffering of the victims [2]. Also, sudden deterioration of health status or death are considered as “red flags” that indicate homicidal poisoning [2].
Homicidal poisoning remain rare and poorly described phenomenon [5]. In general, homicidal poisonings are among the least frequently detected crimes and difficult to establish, around the world [3]. Several limitations are in the detection of homicidal poisonings. For example, lack of suspicion of this type of poisoning and clinical presentations in this poisoning are often misdiagnosed as natural disease, especially if the crime is occurred in a hospital setting [3, 6].
The frequency of homicidal poisoning and poison and drugs used in the poisoning is different in the world. Muazzam, et al. [7] showed that there were 463 homicidal poisoning deaths with the rate remained the same during 2003-2007 in the United States [7]. The highest rates were among aged 0-19 years (rate=0.05), males (rate=0.04) and blacks (rate=0.06) [7].
In a retrospective study in China, the author collected data on 106 cases of homicidal poisoning from 1995 to 2000. From total of 106 cases, 58 deaths have been occurred. The poisoned victims included a high proportion of female, elderly, well-educated individuals and residents living in rural and urban areas. Individuals living in rural areas most often used pesticides, and people in urban areas have greater access to drugs obtained at workplace or online. In this study, tetramine (or tetramethylenedisulfotetramine, is an internationally banned compound that had been used as a rodenticide) and paraquat (or dipyridylium is a highly toxic herbicide) caused many of the deaths [8, 9].
In another study, various studies and case reports on homicidal poisoning from different parts of India has been analyzed. This study showed that homicidal poisoning prevalence varies from 0.3% to 3.7% and having varied prevalence from different regions in this country. The common poisons used in homicide were organophosphates, aluminum phosphide, paraquat, arsenic and methanol [10].
In a study which has been done in Sweden on homicidal poisoning cases during 1992-2019, 29 cases as homicidal poisoning were identified (1.2 per 10 million/year; representing 1.1% of all homicides).
Incidence peaked at age extremes with 0–4 and 69% were females. Pharmaceutical and narcotic drugs, some of which were given in combination including opioids, Z-hypnotics, benzodiazepines and phenothiazines were used in 90% of cases. Most of offenders (86%) were family members [11].
Gauthey, et al. [12] conducted an observational study of a prospectively collected cohort using the 47 participating sites of the Toxicology Investigators Consortium Registry (a North American research consortium). They identified 60 patients with malicious or criminal poisoning who presented to the emergency department between January 2014 and June 2017. From these patients, 21 (35%) were children. Among 21 children, 17 (81%) were less than 2- year old. The main toxic agents involved in pediatric intoxicated patients were sympathomimetics (35%) and opioids (19%). In adults, a more varied presentations of offending substances was used, with no specific toxidrome. Mortality rate was 5% (two children and one adult were died) [12].
Poisonous substances used in homicidal poisoning have changed over the period of time. Historical evidences from ancient civilizations such as Greece, Egypt, Iran, India and China showed that they had been used from natural – based poisons in homicidal poisoning [13].
In spite of the progress in new analytical technologies to identify drugs and poisons in biological and non-biological samples, the poisoners also were in the search of new poisons and its carrier vehicle [13].
Also, knowledge of poisons and poisoning has become more widespread because of the accessibility to information and communications technologies (internet and the social media). Finally, the tendency of criminals to use newer drugs and poisons with difficulties in their detection has increased.
Forensic investigations play a very important role in identifying the poisonous agent’s involvement in cases of homicidal poisoning and death. The review of reported criminal poisonings in the recent years will lead to more information of drugs and poisons implicated in this type of poisoning. From this view, the aim of this article is to review of drugs and poisons used in recently reported homicidal poisoning cases.
Methods
Search Strategy
We conducted the study in accordance with the Preferred Reporting Item for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We searched PubMed (pubmed.gov) and Google Scholar (scholar.google.com) using “Homicidal poisoning” OR “Criminal poisoning” as keyword words. We searched all articles from January 1, 2010 to September 30, 2023 that described human cases of homicidal poisoning.
Inclusion and Exclusion Criteria
All type of articles describing homicidal poisoning were included. Forensic-based studies and reports of forensic cases (including clinical presentations, autopsy findings, postmortem histopathological and toxicological analysis) were included. Finally, we excluded articles that were had insufficient data, no toxicological analysis data or undetected poisonous agent. We evaluated the titles and abstracts, and full-text of the articles. Also, non-English publications were excluded.
Data Collection
We extracted the following data, when available: the number, age, and gender of victim(s), route of exposure (ingestion, injection, dermal), poison name, poison’s vehicle (e.g. food, drinks, pharmaceutical dosage form), offender identity and relationship with victim(s), clinical signs and symptoms, poisoning outcome (survived or death), forensic autopsy findings (including postmortem toxicological and histopathological analysis).
Results
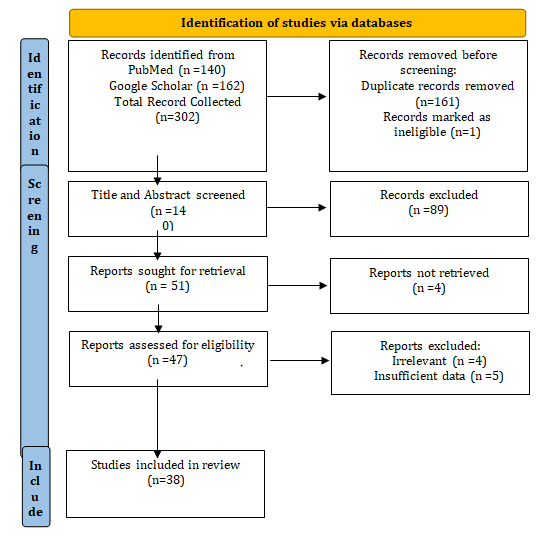
The initial search identified 302 publications. Based on the screening process, 162 duplications and ineligible were removed. Of the remaining 140 articles, we excluded 89 papers after screening the titles and abstracts. We performed full-text review of the remaining 51 eligible papers, excluding an additional 13 papers based on duplication, irrelevant, and/or insufficient data. Finally, 38 papers met our inclusion criteria and were reviewed. Figure 1 showed our search strategy. The included articles involve cases from different countries across the world.
Table- 1 shows a brief description of the included studies in this review. We found 81 cases of homicidal poisoning in this review. Among them, 40 (49.38%) cases were male while 41 (50.62%) were female. The age of the victims was specified in only 50 cases. Among these cases, age mean was 39.75 years old (range: one- month - 95 years old). Among these cases, the most impacted was the ≤50-year-old population (68%). There were 47 (58.02%) fatal cases and 34 (41.98%) cases were survived. In most cases, the poison was administered orally [61 (75.30%) cases]; following injection route [9 (11.11%) cases; including intravenous: 5 cases; subcutaneous: 3 cases and intraperitoneal injection: one case]; dermal [4(4.94%) cases]; inhalation [2 (2.59%) cases]; envenomation [3 (3.70%) cases]. Totally, simultaneous dermal and injection exposure and oral with dermal administration were reported in two cases.
| Name of Poison/ Drug(s) | Victim age, gender and number | Route of exposure | Poison’s vehicle | Offender identity | Clinical signs and symptoms | Poisoning outcome | Forensic autopsy/ toxicological findings | Refe rence No. |
|---|---|---|---|---|---|---|---|---|
| Strychnine | A 35-year-old woman | Oral | Empty amoxicillin capsules | Her husband | Tremor, Muscular spasms, Generalized convulsions, Conscious during convulsions, Complete relaxation between convulsions, Respiratory / cardiac arrest | Died | Postmortem histopathological findings: The external and internal examination did not show any signs of significant change Strychnine was detected in the liver (91 mg/kg wet weight), blood (2.14 mg/mL), urine (2.35 mg/mL) and stomach contents (137 mg/ kg wet weight) | [14] |
| Thallium | A married couple (49-year-old woman and 50-year-old man) | Oral | Table Salt | An offender | Numbness and tingling in the fingers and soles of feet. Progressing to involvement of hands and a stubborn ache in the bottoms of the feet. Numbness, allodynia. Mees’ lines in nails, Alopecia, Primary weakness in the limbs and atrophy of the musculature, perioral dermatitis, and stomatitis in the female | Died | Postmortem histopathlogical findings: Brain: Edema, encephaledema, necroses of neurons, proliferation and necrosis of glial cells, focal neuronophagia, and satellitosis, amyloid corpuscles were deposited in the corpus callosum and hippocampus Kidney: Edema, tubular casts, limited vacuolization, coagulative necrosis, and autolysis in the proximal convoluted tubules Lung: Multifocal edema, hyaline membrane, bronchopneumonia Liver: Focal necrosis, hydropic degeneration, and macrovesicular steatosis were noted in hepatocytes Hair: Electron microscopy revealed a dystrophic condition of hair with disorganized cuticle and atrophy of the hair bulb Postmortem Toxicological findings: Thallium concentrations(µg/mL) were in hair (F: 10.20, M: 13.75); Blood (F: 0.019, M: 0.15), Urine (F: 3.15, M: 3.60); Brain (F: 2.03, M: 2.58); Liver (F: 0.98, M: 5.08); Kidney (F: 0.98, M: 2.21); Heart (0.57, M:1.83); Lung (0.46; M: 0.88) and Stomach (F: 0.38, M: 4.02) | [15] |
| Thallium | A 23-year-old woman | Oral | Tea | Her business colleague | Muscle pain in both thighs that spread gradually to the lower legs. Plantar numbness and gastrocnemius muscle pain, with nausea, abdominal pain, and hair loss in temporal region | Survived | Clinical Toxicology findings: The thallium levels of the blood and urine measured on day 10 were 223 μg/L and 351 μg/L, respectively. | [16] |
| Thallium | 8 members of a same family (Father 92- year old, mother 89 years old, their caregiver, mother and father-in Law and 3 daughters | Oral | Herbal infusion | Grandson of the victims | Systemic malaise, dysentery, nausea, vomit, swelling, lack of energy, numbness, formication of the lower limbs, a sense of skin burning and fever | Three fatality (elderly couple and their oldest daughter and other 5 members were survived | Histopathlogical findings: Cerebral hemorrhage, pleural petechiae, bilateral inflammation of the inferior pulmonary lobes cardiomegaly, atherosclerosis and hepatic steatosis. Postmortem Toxicological findings: Thallium levels (µg/mL): Father (Blood: 2.75; Urine: 1.49; Gastric content: 1.93; Hair: 10.11 ng/mg) Mother (Blood: 1.15; Gastric content: 1.11; Hair: 1.38 ng/mg) Daughter (Blood: 6.01; Gastric content: 3.43; Hair: 5.72 ng/ mg) | [17] |
| Arsenic | Thirteen persons (56% were men and 46% women) (age range: 1-79 years) in a rural church gathering | Oral | Coffee | A church member | Gastrointestinal symptoms (nausea, vomiting abdominal pain, diarrhea), Multisystem organ failure (in two cases) | Eight persons were hospitalized, and 5 were evaluated and discharged home. One person died | Blood arsenic concentrations were in eight cases with a range of 68– 192 µg⁄L (reference range 60 µg ⁄L or less). Emesis samples from two cases had arsenic concentration of 190 and Arsenic levels in leftover cup of coffee and in residual coffee from the brewing pot were 240 µg⁄L and 3500 mg ⁄L, respectively. | [18] |
| Arsenic | A 50-year-old man | Oral | Meal | An offender | Diarrhea, vomiting, general malaise, abdominal tenderness, mild fever, numbness in arms and legs, Blurring of vision. Weigh lost (approximately 15 kg) | Died | Postmortem histopathlogical findings: Bilateral pleural effusions, the trachea contained a large amount of frothy fluid , non-specific pulmonary congestion and edema. The liver was congested, and there was focal reddening of the lining of the ascending colon, Microscopy revealed very occasional contraction bands in the myocardium and some scattered mixed inflammatory cells in the liver sinusoids Postmortem toxicological findings: Arsenic levels in: Blood, 7.0 mmol/L (reference range<0.135µmol/L); Urine (64.5 µmol/L) (reference range: <0.25 µmol/L); Hair (71 µmol/L) | [19] |
| Mercury | A 36-year-old man | Inhalation | Cigarettes contam inated with elementary mercury | His acquaintance | Sensory abnormality in the mouth, headache, appetite loss, shivering flu-like symptoms | Survived | Mercury levels (µg/L): Blood : 99, Urine: 23 | [20] |
| Mercury | A 34-year-old man | Intravenous injection | 40g mercury extracted from 40 thermo meters through the veins at left elbow and back of right foot | His girlfriend | Pyrexia, chill, fatigue, anorexia, dyspnea, sweatiness, productive cough, body aches, and a right dorsal foot pain. Enlarged lymph nodes in the right groin, tumidness, and necrosis in dorsal part of the right foot with purulent fluid, ecchymosis on the anterior tibia of right lower limb, and macular erythematous rash over the body. | Survived | Urinary mercury concentration: 4828mg/L. | [21] |
| Mercury | A 53-year-old woman | Oral | Unknown | An offender | Abdominal pain, nausea, vomiting, diarrhoea, kidney failure, circulatory-respiratory insufficiency | Died | Postmortem toxicological findings: Content of mercury (ng/g) in tissues and internal organs from exhumed cadavers (6 years after death): Small intestine: 1516; Large intestine: 487; Liver: 1201; Heart muscle: 1023; Hair: 227) | [22] |
| Barium (as Barium Chloride) | A middle- aged man | Oral | Table salt | An offender | Vomiting, diarrhea, profuse sweating, abdominal cramps, weakness of the limbs. hypokalemia | Died | Postmortem histopathological findings: Heart: the main coronaries had grade 2 to 4 stenosis and no evidence of recent infarct; Lungs: edematous and congested. Brain: edematous with hippocampal and tonsillar herniation. Miicroscopic findings: fatty changes of the liver; scattered subendocardial hemorrhage in the cardiac left ventricular wall nearest the septum; the kidney showed sloughing of epithelial cells into the proximal tubules, hyaline droplet changes and amorphous, flocculent foamy materials in the tubules’walls; and the small intestine (mainly duodenum) had numerous petechiae on the luminal surface. Postmortem toxicological Findings: Barium concentrations (ppm) as follows: Brain, 24.03; Blood, 20.10; Stomach content, 24.22; Lung, 24.09; Kidney, 24.33; Spleen, 23.56; Liver, 27.08 | [23] |
| Polonium-210 | Alexander Litvinenko (43 years old ) | Oral | Coffee | Former KGB agents | Abdominal pain, vomiting, diarrhea, epigastric tenderness, neutropenia, pancytopenia, Aplastic anemia, Alopecia, severe mucositis,, fever, Generalized erythema, Abnormal ECG, Renal and hepatic failure, multi organ failure, cardiorespiratory arrest | Died | Postmortem histopathlogical findings: Gross macroscopic findings: presence of blood-tinged fibrinous pericarditis, a pleural effusion associated with bilateral congestion of the lungs, gross ascites,, generalized tissue autolysis of most organs, although the brain looked normal. Microscopy of the internal organs was not done. Gamma-ray spectrometry findings: Polonium-210 activity (as Mega Becquerel(MBq) per gram of tissue): Liver (30MBq/ g),Kidney (49 MBq/g), Bile (13 MBq/g), Spleen (9.9 MBq/g), Heart (2.5 MBq/g), Skin (1.8 MBq/g), Lung (3.5 MBq/g) was consistent with intake by ingestion. | [24] |
| Polonium-210 | Yasser Arafat(75 years old) | Oral | Meal | Unknown Person | Severe nausea, vomiting, and abdominal pain, watery diarrhea, disseminated intravascular coagulation, thrombocytopenia, bone marrow hemophagocytosis, cholestatic jaundice, acute renal failure, cerebral hemorrhage, cerebral herniation | Died | Abnormal levels of polonium-210 in some of Arafat’s belongings that were worn during his final hospital stay and which were stained with biological fluids. Postmortem Radioanalytical results on the exhumation of Arafat’s remains in 2012: Significantly higher (up to 20 times) activities of 210Po and lead-210 were found in the ribs, iliac crest (48-904 mBq/g Ca) and sternum specimens compared to reference samples. | [25] |
| Cyanide | A 59 year old man | Injection (Subcutaneous) | - | An offender | Rapid breathing, respiratory depression, bitter almond odor | Died | A single puncture wound, 1 mm in diameter and 2 cm deep on the anterior abdominal wall, situated 7 cm above and 5.5 cm to the right of the umbilicus, surrounded by a circular black discoloration of the skin 1 cm in diameter. The blood was bright red in color. A “bitter almond” odour was detected around the body. Congestion of the internal organs. Postmortem toxicological Analysis: Analysis of the contents of the syringe and a blood sample from the deceased confirmed the presence of cyanide (no quantitative analysis has been done). | [26] |
| Methanol | A 21-month- old male toddler | Oral | Apple cider drink | Stepmother | Lethargy, dyspenea | Died | Autopsy findings: The external examination showed evidence of recent small abrasions and the unusual finding of a probable needle puncture site with a 6- mm surrounding hematoma on the anterior right thigh. The lungs were congested, The stomach contained approximately 10 mL of dark brown fluid with no identifiable food particles. Postmortem toxicological findings :Methanol levels (as w/v%) in: Heart blood: 0.214; Venous blood: 0.231; Vitreous humor: 0.276; Urine: 0.306; Liver: 0126; Bile: 0.252; Gastric content: 0.256 Formic acid concentrations (w/v%): Heart blood: 0.100; Urine: 0.635; Liver: 0.053 Toxicological findings in Sippy cup experiments: Methanol: 0.670% (w/v) | [27] |
| Methane gas | A 53-year-old woman | Inhalation | - | Her husband | - | Died | Congestion of vital organs. | [28] |
| Paraquat (Herbicide) | A 20-year-old woman | Oral | Forcible ingestion after ligature strangulation | Her ex- boyfriend | Semiconscious, burning sensation in the mouth and noticed a greenish fluid and stains around face, respiratory edema and failure | Died | Autopsy findings: Subconjunctival ecchymosis in both eyes and a healing ligature mark around the middle of the neck, The hyoid bone and the laryngeal skeleton were intact. No significant lesions were present in the underlying soft tissues apart from the mild fibrocellular inflammatory reaction. The brain was edematous and cyanosed. The tongue was ulcerated and covered with whitish-yellow slough. The esophageal mucosa was eroded and peeling off. The gastric mucosa appeared swollen. The liver showed extensive fatty changes with areas of focal necrosis. Both kidneys were pale and swollen, while the lungs were heavy, firm, emphysematous, and rubbery in consistency. No postmortem toxicology was performed. However, the paraquat was identified the victim’s vomitus on admission using a spot test. | [29] |
| Paraquat | Two victims (An 81-year- old woman as mother and a man as her son) | Oral | Spicy meal and adulterated drink | Son’s wife | Mother: Sore throat and difficulty swallowing for about 2 weeks, fever, severe dyspnea due to pneumonia in both lungs. Son: Chronically suffering from interstitial lung disease (diagnosed as bronchiolitis obliterans organizing pneumonia) of unknown cause. | Died | Autopsy findings (only in one case when exhumed) On external examination, the body was severely decomposed. On internal examination, internal organs were decomposed and the brain showed liquefactive necrosis. Coronary arteries revealed mild to moderate atherosclerosis. It was difficult to determine whether pneumonia had been in both lungs or not due to postmortem putrefaction. There were some punctuate hemorrhage on the gastric mucosa, and there were no gastric contents. No fracture was identified in the body. Toxicological analysis findings: The paraquat concentrations: 1.5 ng/g (stomach), 1.3 ng/g (liver), 5.5 ng/g (kidney), 4.2 ng/g (spleen), 0.8 ng/g (lung), and 2.3 ng/g (bone marrow) | [30] |
| Paraquat | A 37-year-old man | Oral | White wine | His wife | Intermittent vomiting, which he attributed to being intoxicated. The man was admitted to the hospital for treatment 3 days later. The man did not receive effective treatment and died of respiratory failure 22 days later | Died | Postmortem toxicological analysis: Kidney (1.31 ug/g), liver (0.62 ug/g), urine (0.91 ug/ml), lung (0.39 ug/g), muscle (0.35 ug/g), bile (0.32 ug/ml), heart (0.28 ug/g), brain (0.22 ug/g), pancreas (0.22 ug/g), spleen (0.18 ug/g), cardiac blood (0.15 ug/ ml), cerebrospinal fluid (0.14 ug/ml), pericardial effusion (0.12 ug/ml), pleural effusion (0.09 ug/ml), peripheral blood (0.08 ug/ml), and vitreous humor (0.06 ug/ml). The highest concentration of paraquat was detected in the kidney followed by the urine in all tissues and body fluids. | [31] |
| Paraquat | A 58-year-old man | Oral and dermal exposure simulta neously | paraquat- mixed medicine and wearing paraquat- soaked underwear | His wife | Dyspnea, cough, and scrotal dermatitis and died of respiratory failure 24 days after the initial exposure to paraquat. | Died | Postmortem toxicological analysis: The concentration of paraquat in postmortem specimens from high to low is lung (0.49 μg/g), brain (0.32 μg/g), kidney (0.24 μg/g), liver (0.20 μg/g), cardiac blood (0.11 μg/mL), | [32] |
| Brodifacoum (Rodenticide) | A 50-year-old man | Oral | Meal | Unknown | Sudden massive nasal bleeding, | Survived | Brodifacum concentration in blood sample was 150 ng/mL | [33] |
| Carbofuran (A carbamat pesticide) | Three cases from a family (A 3.5 years old boy, his sister (8 years) and the mother of the children) | Oral | A drink | one of their relatives | burning sensation, vomiting, bitter taste and irritation in the mouth | One fatality (The boy died in the hospital 3 h later while the sister and mother recovered) | Postmortem toxicological analysis: Carbofuran levels were in: Blood (1.5 µg/mL); and Suspected drink (2.1 mg/mL) | [34] |
| Carbofuran | Two cases (A 10- year old girl and her mother). | Oral | A soft drink | Her father | Bitter taste, vomiting, lethargy | One fatality (girl died and mother survived) | Postmortem toxicological analysis: Carbofuran levels were in: Stomach content (300 µg/g); and Suspected drink (3.8 mg/mL) | [34] |
| Organchlorine compound | A 52-year-old man | Injection (Intra peritoneal) | Forcible injections | His business rivals | Not reported | Died | Autopsy findings: Rigor mortis was present all over the body and lividity appeared over the back, which was fixed. No sign of decomposition was seen. The abdomen was distended. Two needle puncture wounds were present over the abdomen. The brain and lungs were edematous and congested. The stomach was congested with hemorrhagic spots only at the antrum and fundus areas. No particular smell was detected. Other visceral organs had no visible abnormality. Toxicological analysis results: The toxicological examination report showed the presence of ‘organochloro’ insecticide in all the viscera and needle puncture wound sites. | [35] |
| Mixture of Chlorpyrifos (an organ ophosphate pesticide) and Cyper methrin (a pyrethroid insecticide) | A 40- year old woman | Oral | Cake | Her husband | Not reported | Survived | Chemical analysis of cake sample by thin layer chromatography (TLC) and Gas chromatography- mass spectroscopy (GC-MS) revealed chlorpyrifos (organophosphorus insecticide) and cypermethrin, (pyrethroid insecticide). | [36] |
| Heroin | A 10-month- ol girl infant | Injection | - | Her father | Found dead in her room | Died | Autopsy findings: Rigor mortis was present and lividity was fully developed posteriorly and in a patchy distribution anteriorly. There was a single needle puncture present in the left antecubital fossa. On microscopic examination, findings were unremarkable apart from broad areas of alveolar edema and generalized vascular congestion on lung histology. Postmortem toxicology findings: Cardiac blood: (Morphine 1092 ng/mL, codeine 74 ng/mL, 6-monoacetyl-morphine 359 ng/mL); Liver tissue (morphine 803 ng/g, codeine 54 ng/g); Vitreous humor (morphine 181 ng/m) | [37] |
| Methadone | A 32-month- old boy infant | Oral | Meal | His father | He was found irresponsive in an adult bed at home by his parents | Died | Autopsy findings: External examination did not reveal anything remarkable. The liver weighted 415 g and was relatively congested. No identifiable pill components or fragments were found in the stomach contents or upper gastrointestinal tract. The heart weighted 85 g and showed a left ventricular hypertrophy. The examination of the aorta and the pulmonary artery revealed a coarctation of the aorta with a focal stenosis (0.6 cm in length) located at the junction of the distal aortic arch and the descending aorta, Histology confirmed the existence of a tubular hypoplasia of the aortic arch. Postmortem toxicology findings : Methadone concentrations (mg/L) were in: Femoral blood (0.633); Urine (5.25); Bile (2.64); Gastric content (1.08); Hair (0-3 cm)(3.11 ng/mg); Hair (4-6 cm) (4.91 ng/mg) | [38] |
Table 1: Review of the Literatures on Homicidal Poisoning Cases.
| Succinylcholine | A 28-year-old man | Injection | A syringe- like dart ejected by a compound crossbow | A man | He was found dead in his car | Died | Autopsy findings: Dark red-purplish liver mortis was evident on his back. His lips and nail beds were cyanotic, and his conjunctivae were congestive with petechial hemorrhages. There was a pinhole located on his back, 5 cm below the inferior angle of scapula and 2 cm left of the spinal column without any external hemorrhage. Extensive subcutaneous and muscular hemorrhages around the pinhole were found after the skin was incised. The wound track was 1.5 cm in depth, passed through the trapezius and terminated in the latissimus dorsi. Heart weighted 280 g, with multiple subepicardial petechial hemorrhages. The lungs were obviously congestive and edematous, accompanying the multiple subpleural petechial hemorrhages. The brain was swollen, weighted 1400 g, without any cerebral contusion. Toxicological findings: The concentration of Succinylcholine in the blood and the solution in the same unused poisonous dart (found in the suspect’s house) were determined to be 23 mg/ml and 1000 mg/ml. | [39] |
|---|---|---|---|---|---|---|---|---|
| Insulin | A 10-year-old girl | Injection | empty syringes and a FIASP ® Flextouch pen | Her mother | Not remarkable | Survived | Toxicology analysis: Aspart insulin tested positive at 2.4 ng/mL in the blood specimens of the child. The substance contained in the syringes and pen also corresponded to aspart insulin. | [40] |
| Cyamemazine with other drugs including Benzodiazepines Z-drugs, Neuroleptics, Antidepressants and Analgesics | A 62-year-old man | Oral | Fruit salad | His wife and son | The patient had six months with neurological disturbances of undetermined cause characterized by episodes of decreased vigilance and even coma, inhalation pneumopathy with acute respiratory distress syndrome and septic shock. | Survived | Toxicological analysis findings: Drug used for repeated attempted homicidal poisoning in biological and non-biological samples: Plasma (Cyamemazine 140µg/L;nordiazepam <100 µg/L) Hair samples: Midazolam,Clonazepam,7- aminoclonazepam,Alprazolam, Bromazepam, Nordiazepam, Oxazepam, Zolpidem, Cyamemazine Haloperidol, Hydroxyzine, Cetirizine, Amitriptyline, Venlafaxine Non-biological samples (meal, syringe and dropper): Cyamemazine, Alprazolam, Bromazepam and Paracetamol | [41] |
| Cyamemazine with Benzodiazepines and Antidepressants | Two cases (A one-month- old and a 4.5-year old girls) | Oral | Drinkable form of a pharma ceutical by pouring the content of bottle into the feeding- bottle of the children. | Her mother | Not reported | Died | Postmortem toxicological analysis: Cyamemazine (3.4 mg/mL in the peripheral blood) in 4.5-year old girl. In second case: Amitriptyline: Liver (29.8 µg/g); Cerebrospinal fluid (4.4 µg/mL), Hair (1811 pg/mg) Nortriptyline: Liver (3.6 µg/g); Cerebrospinal fluid (0.6 µg/mL), Hair (53 pg/mg) Bromazepam: Hair (740 pg/mg) | [42] |
| Amitriptyline | A 6-month- old baby girl | Oral | Not determined | Her parents | Coma with mydriasis, respiratory arrest, generalized tonic–clonic seizure, fast osteotendinous reflexes, bilateral retinal hemorrhage, cerebral IRM revealed subdural hematomas and cortical laminar necrosis | Survived | Toxicological analysis findings: Amitriptyline and its active metabolite nortriptyline were quantified in blood at 99.4 mg/L and 154 mg/L, respectively. Segmental hair analysis showed the presence of amitriptyline and nortriptyline at 6.89 and 8.14 ng/ mg, respectively. | [43] |
| A mix of psychotropic medications | 13 cases (Age range: 83-95 years old) | Oral | Liquid formulation | A young nursing assistant | Malaise and coma | 10 cases were killed and 3 cases survived | Cyamemazine, mirtazapine, loxapine, tiapride, and risperidone hair concentrations were 6–17,458 pg/ mg, 74–1271 pg/mg, 9–1346 pg/mg, 13–148 pg/mg, and 3–5 pg/mg, respectively. Cyamemazine bone marrow concentrations were 229 and 681 ng/g and 152–717 ng/mL in blood. | [44] |
| Anesthetic drugs(propofol, midazolam, vecuronium) | A 41-year-old man | Injection (intravenous) | - | An offender | The man with diarrhea was found dead within 5 minutes after transfusion of levofloxacin, gentamicin and clindamycin in the hospital. Cyanosis and dyspnea occurred soon after withdrawal of the needle, then respiratory and cardiac arrested afterward. | Died | Autopsy findings:multifocal emphysema within the surface of both lungs. Pulmonary edema, compensatory emphysema, lymphocytes and monocytes infiltration in bronchial walls, focal thickening and fibrosis of alveolar septum and congested capillaries in the alveolar walls, but eosinophilic granulocyte infiltration was not involved. Additionally, congestion of all organs was noticed as well. The results of toxicological analysis showed three anesthetic drugs (propofol, midazolam, vecuronium) in the deceased’s Blood (0.517, 0.098, 0.10 µg/mL, respectively), Urine (ND, 0.012, 012µg/mL, respectively), Liver(3.983, 0.31 and 0.25 µg/mL, respectively) and Kidney (0.765, 0.61 and 0.39 µg/ml, respectively). | [45] |
| Heroin and Estazolam | A 40-year-old woman | Oral and injection | Adulterated milk | An offender | She was deceived into drinking a cup of milk that had 72 tablets of estazolam (2mg/tablet) dissolved in, and then being injected heroin aqueous solution on the right deltoid region by the criminal. | Died | Pinpoint pupils and a new injection site on the right deltoid region were found. Multiple patchy hemorrhages and considerable amounts of foreign amorphous substance with yellow appearance at the injection site. Some double refracting crystals with the forms of Maltese cross, acicular, rhomb or irregular were found by polarizing microscope, which may result from the diluent in heroin such as starch. Toxicological qualitative analysis showed the presence of estazolam and morphine in blood and urine, and heroin in the injector left at scene. | [46] |
| Atropine | A 51-year-old man | Oral | Atropine sulfate eye drops | An offender | The man was found in the boot of his car, which had been left in a public car park. | Died | Atropine was detected and quantified in the biologic fluids and the hair. The atropine concentrations were 887 ng/mL in the cardiac blood, 489 ng/mL in the peripheral blood, 6693 ng/mL in the gastric contents (1.1 μg), 6753 ng/mL in the urine, and 2290 pg/mg in the hair. | [47] |
| Tetrodotoxin (TTX) | A 29-year-old man | Injection (Subcu taneous) | - | Two strange men | Gasping and rapid death | Died | Autopsy findings: A patchy bleeding was observed in the upper lip mucosa, as well as cyanosis of the mouth, lips, fingers and toenails bed.A needle hole was found at middle of left buttock with subcutaneous bleeding around the hole. After the tissues surrounding the hole was squeezed, a small amount of blood flowed out. Dissection of the buttock showed bleeding in the subcutaneous tissue at the pinhole in the middle of the left buttock. A 3 cm needle stalk was found in the subcutaneous tissue, and no obvious bleeding was observed in the muscle. Remarkable histopathological examination findings included subcutaneous focal hemorrhages at left buttock, pulmonary interstitial blood vessels dilated and filled up, alveolar spaces expanded and filled with massive pink edematous fluid or erythrocyte. In the myocardium, myocardial cells showed “wave-like” changes, mild adipocyte infiltration, the vessel of atrioventricular node mild thickened. In the liver, we observed massive hepatocyte steatosis, bile duct epithelium autolysis. TTX concentrations in cardiac blood was 1.26 ng/ml | [48] |
| Gloriosa superba seeds (contain Colchicine) | A 27-year-old man | Oral | Drinking coriander tea | Victim’s sister- in-law | Profuse vomiting, diarrhea , shock, respiratory distress, mild renal impairment, thrombocytopenia, massive generalized alopecia | Survived | Detection of Gloriosa seeds by the family members because they had seeds at home and the victim’s sister-in-law who had made the herbal tea went missing from home. They were able to identify Gloriosa seeds, which looked similar to coriander, in the pot. | [49] |
| Snake Bite | Three victims (They were 9-, 6-, and 4-years old. girls) | Forced envenomation | Egyptian cobra | Victims’ father | Not reported | Died | Autopsy findings: In the eldest child(9 years old): Cyanosed finger tips, lips and tongue. Multiple fang marks was noticed in the lower part of right leg. They were five pairs of marks with almost fixed distance between paired one. Sometimes, the two fang marks were asymmetrical, indicating the father forced the snake fang into the skin. Superficial penetrating fang marks were seen indicating hand movement of the father during fang insertion in the skin. It was surrounded by erythema and little swelling. On making superficial incision, reddish fluid oozed. Intense congestion of all the internal organs. The second female child was 6 years old. Hypostasis, rigor mortis, cyanosis, and internal organ congestion. There were two pairs of fang marks on the left leg. Each pair was symmetrical. These marks were surrounded by erythema and slight swelling. Superficial fang marks were also noticed. The youngest child was 4 years old: She has multiple fang marks close to each other with more erythema in the right leg. | [50] |
| VX (A nerve agent) | Kim Jong- nam (45-year old) | Dermal and Inhalation | By a poisoned hand kerchief to his face | The killing was carried out by two women | Trembling hands, hyperhidrosis, weakness symptoms of cholinergic Syndrome, respiratory failure, The death occurred 20 min after the attack. | Died | The autopsy report is probably not available to the public. | [3] |
| Novichok (A-234 agent) | Two cases Sergei Skripal (67 years old) and his daughter Yulia (39 years old) | Dermal contact | Spray the Novichok agent on the door knob and front door of Skripal’s home | Two agents of Russian Military Intelligence service (GRU) | Coma and Foam was coming out of Yulia’s mouth. On admission to hospital, the condition of both was described as critical. | Survived | the Organization for the Prohibition of Chemical Weapons (OPCW) experts visited the locations where the victims were exposed and collected environmental samples. The OPCW team also took biomedical samples from the exposed individuals. The results of analysis by the OPCW designated laboratories confirmed the findings made by the Defence Science and Technology Laboratory (DSTL), Porton Down, relating to the identity of the agent. | [51] |
| Novichok | Alexei Navalny (44- year old) | Dermal | His underwear left in his hotel room | Russian FSB agents | He was suddenly became confused and began to sweat heavily on a domestic flight in Russia approximately 10 min after departure; he vomited, collapsed, and lost consciousness. comatose with hypersalivation, increased diaphoresis, respiratory failure, myoclonic status, disturbed carbohydrate metabolism, electrolyte disorders, and metabolic encephalopathy. | Survived | Severe poisoning with a cholinesterase inhibitor was subsequently diagnosed. the German Government announced that a laboratory of the German armed forces designated by the Organization for the Prohibition of Chemical Weapons (OPCW) had identified an organophosphorus nerve agent from the novichok group in blood samples collected immediately after the patient’s admission to hospital. | [52] |
Table 2: Review of the Literatures on Homicidal Poisoning Cases.
In this study, most of the killers were a members of the victim’s family [20 (45.45%) people]. Others were criminals [19 (43.20%) people]; victim’s girl- or boy- friend [2 (4.54%) people], colleagues [2 (4.54%) people] and caregiver [1(2.27%) person].
In this review, we observed according to the numbers of victims with homicidal intent, arsenic had the most affected cases (17.28%); following, thallium (13.58%), paraquat (6.18%) and carbofuran (6.18%).
Also, administration of pharmaceutical agents as a tool in homicidal poisoning were common and reported in 9 articles with in total 22 poisoned cases resulted 16 (72.2%) fatal cases. The common drugs used in homicidal intent poisonings were included as the combination of benzodiazepines, antipsychotics, antidepressants, analgesics, antihistamines and methadone, succinylcholine, atropine, Insulin, general anesthetics and muscular relaxants.
A polydrug pattern in the homicidal poisonings was observed in 17 (20.98%) victims including benzodiazepines Z-drugs, neuroleptics, antidepressants, analgesics and anesthetic drugs (propofol, midazolam, vecuronium). In addition, the most frequent reported poisons used in homicidal poisonings were pharmaceutical agents (combination of antipsychotics with benzodiazepines and antidepressants drugs) (3 reports), paraquat (4 reports), mercury (3 reports), thallium (3 reports), carbofuran (2 reports), heroin (2 reports), Polonium-210 and Novichock (2 reports from each other).
The frequency of the used poisons and drugs in the homicidal poisonings according to number of victims and number of the reported episodes have been demonstrated in Table 2.
| Name of Poison/Drug | Number of victims (Total cases=81) | Frequency (%) | Number of reported episodes |
|---|---|---|---|
| Polydrug poisoning including Benzodiazepines Z-drugs, Neuroleptics, Antidepressants and Analgesics | 16 | 19.75 | 3 |
| Arsenic | 14 | 17.28 | 2 |
| Thallium | 11 | 13.58 | 3 |
| Paraquat | 5 | 6.18 | 4 |
| Carbofuran | 5 | 6.18 | 2 |
| Mercury | 3 | 3.7 | 3 |
| Snake bite | 3 | 3.7 | 1 |
| Heroin | 2 | 2.47 | 2 |
| Polonium-210 | 2 | 2.47 | 2 |
| Novichock (Organophosphorus nerve agent) | 2 | 2.47 | 2 |
| Strychnine | 1 | 1.23 | 1 |
| Barium | 1 | 1.23 | 1 |
| Cyanide | 1 | 1.23 | 1 |
| Methanol | 1 | 1.23 | 1 |
| Methane gas | 1 | 1.23 | 1 |
| Brodifacoum | 1 | 1.23 | 1 |
| Methadone | 1 | 1.23 | 1 |
| Succinylcholine | 1 | 1.23 | 1 |
| Insulin | 1 | 1.23 | 1 |
| Atropine | 1 | 1.23 | 1 |
| Tetrodotoxin (TTX) | 1 | 1.23 | 1 |
| Herbal toxin (Colchicine) | 1 | 1.23 | 1 |
| Amitriptyline | 1 | 1.23 | 1 |
| Anesthetic drugs (Propofol, Midazolam, Vecuronium) | 1 | 1.23 | 1 |
| Mixture of Chlorpyrifos and Cypermethrin | 1 | 1.23 | 1 |
| Organochlorine compound | 1 | 1.23 | 1 |
| VX (Organophosphorus nerve agent) | 1 | 1.23 | 1 |
Table 3: The Frequency of the Used Poisons and Drugs in the Homicidal Poisonings According to Number of Victims and Reported Epis
Discussion
The result of this study showed that 81 cases with homicidal poisoning reported in the period of the study. The majority of cases were female and the common age of the victims were equal or less than 50-year old. These findings are similar to previous studies. For example, in Sweden during 1992-2019, female victims in homicidal poisoning cases was dominant when compared to males [3]. In previous study, female cases were reported among infant and children while male cases were reported among older age groups [10].
In the study, 45.45% of known offenders were family members. This finding is in concordance with many of previous studies on homicidal poisoning [3, 5, 6]. In the present study, the case fatality rate in the victims were 58.02% and drugs were used in more than 20% of cases.
Drugs as a Tool Used in Homicidal Poisoning
A notable issue in this study, co-administration and a polydrug pattern including benzodiazepines (midazolam, clonazepam, alprazolam, bromazepam, oxazepam), Z-drugs (zolpidem), antipsychotics (cyamemazine, haloperidol, risperidone, tiapride), antihistamines (Hydroxyzine, cetirizine), antidepressants (amitriptyline, venlafaxine) and analgesics (paracetamol) as a cocktail for homicidal poisoning in elder victims.
Antipsychotics are commonly used to treat schizophrenia, bipolar disorders, depression, and other conditions. Antipsychotics are classified as typical first- generation or atypical second-generation drugs [53]. They have special warnings for use in the elderly patients with dementia-related psychosis that includes an increased risk for fatalities and cerebrovascular accidents [53]. Also, sudden cardiac death has become a significant clinical concern when prescribing antipsychotic drugs, especially to elder patients with dementia. Actually, patients treated with both the first- and second-generation versions and current use of tricyclic antidepressant and benzodiazepines experienced an increased incidence of fatalities. Co-morbidity conditions, especially heart disease, in the administration of antipsychotics drugs have been associated with sudden cardiac death [54]. From this view, administration of cocktail of these drugs as a homicidal tool by offenders should be considered especially in elder patients nursing house in suspicious and undetermined death. In reviewed cases intermittent episodes of malaise, decreased of vigilance, acute respiratory distress and coma have been reported as clinical presentations of the victims due to covert oral administration of antipsychotics plus other central depressant medicines via meal in the elder patients.
Heavy Metals Used in Homicidal Poisoning
In our study, arsenic had one reported homicidal intent of poisoning but it had high number of poisoned victims in this episode. This report demonstrates an outbreak of apparent food-borne illness following a church gathering. Gastrointestinal symptoms among church attendees were initially attributed to consumption of leftover sandwiches that had been served the previous day. However, a rapid epidemiological and laboratory assessment revealed the etiology of illness was not food-borne in origin. It was due to a criminal act via deliberate arsenic contamination of the brewed coffee by one of the church members [18].
Arsenic, a metalloid, is one of the oldest poisons known to humans. Historically, its applications were including pesticides (insecticides, fungicides, herbicides), ceramic enamels, preservatives, glass manufacturing, firework, medicinal use (antibacterial, dermatological and hematological agents), and paint. Acute arsenic poisoning is rare in the recent years. Arsenic compounds are organic arsenicals and pentavalent or trivalent inorganic arsenic. The trivalent derivatives are more toxic than pentavalent forms [55, 56]. Arsenic-related deaths due to acute poisoning occur as a result of accidental, intentional (homicides and suicides) poisoning [55, 56]. Clinical presentations of acute arsenic poisoning are usually apparent when the poison is administered orally, inhalation or by injection [54]. Clinical signs and symptoms of acute arsenic poisoning are predominantly gastrointestinal, cardiovascular, neurologic, and renal [56]. Acute arsenic poisoning is associated initially with nausea, vomiting, abdominal pain, and severe diarrhea. Encephalopathy and peripheral neuropathy are reported [57]. Acute arsenic poisoning may result in death. A garlic- like odor on the breath or in perspiration is suggestive of arsenic poisoning. Death from arsenic is generally caused by circulatory collapse, associated with intense gastroenteritis, capillary injury that produces vasodilatation, transudation of plasma, and shock and multiorgan failure [56]. Arsenic toxicity induces by inhibition of many enzymes, especially those involved in cellular energy pathways and DNA synthesis and repair [57].
Thallium is another common poison used in the homicidal poisoning in this study. In unique case a thallium toxicosis in Italy in 2017 due to deliberate adulteration of an herbal infusion with thallium sulphate by the grandson of the victims occurred in eight members of a family, three of them died because of the poisoning [17]. Thallium is a toxic heavy metal used in concrete, optical lenses, dyeing and pigments, jewelry, electronic, for green fireworks and military industries. Thallium in the form of water soluble salts (sulfate, acetate and carbonate), with a concentration of 2% as a rat poison killer. Thallium is colorless, odorless, water- soluble, and tasteless, therefore, it often passes unnoticed. It is extremely toxic, and the lethal dose is estimated to be 10–15 mg/kg [58]. The diagnosis of criminal thallium poisoning in general clinical practice is quite hard and may be misdiagnosed due to the wide range of symptoms of the poisoning with other common diseases [17, 58]. The acute thallium poisoning is divided into three phases.
The first phase is the intravascular distribution and lasts approximately for the first 4 h. Then, the poison is distributed in the central nervous system and this second phase lasts for 48 h. The third phase is the elimination phase mainly through the gastrointestinal and renal system which begins 24 h later.
Gastrointestinal, neurological, and dermatological symptoms are the main symptoms in acute thallium poisoning [58, 59]. The first symptoms of poisoning, within the first 48 hours from the poisoning is include gastrointestinal symptoms (abdominal pain, cramps, nausea, vomiting, fever and constipation), acute cardiotoxic effects, hematologic manifestations (anemia and thrombocytopenia), followed by neurotoxicological symptoms (tremor, acute and progressive paralysis of the limbs, coma) [59]. Within 3-4 weeks, usually, alopecia appears mainly to the eyebrows and the auxiliary area. The death can occur due to cardio-circulatory failure or multi-organ failure [58, 59]. Thallium acts in a way similar to potassium but with an affinity 10 times higher, replacing this latter substance in a series of enzymatic complexes, especially mitochondrial, other mechanisms are suspected of having an important role in these processes as the already cited oxidative stress, the interruption of the potassium- regulated homeostasis and of the glutathione metabolism [57, 58, 59].
Elemental mercury and its salts was a common cause of homicidal poisoning in the present study.
Mercury is a toxic heavy metal has three forms including metallic, inorganic, and organic compounds.
Metallic mercury is volatile and highly lipophilic [21, 60] Metallic mercury poisoning is usually caused through inhalation of its vapor [21]. Systemic symptoms in acute mercury poisoning are headache, pyrexia, chill, fatigue, sore throat, dizzy, itching, skin rash, body aches, and waist soreness, soft tissue necrosis, respiratory symptoms (chest pain, cough, bloody sputum, sweatiness, hemoptysis, dyspnea). In addition, gastrointestinal presentations (abdominal pain, nausea, vomiting, anorexia, diarrhea, oral ulcers and gingival bleeding), neurological deficits (tremors, cerebellar dysfunction, generalized tonic-clonic seizures, peripheral axonopathy and mental abnormalities) and liver and kidney damage have been reported in acute exposure of metallic mercury [21, 60].
Metallic mercury poisoning through intravenous administration is quite rare, especially for homicide [21]. Injection of metallic mercury can lead to a rapid increase of circular mercury in a short time, and finally distributes throughout the body. It can be easily misdiagnosed when no history of mercury exposure is available, especially in homicide cases [21].
Pesticides Used in Homicidal Poisoning
Pesticides defined as a chemical or biological agents used to repel or kill the agricultural and veterinary pests. Pesticides are potent and lethal toxic substances that are also being infamously used for homicidal intent due to their easy availability and rapid action. In this review, organophosphates and rodenticides were the most commonly used pesticides, and ingestion was the most common route of administration; however, other modes of administration, such as through intraperitoneal injection, were also reported. The regulations for the production, distribution, sale, and use of pesticides and sever monitoring programs can help control the prevalence of these type of poisoning [61]. In the present study, pesticides including paraquat (N,N′-dimethyl- 4,4′-bipyridinium dichloride; a herbicide), carbofuran (a carbamate insecticide and nematocide), chlorpyrifos (an organophosphate pesticide) and cypermethrin (a synthetic pyrethroid used as an insecticide), brodifacoum (is a highly lethal 4-hydroxycoumarin vitamin K antagonist anticoagulant poison, a rodenticide), strychnine (an alkaloid and used as a rodenticide) were the reported poisons used in homicidal poisoning mainly in countries like as India, Sri Lanka and South Korea. This findings are similar to previous studies especially from developing countries which public availability to these poisons is easer [10, 29, 30, 31, 32, 33].
Poisons Used in the Recent Political Homicidal Poisoning
Poisons used in political homicidal poisoning in famous cases according to timeline and place of incident were ricin (Georgi Markov, 11 September 1978, London, UK), fentanyl (Khaled Mashal, 25 September 1997, Amman, Jordan),TCDD dioxin (Viktor Andriyovych Yushchenko, 5 August 2004, Kyiv, Ukraine), polonium-210 (210Po) radioisotope (Yasser Arafat, 11 November 2004, Percy, France and Alexander Litvinenko, 1 November 2006, London, UK), VX (Kim Jong- Nam, 13 February 2017, Kuala Lumpur, Malaysia), and Novichock (Sergei Skripal and his daughter Yulia, 4 March 2018, London, UK, and Alexei Navalny, 20 August 2020, Tomsk, Russia) [3, 62, 63]. As a notable fact, contemporary poisons, are based on the use of synthetic substances from the organophosphorus-based nerve agents and radioactive isotopes instead of biotoxins. Some of these poisons (especially, polonium-210 and ricin), resulted initially in a clinical presentations that was misdiagnosed with infections, chronic disease or chemicals poisoning like as heavy metals and chemotherapeutic agents or radiations [3, 24].
Polonium-210 (210Po) is an isotope of Polonium and a natural radioactive element that it undergoes alpha decay to stable lead-206, with occasional excitation in the nucleus and emission of 803keV gamma rays. Its half-life is 138 days and its biological half-life is human body approximately 30-50 days [24, 25, 63]. 210Po is used in various industrial processes and as a lightweight heat source to power thermoelectric cells in satellites. Also, Polonium-210 was used in initiators for atomic bombs through the alpha and neutron reaction with beryllium. 210Po is extremely toxic as a radiotoxic agent for man. One microgram of 210Po being more than enough to kill the average adult, it is 250,000 fold more toxic than hydrogen cyanide by weight [63]. Lethal dose 50 (LD50) of 210Po considered as 50ng (for oral route) and 10ng (in inhalation route). This is a consequence of its ionizing alpha radiation, as high energy alpha particles are especially damaging to organic tissues. However, 210Po does not pose a radiation hazard when contained outside the body. The alpha particles it produces cannot penetrate the outer layer of dead skin cells [63].
Intake of 210Po occurs primarily through contaminated food, water or air, as well as through open wounds. It forms water-soluble, colorless salts that are readily absorbed across biological membranes. Post ingestion, 210Po concentrates in red blood cells and soft tissues (with highest concentration in the liver, spleen, bone marrow, kidneys, gonads and skin). 210Po is excreted in urine, bile, sweat, and possibly in breath and is also deposited in hair. After ingestion, unabsorbed 210Po is present in the faces [64, 65].
However, It is not widely available and used in political homicidal poisoning by governmental secret security and intelligence agencies for assassination and terroristic acts of political activists and leaders. If the absorbed dose is sufficiently large, polonium-210 can cause Acute Radiation Syndrome (ARS). Clinical presentations after oral intake of 210Po are gastrointestinal symptoms such as nausea, vomiting, anorexia, abdominal cramps and watery and bloody diarrhea. Additional symptoms include bleeding, alopecia, lymphopenia (especially without elevated temperature), thrombocytopenia and leukocytes (occurring after a few days or weeks after gastrointestinal symptoms). Followed by a latent phase during which there is some clinical improvement. Subsequently, the characteristic bone marrow suppression, gastrointestinal or cardiovascular/ central nervous system (confusion, loss of consciousness, seizure, cerebral edema, cerebral hemorrhage and a burning sensation of the skin). Extreme immunosuppression and mucosal bleeding secondary to myelosuppression and pancytopenia. Severe electrolyte imbalances from diarrhea and dehydration can also be seen. The triad of early emesis followed by alopecia and myelosuppression is typical of ARS [65]. Death often occurs within 2–3 weeks of the onset of the poisoning and due to multiorgan failure [66].
Recently, organophosphate nerve agents such as VX and novichock have been used in chemical terrorism acts for political homicidal poisoning [3, 51, 52].
VX (venomous agent X) is an extremely toxic organophosphorus nerve agent class of chemical weapons. In recent years, pure form of VX was used in the assassination of Kim Jong-nam. Physically, pure form of VX is an amber- colored, odorless, tasteless and oily liquid [3, 67]. The LD50 of VX through dermal contact in a 70 kg human is reported to be 5–10 mg [3, 67].
VX fatalities occur with exposure via inhalation, ingestion or dermal contact. VX as a nerve agent severely disrupt the signaling between the nervous and muscular systems, by irreversible inhibition of acetylcholinesterase and increasing the amount of acetylcholine in the neuromuscular junction, resulting neuromuscular blockade, flaccid paralysis of all the muscles in the body including the diaphragm, and death by asphyxiation [67].
The symptoms and signs of VX acute poisoning are hyperstimulation of muscarinic receptors such as miosis, nausea, vomiting, abdominal cramps, salivation, lacrimation, hyperhidrosis, rhinorrhea, bronchorrhea, bronchospasms, dyspnea, bradycardia, and hypotension. It also hyper- stimulates nicotinic receptor at the neuromuscular junction and results in fasciculations, muscle weakness, and, ultimately paralysis. Nicotinic receptor hyperstimulation also induces hypertension and tachycardia [67]. Dermal exposure with VX causes the appearance of cholinergic toxidrome. It can induce immediate bronchoconstriction or respiratory distress in the lung spaces [67].
Novichoks (in Russian language means “newcomer”) are the suspected nerve agents to carry out political assassinations in case of the Skripal and Navalny poisoning [3, 68, 69]. Novichoks are referred as fourth generation chemical weapons with a group of organophosphorus-based compounds [68]. Novichoks are most commonly found in stable forms as liquid and fine powder forms [3]. The high lipophilicity of these compounds prolongs their detection time in the body. Novichocks may be up to 5-8 times more toxic than VX [3, 68].
The mechanism of action of novichocks involves irreversible inhibition of acetylcholinesterase resulting in cholinergic toxidrome [68, 69]. Symptoms resulting from overstimulation of muscarinic receptors include skin flushing, miosis, visual disturbances, salivation, lacrimation, bronchorrhea, bronchospasm, coughing, dyspnea, sweating, abdominal carmps, diarrhea, bradycardia and involuntary urination and defecation. Overstimulation of nicotinic receptors is responsible for tremor, seizure, muscle weakness up to complete paralysis, tachycardia, hypertension [68, 69].
Biotoxins Used in the Homicidal Poisoning
Application of biotoxins such as tetrodotoxin (TTX), herbal toxin (colchicine) and snake venom in forcible snake bite as homicidal poisoning were notable in this review.
Tetrodotoxin (TTX) is a potent marine neurotoxin that was first identified in puffer fish (mainly in the liver and gonads) and in some fish such as globefish, sunfish, triggerfish and toadfish (order Tetraodontiformes), and in some amphibian, octopus, and shellfish species. Also, it has been isolated from an array of taxa that host TTX-producing
bacteria. TTX is a crystalline, colorless and weakly basic organic substance. TTX is a sodium channel blocker inhibits the firing of action potentials in neurons by binding to the voltage-gated sodium channels in nerve cell membranes and blocking the passage of sodium ions into the neuron.
TTX poisonings were most commonly reported as a food poisoning from countries like Japan, Thailand, and China, but today the risk of TTX poisoning is spreading around the world. Recent studies have shown that TTX-containing fish are being found in other regions of the Pacific, Southeast Asia and in the Indian Ocean, and in the Mediterranean Sea [70, 71].
TTX is extremely toxic. The oral LD50 in mice as 334 μg/kg. TTX is even more dangerous if administered intravenously; the amount needed to reach a lethal dose by injection is 8 μg/ kg in mice [72].
TTX poisoning symptoms typically develop within 30 minutes up to 4 hours of ingestion, in fatal cases, the symptoms are usually present within 10-20 minutes of ingestion. Orolingual numbness followed by developing it in the extremities (acroparesthesia), salivation, sweating, headache, weakness, lethargy, incoordination, tremor, paralysis, bluish skin, loss of voice, dysphasia and seizures. The GI symptoms are often severe and include nausea, vomiting, diarrhea, and abdominal cramps. Death is usually secondary to cardiorespiratory failure [70, 71, 72]. The victim usually exhibits shortness of breath, mydriasis, complete atrioventricular block and hypotension. Mental impairment and cardiac dysrhythmia may occur. Although, the victim completely paralyzed, may be conscious and in some cases completely understandable until shortly before death. However, some victims enter a coma [70, 71, 72].
A rare and strange homicidal poisoning case reported was forced envenomation by snake bite [50]. Snake bite is accidental in urban, suburban and rural areas and desert and few cases were reported to commit suicide. Homicidal snake poisoning is so rare. It was known in ancient world by executing capital punishment by throwing the victim into a pit full of snakes. Or to ask the victim to put his hand inside a small basket harboring a deadly snake. Murder a victim by direct snake bite is so rare. In this case report, killing three children (they were 9-, 6-, and 4-years old girls) by forced snake bite. In forensic investigations, it was found that the father disliked these three children as they were girls. He married another woman and had a male baby. The father decided to get rid of his girl children. To achieve his plan, he trained to become snake charmer and bought a snake (Egyptian cobra) the father forced the snake to bite the three children several times and left them to die. At last, he burned the snake.
Egyptian cobra (Naja haje haje), is widely distributed in Africa and the Middle East. The LD50, its venom is 0.12 µg/g. Envenomation causes local pain and swelling, and may be associated with blistering at the bite site. Neurotoxic and systemic symptoms develop within few hours, and deaths have occurred within 6–16 h after large snakes’ bites, despite the use of antivenom and mechanical ventilation [73]. Four toxins (CM-7, CM-8, CM-9 and CM-10b) were purified from Egyptian cobra venom and belong to a cytotoxin group [74]. Recently, the researchers purified an approximately 15 kDa basic phospholipase A2 enzyme from its venom [75].
Application of Gloriosa superba seeds (contain colchicine) for homicidal poisoning has been reported [49]. Colchicine, a natural tricyclic and lipid-soluble alkaloid found in plants such as the Colchicum autumnale and Gloriosa superba has been used for the treatment and prevention of gout and for familial Mediterranean fever (FMF) and many immunological diseases, but if misused can result in fatal consequences. Accidental poisoning of colchicine as a result of consumption of the herb G. superba has been reported, previously [76]. Colchicine has a narrow therapeutic index (1.2–2.4 mg/day in adults) and long half-life and intentional and unintentional poisoning is common and often associated with a poor outcome. It is readily absorbed after oral ingestion. It is primarily metabolized by the liver and undergoes extensive first-pass metabolism and significant enterohepatic recirculation. It widely distributed and binds to intracellular parts. It is also excreted by the kidneys. High mortality rate was reported after acute ingestions exceeding 0.5 mg/kg. The lowest reported lethal doses of oral colchicine are 7-26 mg [77].
Colchicine toxicity is an extension of its mechanism of action - binding to tubulin and disrupting the cell transport system. Colchicine can inhibit protein synthesis and assembly, decreased endocytosis and exocytosis and cellular motility, altered cell morphology, disruption in mitosis, and interrupted cardiac conduction and contractility. Finally, multisystem organ dysfunction and failure has occurred during 24-72 hours. Colchicine typical toxidrome consistence of gastroenteritis, hypotension, lactic acidosis, and prerenal azotemia [77, 78].
Colchicine poisoning clinical presentations were in three sequential phases: phase 1: 10-24 h after ingestion, gastrointestinal phase mimicking gastroenteritis (profuse vomiting and diarrhea, which can be bloody, abdominal cramps). Phase 2: 24 h to 7 days after ingestion, metabolic acidosis, hypovolumic shock, myelosupression (including anemia, leucopenia, and thrombocytopenia) and multi-organ dysfunction including oliguric renal failure, liver dysfunction, acute myocardial injury and respiratory failure. Death results from rapidly progressive multi-organ failure and sepsis.
Delayed presentation, pre-existing renal or liver impairment are associated with poor prognosis. 3) Recovery typically occurs within a few weeks of ingestion. The fatality rate in colchicine poisoning is 50% [77, 78]
The Role of Forensic Investigations, Autopsy Findings and Postmortem Toxicological Analysis for Determining the Homicidal Poisoning
A Comprehensive forensic investigation including crime scene and evidences analysis and postmortem examination in poisoning-related fatalities is a crucial role to establish the cause and manner of death. A comprehensive analysis of homicidal poisoning fatalities involving forensic investigative data about crime scene evidences evaluation and circumstances, clinical toxicology findings of the poisoned victim who admitted in a hospital, autopsy findings, postmortem histopathological and toxicological results are a fundamental part to diagnosis of fatal homicidal poisoning. Autopsy and postmortem histopathological findings indicative of an poisoned death are scarce and mostly unspecific and majority of pharmaceutical drugs poisonings will leave no characteristic findings at autopsy. Indeed, the most common findings are organ edema and congestion such as pulmonary edema and liver congestion, which are common in all kinds of deaths. However, the external and internal examinations of victim’s corpse gives a valuable data about cause and manner of death. For example, residues of powder or colored material in stomach content might indicate tablet or capsule remains in a oral poisoning. Smell of body (bitter almond in cyanide or nitrobenzen poisoning and garlic odor in organophosphate, phosphorous, phosphine and arsenic deaths) and livor mortis (also known as postmortem hypostasis or postmortem lividity) like cherry red lividity in carbon monoxide poisoning have been observed. Injections marks are important clues for an parental administration of poison or drugs. Noncardiogenic pulmonary edema resulting in heavy, enlarged lungs with edema and congestion along with froth in the airways is typically found in opioid toxicity deaths. Liver necrosis can be the result of paracetamol (acetaminophen) overdose. A massive spontaneous brain hemorrhage and edema, or gastrointestinal bleeding may indicate intake of anticoagulants and radiotoxic agents. Some histopathological findings like as dilated cardiomyopathy (ethanol use) and steatotic or cirrhotic in cases of chronic alcoholic abusers were observed [79].
Postmortem toxicological analysis on biological fluids and tissues including blood (femoral), urine, stomach content, bile, vitreous humor, cerebrospinal fluid, bone marrow, liver, lung, kidney and muscle tissues and hair are important for detection of drugs and poisons in fatal poisonings [80, 81, 82]. There are a wide variety of analytical techniques available for the analysis of toxic substances in biological samples.
The most common techniques used in forensic toxicology can be grouped into spectrophotometry [e.g. Atomic Absorption Spectrophotometry (AAS), Ultraviolet-Visible Spectrophotometry (UV-VIS)], immunoassay [Enzyme- Linked Immunosorbent Assay (ELISA), Radioimmunoassay (RIA), Fluorescence Polarization Immunoassay (FPIA), Cloned Enzyme Donor Immunoassay (CEDIA), and Enzyme Multiplied Immunoassay Technique (EMIT)], chromatography methods (High-Performance and Ultrahigh- Performance Liquid Chromatography (HPLC and UHPLC), Gas-Chromatography with Flame Ionization Detector (GC- FID), or specific detectors for GC like Electron Capture Detector (ECD) and Nitrogen Phosphorus Detector (NPD), Gas-Chromatography with Mass Spectrometry (GC-MS) have been used in forensic toxicology analysis. Also, more sophisticated techniques like Liquid Chromatography with tandem mass spectrometry (LC-MS-MS), tandem GC-MS, Inductively coupled plasma mass spectrometry (ICP-MS) can be used to measure drugs and poisons at trace levels in biological samples [79, 83]. In addition, alpha-particle spectroscopy and gamma-ray spectroscopy can be used for the qualitative analysis of the energy spectra in radioisotopes induced poisoning [84].
Conclusion
Contemporary poisons and drugs used in homicidal poisonings are based in combinations of old and well- described poisons and drugs (including cyanide, arsenic, thallium, atropine, and pesticides) and the use of natural or synthetic drugs and poisons from the group of tetrodotoxin, organophosphorus agents, radioactive substances and poly drug pattern of antipsychotics with antidepressants, and sedative-hypnotics drugs. The reliable detection of cause of homicidal poisoning is a multidisciplinary task between police officers, law enforcement agents, clinical and forensic practitioners including clinical toxicologists, forensic pathologist and forensic toxicologists. Forensic autopsy and postmortem histopathological and toxicological analysis have a critical role for investigation on homicidal poisoning fatal cases. The advanced instrumental analysis (usually using tandem mass spectrometry) can be used for toxicological analysis of trace levels of drugs and poisons in routine and alternative samples in the victims of homicidal poisoning. Finally, it is important to correlate the circumstantial finding, clinical and autopsy results with the histopathological and toxicology results to appropriately assessment of cause and manner of death in homicidal poisoning fatalities.
Conflicts of Interest: The author declares no conflict of interest.
Funding: This research received no external funding.
References
-
Holden IG (1966) Homicidal poisoning. Med Sci Law 6(1): 22-26.
-
Steck-Flynn K (2007) Just a pinch of cyanide: The basics of homicidal poisoning investigations. Law Enforcement Technology 34(10): 118-126.
-
Brunka Z, Ryl J, Brushtulli P, Gromala D, Walczak G, et al. (2022) Selected political criminal poisonings in the years 1978–2020: Detection and treatment. Toxics 10(8): 468.
-
Farrell M (2017) Poisonous Plants, Animals, Bacteria, and Drugs. Criminology of Homicidal Poisoning pp: 63- 77.
-
Shepherd G, Ferslew BC (2009) Homicidal poisoning deaths in the United States 1999-2005. Clin Toxicol (Phila) 47(4): 342-347.
-
Finnberg A, Junuzovic M, Dragovic L, Ortiz-Reyes R, Hamel M, et al. (2013) Homicide by poisoning. Am J Forensic Med Pathol 34(1): 38-42.
-
Muazzam S, Swahn MH, and Alamgir H, Nasrullah M (2012) Differences in poisoning mortality in the United States-2007: epidemiology of poisoning deaths classified as unintentional, suicide or homicide. West J Emerg Med 13(3): 230-238.
-
Tao Z (2023) 106 Cases of homicide poisoning in China-A retrospective study. Legal Medicine 65: 102317.
-
Li Y, Gao Y, Yu X, Peng J, Ma F, et al. (2014) Tetramine poisoning in China: Changes over a decade viewed through the media’s eye. BMC Public Health 14: 842.
-
Sikary AK (2019) Homicidal poisoning in India: A short review. J Forensic Leg Med 61: 13-16.
-
Ström S (2020) Homicidal poisoning in Sweden: A review of cases from 1992–2019. Thesis.
-
Gauthey M, Capua M, Brent J, Finkelstein Y (2019) Poisoning with malicious or criminal intent: Characteristics and outcome of patients presenting for emergency care. Clin Toxicol (Phila) 57(7): 628-631.
-
Hashim A, Vaswani V, Pramod KL, Rasheed S (2016) Homicidal poisons-past, present and future. Indian J Forensic Med Toxicol 10(2): 245-249.
-
Kodikara S (2012) Strychnine in amoxicillin capsules: a means of homicide. J Forensic Leg Med 19(1): 40-41.
-
Li S, Huang W, Duan Y, Xing J, Zhou Y (2015) Human fatality due to thallium poisoning: autopsy, microscopy, and mass spectrometry assays. J Forensic Sci 60(1): 247- 251.
-
Yumoto T, Tsukahara K, Naito H, Iida A, Nakao A (2017) A successfully treated case of criminal thallium poisoning. J Clin Diagn Res 11(4): OD01-OD02.
-
Di Candia D, Muccino E, Battistini A, Boracchi M, Gentile G, et al. (2020) Thallium toxicity due to audultered infusion with thallium sulfate in eight members belonging to the same family nucleus: Autopsy findings and ICP-MS analysis (inductively coupled plasma mass spectrometry) in a triple homicide. Leg Med (Tokyo) 42: 101661.
-
Gensheimer KF, Rea V, Mills DA, Montagna CP, Simone K (2010) Arsenic poisoning caused by intentional contamination of coffee at a church gathering--an epidemiological approach to a forensic investigation. J Forensic Sci 55(4): 1116-1119.
-
Duncan A, Taylor A, Leese E, Allen S, Morton J, et al. (2015) Homicidal arsenic poisoning. Ann Clin Biochem 52(Pt 4): 510-515.
-
Hitosugi M, Tojo M, Kane M, Shiomi N, Shimizu T, et al. (2019) Criminal mercury vapor poisoning using heated tobacco product. Int J Legal Med 133(2): 479-481.
-
Lu Q, Liu Z, Chen X (2017) Mercury poisoning through intravenous administration: Two case reports with literature review. Medicine (Baltimore) 96(46): e8643.
-
Lech T (2015) Detection of mercury in human organs and hair in a case of a homicidal poisoning of a woman autopsied 6 years after death. Am J Forensic Med Pathol 36(3): 227-231.
-
Ananda S, Shaohua Z, Liang L (2013) Fatal barium chloride poisoning: four cases report and literature review. Am J Forensic Med Pathol 34(2): 115-118.
-
Nathwani AC, Down JF, Goldstone J, Yassin J, Dargan PI, et al. (2016) Polonium-210 poisoning: A first-hand account. Lancet 388(10049): 1075-1080.
-
Froidevaux P, Bochud F, Baechler S, Castella V, Augsburger M, et al. (2016) (210)Po poisoning as possible cause of death: Forensic investigations and toxicological analysis of the remains of Yasser Arafat. Forensic Science International 259: 1-9.
-
Abeyasinghe NL, Perera HJM, Weerasinghe DSK (2011) Case report--death by subcutaneous injection of cyanide in Sri Lanka. J Forensic Leg Med 18(4): 182-183.
-
Beno JM, Hartman R, Wallace C, Nemeth D, LaPoint S (2011) Homicidal methanol poisoning in a child. J Anal Toxicol 35(7): 524-528.
-
De-Giorgio F, Grassi VM, Vetrugno G, Rossi R, Fucci N, et al. (2011) Homicide by methane gas. Forensic Sci Int 221(1-3): 1-3.
-
Ruwanpura R, Nandasiri C (2019) Homicidal paraquat poisoning following ligature strangulation. Acad Forensic Pathol 9(3-4): 212-216.
-
Park S, Jeong S, Lee HY (2015) Homicidal paraquat poisoning in exhumed case. Korean J Leg Med 39: 36-40.
-
Liu Z, Huang F, Zhao S, Ma L, Shi Q, et al. (2022) Homicidal paraquat poisoning: Poisoned while drinking. J Forensic Sci 67(3): 1312-1319.
-
Chen F, Ye Y, Jin B, Yi B, Wei Q, et al. (2019) Homicidal paraquat poisoning. J Forensic Sci 64(3): 941-945.
-
Foti F, Sica S, Alma E, De Cristofaro R, Mores N, et al. (2020) Sudden nasal bleeding and brodifacoum: A case of accidental exposure or attempted homicide?. Leg Med (Tokyo) 47: 101772.
-
Sakunthala Tennakoon DAS, Karunarathna WDV, Udugampala USS (2013) Carbofuran concentrations in blood, bile and tissues in fatal cases of homicide and suicide. Forensic Sci Int 227(1-3): 106-110.
-
Kumar A, Kumar A, Murty OP, Gupta VP, Das S (2012) A rare case of homicidal insecticide (organochloro compound) poisoning by intraperitoneal injection. Med Sci Law 52(4): 231-233.
-
Ghoti CB, Apte SS, Bhandarkar MR (2018) A Rare case of insecticide mixture attempted homicidal poisoning using cake as a medium: A case report. Chem Sci Transactions 7(4): 648-651.
-
Mahesan Paul AB, Simms L, Mahesan AM (2018) Intentional heroin administration resulting in homicide in a 10-month old infant. Forensic Sci Int 290: e15-e18.
-
Bonsignore A, Groppi A, Ventura F, De Stefano F, Palmiere C (2016) Fatal methadone intoxication in an infant listed as a homicide. Int J Legal Med 130(5): 1231-1235.
-
Guo W, Luo G, Wang H, Meng X (2015) Homicide by Sch from a syringe-like dart ejected by a compound crossbow. J Forensic Leg Med 30: 25-8.
-
Arbouche N, Godard E, Gheddar L, Raul JS, Kintz P (2021) Attempted murder of a young child followed by an attempted suicide of the mother by injection of insulin Aspart: Identification of quantification of insulin by LC-HRMS and UPLC-MS/MS in blood of the two cases. Journal of Analytical Toxicology 46(2): e65-e72.
-
Baillif-Couniou V, Bartoli C, Sastre C, Chèze M, Deveaux M, et al. (2018) Repeated attempted homicide by administration of drugs documented by hair analysis. J Forensic Leg Med 54: 82-86.
-
Gaillard Y, Breuil R, Doche C, Romeuf L, Lemeur C, et al. (2011) Detection of amitriptyline, nortriptyline and bromazepam in liver, CSF and hair in the homicidal poisoning of a one-month-old girl autopsied 8 months after death. Forensic Sci Int 207(1-3): 16-18.
-
Allibe N, Eysseric-Guerin H, Kintz P, Bartoli M, Bost-Bru C, et al. (2015) Amitriptyline poisoning of a baby: how informative can hair analysis be?. Forensic Sci Int 249: 53-58.
-
Willeman T, Allibe N, Sauerbach L, Barret A, Eysseric- Guerin H, et al. (2022) Homicidal poisoning series in a nursing home: retrospective toxicological investigations in bone marrow and hair. Int J Legal Med 136(1): 123- 131.
-
Yu Y, Gon D, Cao Y, Lu M, Huang F, et al. (2015) A murder disguised as a medical accident: A case report of homicidal poisoning of three anesthetics. Romanian Journal of Legal Medicine 23(1): 45-48.
-
Liu D, Li S, Ma X, Gao J, Xu L, et al. (2016) Homicidal poisoning of heroin and Estazolam: Autopsy and pathological findings, toxicological analysis. International Journal of Multimedia and Ubiquitous Engineering 11(4): 215-222.
-
Carlier J, Escard E, Péoc’h M, Boyer B, Romeuf L, et al. (2014) Atropine eye drops: An unusual homicidal poisoning. Journal of Forensic Sciences 59(3): 859-864.
-
Li J, Zhang X, Ye Y, Li X, Gu Y, et al. (2021) Awareness on tetrodotoxin of illegal activity: forensic issue from a rare homicide case report and literature review. J Forensic Leg Med 79: 102152.
-
Kande Vidanalage CJ, Ekanayeka R, Wijewardane DK (2016) Case report: a rare case of attempted homicide with Gloriosa superba seeds. BMC Pharmacol Toxicol 17(1): 26.
-
Paulis MG, Faheem AL (2016) Homicidal Snake Bite in Children. J Forensic Sci 61(2): 559-561.
-
Vale JA, Marrs TC, Maynard RL (2018) Novichok: a murderous nerve agent attack in the UK. Clin Toxicol (phila) 56(11): 1093-1097.
-
Steindl D, Boehmerle W, Körner R, Praeger D, Haug M, et al. (2021) Novichok nerve agent poisoning. The Lancet 397(10270): 249-252.
-
Kwak YT, Yang YS, Jang HR (2016) Understanding of antipsychotics in elderly patients with dementia. Dement Neurocogn Disord 14(2): 53-69.
-
Narang P, El-Refai M, Parlapalli R, Danilov L, Manda S, et al. (2010) Antipsychotic drugs: sudden cardiac death among elderly patients Psychiatry (Edgmont) 7(10): 25- 29.
-
Lech T, Trela F (2005) Massive acute arsenic poisonings. Forensic Sci Int 151: 273-277.
-
Tournel G, Houssaye C, Humbert L, Dhorne C, Gnemmi V, et al. (2011) Acute arsenic poisoning: clinical, toxicological, histopathological, and forensic features. J Forensic Sci 56(S1): S275-S279.
-
Ratnaike R (2003) Acute and chronic arsenic toxicity. Postgrad Med J 79(933): 391-396.
-
Moore D, House I, Dixon A (1993) Thallium poisoning. Diagnosis may be elusive but alopecia is the clue. BMJ 306(6891):1527-1529.
-
Al Hammouri F, Darwazeh G, Said A, Abu Ghosh R (2011) Acute thallium poisoning: series of ten cases. J Med Toxicol 7(4): 306-311.
-
Syversen T, Kaur P (2012) The toxicology of mercury and its compounds. J Trace Elem Med Biol 26(4): 215-26.
-
Menezes RG, Rizwan T, Khan A, Madadin M, Usman MS (2021) Homicidal pesticide poisoning - An overview. Forensic Sci Rev 33(1): 67-78.
-
Harrison J, Smith T, Fell T, Smith J, Ham G, et al. (2017) Collateral contamination concomitant to the polonium-210 poisoning of Mr Alexander Litvinenko. J Radiol Prot 37(4): 837-851.
-
Diac M, Knieling A, Simona D, Iliescu DB, Sandu I, et al. (2017) Forensic aspects in Polonium-210 poisoning. Revista de Chimie 68(11): 2646-2649.
-
Harrison J, Leggett R, Lloyd D, Phipps A, Scott B (2007) Polonium-210 as a poison. J Radiol Prot 27(1): 17-40.
-
Jefferson RD, Goans RE, Blain PG, Thomas SHL (2009) Diagnosis and treatment of polonium poisoning. Clin Toxicol (Phila) 47(5): 379-392.
-
Le MH (2007) Polonium 210, exposed. J Med Toxicol 3(2): 82-84.
-
Wiener SW, Hoffman RS (2004) Nerve agents: A comprehensive review. J Intensive Care Med 19(1): 22- 37.
-
Bhakhoa H, Rhyman L, Ramasami P (2019) Theoretical study of the molecular aspect of the suspected novichok agent A234 of the Skripal poisoning. Royal Society Open Science 6(2): 1-15.
-
Kloske M, Witkiewicz Z (2019) Novichoks-The A group of organophosphorus chemical warfare agents. Chemosphere 221: 672-682.
-
Katikou P, Gokbulut C, Kosker AR, Campàs M, Ozogul F (2022) An updated review of tetrodotoxin and its peculiarities. Mar Drugs 20(1): 47.
-
How CK, Chern CH, Huang YC, Wang LM, Lee CH (2003) Tetrodotoxin poisoning. Am J Emerg Med 21(1): 51-54.
-
Lorentz MN, Stokes AN, Rossler DC, Lötters S (2016) Tetrodotoxin. Curr Biol 26(19): R870-R872.
-
Omran MAA, Fabb SA, Dickson G (2004) Biochemical and morphological analysis of cell death induced by Egyptian cobra (Naja haje) venom on cultured cells. Journal of Venomous Animals and Toxins including Tropical Diseases 10(3): 219-241.
-
Joubert F, Taljaard N (1978) Naja haje (Egyptian cobra) venom. Purification, some properties and the amino acid sequences of four toxins (CM-7, CM-8, CM-9, and CM- 10b). Biochim Biophys Acta 534(2): 331-340.
-
Salama WH, Shaheen MNF, Shahein YE (2022) Egyptian cobra (Naja haje haje) venom phospholipase A2: A promising antiviral agent with potent virucidal activity against simian rotavirus and bovine coronavirus. Archives of Microbiology 204(8): 526.
-
Raghavendra Babu YP, Manjunath S, Bakkannavar SM, Acharya J, Kumar GNP (2012) Colchicine poisoning: a case report and review of literature. Med Sci Law 52(4): 205-206.
-
Finkelstein Y, Aks SE, Hutson JR, Juurlink DN, Nguyen P, et al. (2010) Colchicine poisoning: the dark side of an ancient drug. Clin Toxicol (Phila) 48(5): 407-414.
-
Wu J, Liu Z (2022) Progress in the management of acute colchicine poisoning in adults. Intern Emerg Med 17(7): 2069-2081.
-
Omran BHF (2022) systematic review of postmortem examination in toxicological fatalities. Egyptian Societ Clin Toxicol J 10(2): 1-19.
-
De Campos EG, Da Costa BRB, Dos Santos FS, Monedeiro F, Alves MNR, et al. (2022) Alternative matrices in forensic toxicology: a critical review. Forensic Toxicol 40(1): 1-18.
-
Kintz P (2017) Hair analysis in forensic toxicology: An updated review with a special focus on pitfalls. Curr Pharm Des 23(36): 5480-5486.
-
Dinis-Oliveira RJ, Carvalho F, Duarte JA, Remião F, Marques A, et al. (2010) Collection of biological samples in forensic toxicology. Toxicol Mech Methods 20(7): 363- 414.
-
Chung H, Choe S (2017) Overview of forensic toxicology, yesterday, today and in the future. Curr Pharm Des 23(36): 5429-5436.
-
Lin Z, Wu Z (2009) Analysis of polonium-210 in food products and bioassay samples by isotope-dilution alpha spectrometry. Appl Radiat Isot 67(5): 907-912.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review