Non-Accidental Injury Involving a Neonate
Non-accidental injury (NAI) was brought forward by the investigation and research that was conducted by Ambroise Tardieu, John Caffey and Henry Kempe. Whiplash-shaken infant syndrome and battered child syndrome are the other alternative terms used. NAI is defined as repetitive physical abuse. Marks of injuries such as multiple bruises or abrasions of differing ages and patterns, bite marks, burns and radiological evidence of old bony fractures are valuable indicators in distinguishing nonaccidental from accidental injuries. In addition, birth trauma, bleeding disorders, sepsis, vasculopathy, congenital anomalies, metabolic abnormalities and true accidental injuries must be ruled out beforehand with a meticulous approach when dealing with such deaths. Here, we report a case of a 28-day-old female neonate who was brought in unresponsive by her parents and was pronounced dead at the accident and emergency department. The external examination did not reveal any gross abnormality whereas, the internal examination revealed subgaleal haematoma, subdural and subarachnoid haemorrhage. The microscopic examination revealed retinal haemorrhage. The cause of death was attributed to blunt force trauma to the head. This case is a reminder to all forensic and clinical pathologists that an extremely uncommon manifestation can occur, therefore, a meticulous approach should always be undertaken, before corroborating a cause of death. In conclusion, the findings of the forensic autopsy and histopathology facilitated the investigation and established the cause of death.
Introduction
The neonatal mortality rate in Malaysia has been declining at a moderate rate since 1955, albeit, in 2018, 4.3 deaths per 1000 live births were reported. In England and Wales, according to the Trauma Audit and Research Network that was conducted from the year 2004 to 2013, 1126 children were subjected to non-accidental injuries, whereas, 23,529 child abuse cases were recorded in the UK between 2019 and 2020 according to the National Society for the Prevention of Cruelty to Children [1, 2].
The term non-accidental injury (NAI) was developed due to the observation, investigation and research that was conducted historically by Ambroise Tardieu, John Caffey and Henry Kempe [3, 4]. Terms such as whiplash shaken infant syndrome and battered child syndrome are such examples. Post-mortem examination has an important connotation in the investigation of criminal and non-criminal deaths; besides that, it has also been a major contributor to the development of medical education and laws relating to child abuse.
NAI is defined as repetitive physical abuse suffered due to beating, shaking, throwing or dropping the neonate or child. External marks of injury such as bruising, abrasions, lacerations, bite marks and burns are useful indicators in distinguishing non-accidental from accidental injuries. The victims are often less than 3 years of age. Internal injuries to the head and abdomen are a frequent discovery. Meningeal haemorrhages are customary with or without skull fractures and are commonly associated with retinal haemorrhages [3, 5]. Long bone and rib fractures should also be considered with caution.
Nevertheless, other causes such as trauma at birth, bleeding disorders, sepsis, vasculopathy, congenital anomalies and metabolic abnormalities must be ruled out beforehand. One such case was reported in the UK where doctors missed a vitamin D deficiency rickets-related death in a child, which resulted in the wrongful prosecution of the parents [6]. Therefore, a meticulous approach should be practised when dealing with such deaths.
Risk factors associated with non-accidental injury can be divided into two groups which are intrinsic to the child such as prematurity, low birth weight and numerous medical issues, and intrinsic to the parents or family such as poverty, young or single parents, unwanted pregnancy, substance misuse, mental health issues and history of physical or sexual abuse during their childhood [4, 7].
Case Report
A 28-day-old female neonate was brought in unresponsive to a government clinic by her parents on the 25th of February 2019 around 1420H. Resuscitation was immediately initiated but unfortunately to no avail. The neonate was pronounced dead at 1515H, and the body was sent to the General Hospital for post-mortem examination. She was delivered at full term through spontaneous vaginal delivery, and her antenatal history was unremarkable. Otherwise, there was no history of illness, evidence of trauma or neglect reported. Death was classified as sudden death by the investigating police officer.
Post Mortem Examination
A post-mortem examination was performed within 24 hours after the death. The body examined was of a normally formed, well-nourished female neonate. The body weight was 3650g. The crown heel length was 54cm, the crown-rump length was 44cm and the head circumference was 36cm, whereas the abdominal circumference was 34cm, the chest circumference was 36cm and the foot length was 6.2cm.
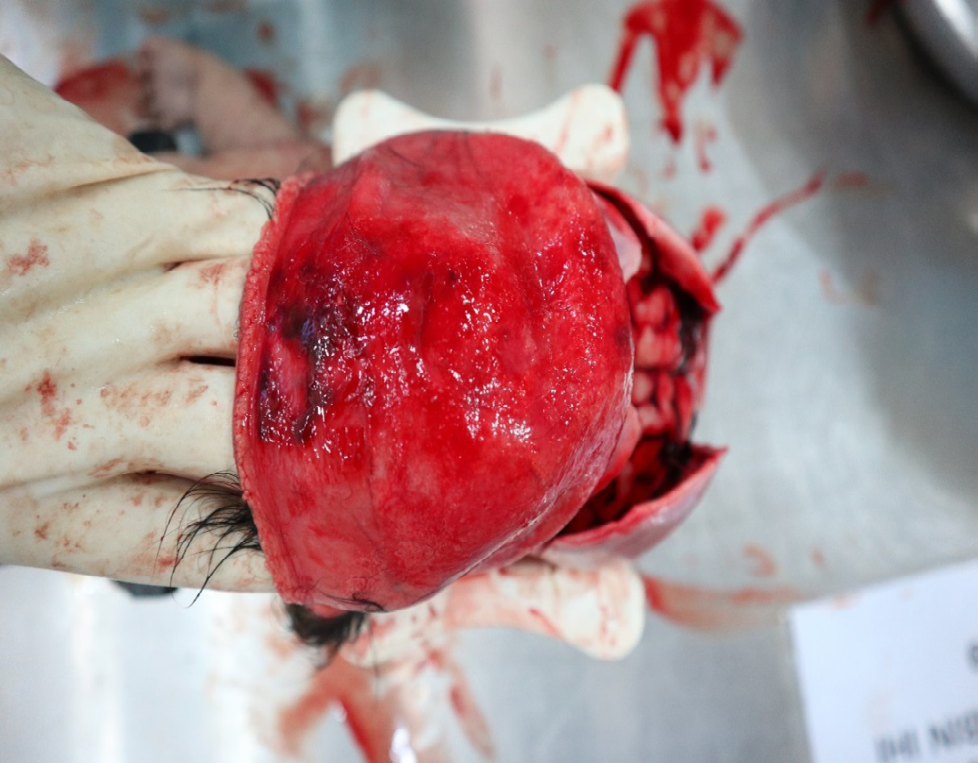
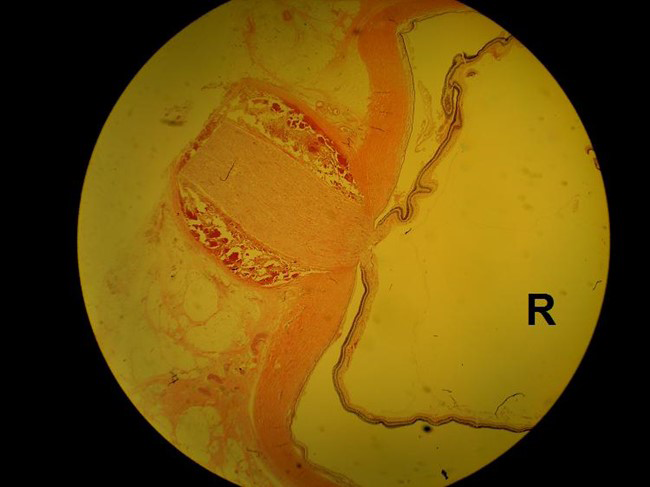
There was no dysmorphism or discernible abnormalities seen on external examination. Two parallel linear abrasions were noted on the left side of the chest, measuring 1.5cm x 0.2cm, located 3.3cm and 3.8cm respectively from the left nipple (Figure 1). One linear abrasion measuring 0.8cm x 0.1cm on the right lateral forearm was noted (Figure 2). The skull was not fractured. There was no obvious suture diastasis. Subgaleal haematoma was present at the vertex, measuring 10cm x 6cm upon reflecting the scalp (Figure 3). Meninges were intact but appeared tensed. Subdural haemorrhage was present in liquid form, measuring 15ml (Figure 4). There was subarachnoid haemorrhage seen at the vertex of both cerebral hemispheres (Figure 5). The brain was grossly oedematous and weighed 470gms. The cut section of the brain revealed no mark of injuries or pathology, nor was there any gross evidence of infection in the meninges and brain matter. The microscopic examination of the brain revealed oedema but there were no haemorrhages seen, whereas, the microscopic examination of the eye showed haemorrhages around the nerve insertion (Figure 6). There were no other injuries, pathologies or abnormalities apart from the aforementioned. No recent or old fractures were noted. Blood, urine, vitreous humour and cerebrospinal fluid for microbiology, biochemistry and genetic analysis were normal. Toxicology analyses of blood, vitreous humour and urine did not detect ethyl alcohol, common basic drugs and any other substances.




Discussion
This case describes a non-accidental injury involving a 28-day-old female neonate. The neonatal period which is the first 28 days of life is the most vulnerable period for a child’s survival, hence, diligent care is paramount. Non- accidental injury was suspected in this case upon finding three linear abrasions on external examination even though the history of trauma or evidence of fracture on radiological examination was not present. The abrasions on the chest and arm correlate to the area and pattern of injury commonly detected in child abuse. The abrasion on the chest and arm could have been inflicted by tightly gripping or squeezing the chest or gripping the arm to pull or drag the child roughly.
It has been stated by Dimaio & Dimaio (2001) that NAI has three categories which are classical battered child, angry homicide and gentle homicide [8]. A battered child is defined as a child who has sustained multiple bruises or abrasions of differing ages and patterns. Angry homicide is a characteristic of a child who has sustained an acute injury without any signs of chronic abuse, whereas, gentle homicide denotes smothering and Munchausen syndrome by proxy [8].
Head injuries that are often encountered are subdural and subarachnoid haemorrhage with or devoid of skull fracture. The survival rate of non-accidental head injury in children is merely 15% according to the Centers for Disease Control and Prevention (CDC) [4]. The presence of subgaleal haematoma is indicative of blunt-force trauma. The force of trauma could vary, and based on the post-mortem examination absence of external marks of injury on the scalp corresponds that the decedent sustained a moderate force of trauma. Furthermore, the hair on the scalp could also act as a protective layer.
Subdural and subarachnoid haemorrhage is a leading cause of morbidity and mortality. NAI should be suspected in all young children presenting with subdural or subarachnoid haemorrhage [5]. According to a study conducted at Birmingham Children’s Hospital, head trauma was the leading cause of death in NAI [1]. The decedent in this case sustained both subdural and subarachnoid haemorrhage but there was no evidence of any skull fracture. This signifies that the trauma suffered was probably due to blunt force or violent shaking.
The pathophysiology causing these traumatic brain injuries (TBI) can be attributed to four reasons. The first is due to the thin and soft cranium which produces very minimal protection for the brain matter.
Next, the brain is highly vascularized and rich in water, hence, heightening the risk of cerebral oedema and haemorrhage. Third, the incomplete formation of the cerebral myelin sheath and soft brain tissue makes it susceptible to shear force injury leading to tearing of the bridging veins and subsequently causing subdural haemorrhage. Finally, the brain of the infant is vulnerable to acceleration-deceleration damages due to the incomplete development of the neck muscles and a large head-to-body ratio. This ultimately leads to the whiplash movement of the brain leading to contusions and haemorrhage [8, 9, 10].
Besides traumatic brain injury, retinal haemorrhage is another sensitive and specific finding commonly detected in NAI deaths. Bilateral retinal haemorrhages associated with intracranial injuries are indicative of abuse. Other ocular injuries such as periorbital haematoma, subconjunctival haemorrhage, dislocated lens and retinal detachment could also manifest [4, 11]. Violent shaking, retinoschisis, intracranial haemorrhage leading to raised intracranial pressure and tracking of blood in the eye could lead to these ophthalmic injuries [8, 11].
Conclusion
In conclusion, the findings of the forensic autopsy facilitated the investigation and established the cause of death. It was concluded that the cause of death was blunt force trauma to the head. The deceased suffered a blunt force impact to her head, which resulted in intracranial injuries predominantly, cerebral oedema, subdural haemorrhage and subarachnoid haemorrhage. From the examination of the brain and meninges, the trauma was less than 24 hours from death. Otherwise, there was no other evidence of previous injuries indicating repetitive trauma. This is an example of a typical angry homicide which is the most frequent discovery in non-accidental injury [7, 8]. Thus, this case discusses the importance of conducting a detailed and comprehensive post- mortem examination which includes radiology, microbiology, biochemistry and genetic analysis and screening on neonatal deaths in determining the cause of death.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the legal guardian has given his consent for images and other clinical information to be reported in the journal. The guardian understands that names and initials will not be published and due efforts will be made to conceal patient identity, but anonymity cannot be guaranteed.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest
References
-
Taylor J, Efstathiou N (2017) Non-Accidental and Neglectful Injuries in Children: Patterns and typology. Birmingham Children’s Hospital, University of Birmingham.
-
Cawson P, Wattam C, Brooker S, Kelly G (2000) Child Maltreatment in the United Kingdom: a Study of the Prevalence of Abuse and Neglect. NSPCC Research Findings pp: 1-21.
-
Picini M, Gonçalves JRR, Bringhenti T, Forlin E (2017) Evaluation of suspected physical abuse in children: a 500-case study. Rev Bras Ortop 52(3): 284-290.
-
Paul AR, Adamo MA (2014) Non-accidental trauma in pediatric patients: a review of epidemiology, pathophysiology, diagnosis and treatment. Transl Pediatr 3(3): 195-207.
-
Cheah IG, Kasim MS, Shafie HM, Khoo TH (1994) Intracranial haemorrhage and child abuse. Ann Trop Paediatr 14(4): 325-328.
-
Dyer C (2012) Prosecution of Parents over Baby’s Death Raises Controversy over Diagnosing Child Abuse. BMJ 344: e2932.
-
Nor FM, Zainun KA (2016) Non-accidental injury in children in Kuala Lumpur: An urban perspective. Egyptian Journal of Forensic Sciences 6(4): 553-557.
-
DiMaio VJ, DiMaio D (2001) Forensic Pathology In: 2nd (Edn.), CRC Press, New York, USA, pp: 1-594.
-
Saukko P, Knight B (2016) Knight’s forensic pathology, In: 3rd (Edn.), Boca Raton: CRC Press, London, UK, pp: 1-673.
-
Vanezis P (2020) Essential forensic medicine. Wiley.
-
Wendel LJA, Longmuir SQ, Syed NA (2009) Non- accidental Trauma: An unresponsive infant with bilateral retinal haemorrhages. EyeRounds.org.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review