Degenerative Injury and Acute Trauma Lead to Rotator Cuff Tear: How can we Judge the Relationship Between Acute Trauma and Disease?
Degenerative injury (own disease) and acute trauma are the two most common causes of rotator cuff tears (RCTs). It is always difficult to judge whether an RCT is caused by the former, the latter or the combination of both when the two factors coexist in the clinical appraisal of forensic medicine. To solve this problem, this paper reviews the literature from four aspects: the anatomical structure of the rotator cuff, the injury mechanism of the RCT, medical imaging and forensic clinical identification. We hope to provide a reliable forensic path for determining the relationship between acute trauma and one’s own disease through a discussion of the following content. Key ideas • The signs of accompanying injury on MRI and the magnitude and form of acute trauma can be used to analyze whether acute trauma leads to RCT. • Depending on X-ray or CT and MRI, the factors of own disease can be analyzed to determine the degree of the disease. • The above two parts form clear appraisal results for court judgment.
Zhongchong Liu¹, Xiwei Zhang¹ and Liangcheng Ding*²
¹The 80th Group Military Hospital of the Chinese People's Liberation Army, China ²Dongying People's Hospital (Dongying Hospital of Shandong Provincial Hospital Group), China Keywords: Rotator Cuff Tear; Medical Imaging; Forensic Medicine
Abbreviations
RCTs: Rotator Cuff Tears; AI: Acromial Index; LAA: Lateral Acromion Angle; CSA: Critical Shoulder Angle AHD: Acromial- Humeral Distance; AGA: Acromial Glenoid Angle; GI: Glenoid Inclination; FI: Fatty Infiltration; OG: Occupation Grade.
Introduction
RCT can be divided into acute traumatic tears and degenerative tears (own disease) depending on the cause of the damage [1, 2, 3, 4]. Cases in which two factors coexist often appear in forensic identification. However, the lack of understanding of objective identification factors often leads many forensic appraisers to face trouble, and the final appraisal opinions arouse the doubts of the parties. Therefore, to provide a reliable practice basis for the judgment of the injury relationship of RCTs, this paper combines the results of previous clinical research to analyze the influencing factors of RCTs from the perspective of forensic medicine.
Anatomy of the Rotator Cuff
The tendon complex formed by the terminal tendons of the infraspinatus, supraspinatus, teres minor, and subscapularis muscles is called the rotator cuff. The rotator cuff serves as a bearing to maintain the stability of the menciohumeral joint and prevent joint dislocation during joint movement.
The tendons constituting the rotator cuff arise from the scapula, with the subscapularis ending at the lesser tuberosity of the humerus and the infraspinatus, supraspinatus, and teres minor ending at the greater tuberosity of the humerus. In addition, because the branches of the superior and inferior scapular arteries and the branches of the pronator arteries cross each other near the insertion of the greater tuberosity of the humerus of the supraspinatus and infraspinatus muscles, the blood supply of the corresponding parts is significantly reduced, which Codman EA, et al. [5] called this area “the risk area of poor blood supply”. In clinical practice, supraspinatus muscle tears are prone to be accompanied by partial infraspinatus muscle fiber bundle rupture, accounting for approximately 90% of RCTs [6].
Mechanism of Rotator Cuff Tear
Degenerative Tears (Own Disease): According to Codman’s theory of endogenetic tendinosis [7], with aging, muscle cells begin to degenerate and become necrotic, and some fibers rupture until RCT, which is a progressive pathological change. Using ultrasound to analyze 90 patients with rotator cuff tears aged 30--90 years, Milgrom C, et al. [8] reported that the incidence of RCT significantly increased in patients over 50 years of age, and the incidence of RCT was greater than 50% in patients over 70 years of age and up to 80% in patients over 80 years of age.
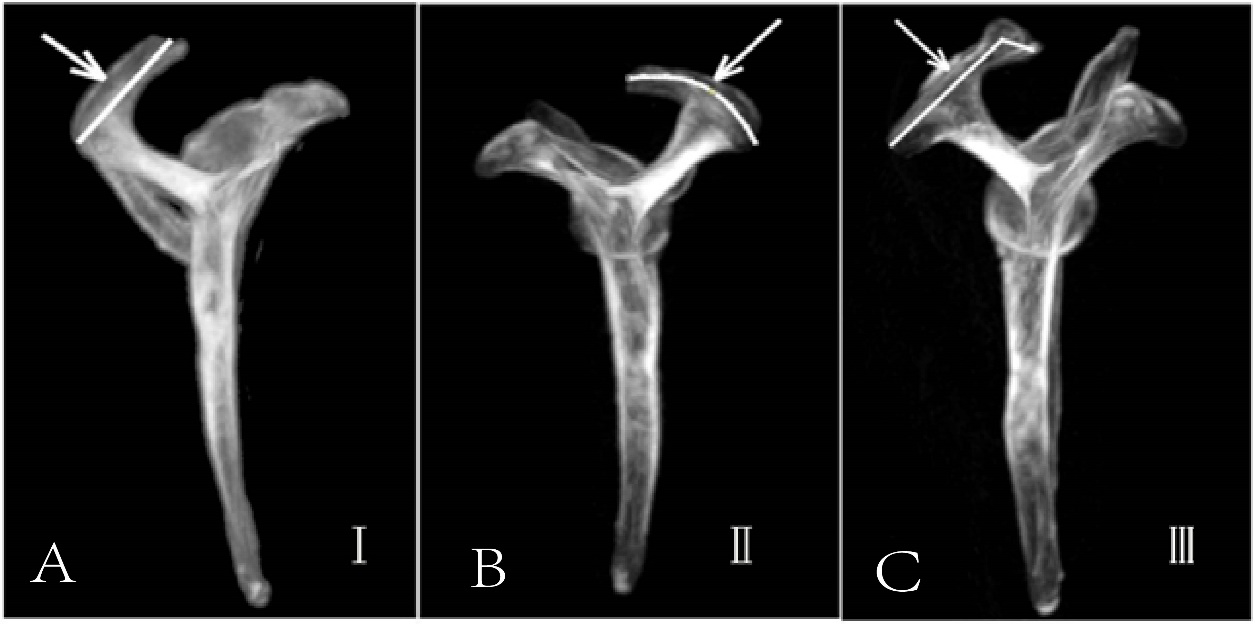
Neer’s theory of external impingement [9]: The subacromial bursa, supraspinatus and infraspinatus muscles are repeatedly rubbed and impacted in the subacromial space when the shoulder is lifted, which results in a series of pathological changes, such as local inflammation and injury. This phenomenon is called impingement syndrome. Depending on the location of impingement, it can be divided into subacromial impingement, subcoracoid impingement and intrarotator cuff impingement. In clinical practice, impingement syndrome is usually referred to as subacromial impingement. Since this theory was proposed, the relationship between the shape of the acromion and rotator cuff tear has attracted increasing attention. In 1986, Bigliani LU, et al. [10] classified the data, as shown in Figure 1A previous study revealed that 95% of RCTs involved subacromial impingement, especially type III acromions [11].
Acute Trauma Tears (Trauma Factor)
According to the magnitude of external force and injury time, trauma can be divided into acute trauma and repeated minor trauma (chronic subacromial impingement). The latter is a disease factor and is the cause of most RCTs. In contrast, RCTs and investigations of the normal bone structure of the shoulder caused by acute trauma are rare, and injury factors in combination with the mode of force action during trauma need to be analyzed [12]. For example, if the external force acts on the top of the shoulder joint, the acromion and proximal humerus will be affected by the downward impact force, leading to bone injury and rotator cuff tear in the corresponding parts. Pulling the upper arm downward, the force acts on the greater/lesser tuberosity of the humerus, causing the attachment point of the rotator cuff to tear and also leading to the medial and inferior dislocation of the shoulder joint. When the upper arm is subjected to extreme abduction and external rotation, the reduction of the subacromial distance leads to the tear of the supraspinatus muscle, and the bone morphology generally does not change significantly.
Medical Imaging Examination
X-ray and CT The anteroposterior radiographs and Y-view radiographs of the supraspinatus outlet, or MPR and VRT reconstruction images of CT scan are often used to evaluate the changes of the shoulder bone structure of degenerative- RCT. Evaluation indicators include Acromial index (AI), Lateral acromion angle (LAA), Critical shoulder angle (CSA), and Acromial-humeral distance (AHD), Acromial glenoid angle (AGA), Glenoid inclination (GI), and other indicators.
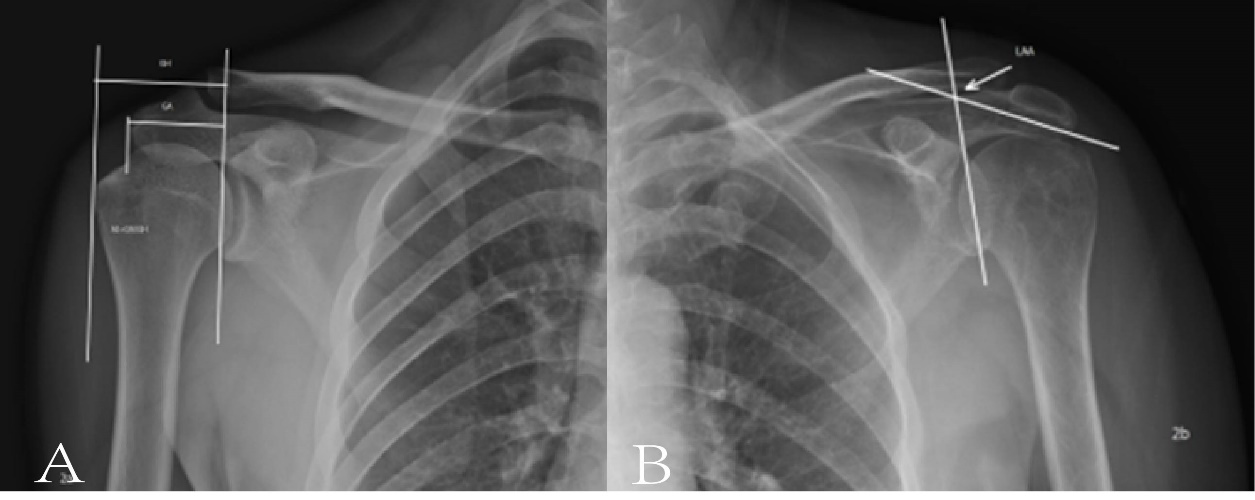
AI is the ratio of the distance from the outermost edge of the acromion and the outermost edge of the humeral head to the glenoid tangent line, respectively, on the anteroposterior radiograph, Figure 2A. AI is used to evaluate the lateral extension of the acromion. The risk of rotator cuff tear increases with the increase of AI. The reason may be that the increase of the lateral extension of the acromion will increase the force of the deltoid muscle in the vertical direction, which will lead to the increase of the risk of RCT.
Pandey V, et al. [11] found that an increase in AI indicates the presence of a full-thickness RCT. However, in the actual measurement, AI is greatly affected by the relative position of the humeral head and acromion, and standardization of the X-ray projection position is particularly important for ensuring measurement accuracy.
LAA refers to the angle between the tangent line of the inferior surface of the acromion and the glenoid on the anteroposterior X-ray (Figure 2B). Banas MP, et al [13]. reported that the average value of this angle was approximately 78°, and the incidence of RCT tended to increase as the LAA angle decreased.
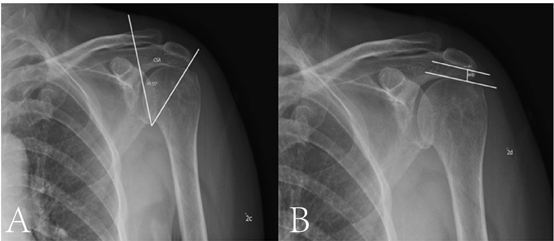
The CSA is the angle between the line connecting the lowest point of the glenoid to the outermost border of the acromion and the glenoid tangent (Figure 3A). This parameter takes into account the influence of both the glenoid tilt angle and lateral acromion extension. According to the literature, a CSA>35° indicates a rotator cuff tear [14]. In addition, other studies have reported that the CSA angle of patients with complete rotator cuff tears and arthritis tends to significantly increase [15], and analysis suggests that the extra load of the supraspinatus muscle to maintain the stability of the shoulder joint may be caused by the extra load of the supraspinatus muscle. Chalmers PN, et al. [16] reported that the CSA angle was not correlated with the severity of rotator cuff tears or disease progression.
AHD refers to the vertical distance from the lowest point of the lower acromion to the humeral head (Figure 3B), which is affected by the upward displacement of the acromion and the humeral head at the same time and is an effective indicator for evaluating the RCT and the degree of tear. The normal range of AHD is 7–13 mm, with less than 7 mm indicating a rotator cuff tear. Nove-Josserand L, et al. [17] reported that reduced AHD was associated with tears of multiple tendons, such as the supraspinatus and infraspinatus, rather than merely suggesting supraspinatus tears.
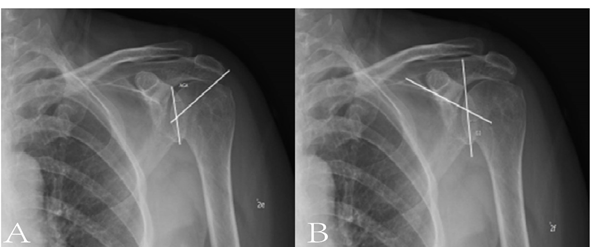
The AGA refers to the angle formed by the connection between the highest point of the glenoid and the midpoint of the connection between the lowest point and the inferior edge of the acromion [18] (Figure 4A). AGA is a predictive indicator for the diagnosis of RCT and shoulder arthritis and is strongly correlated with the CSA, AHD, and AI.
The angle between the bottom margin of the superior fossa of the GI finger and the connection between the highest point and the lowest point of the glenoid is shown in Fig. 4B. This parameter has little individual variation and is also an effective indicator. Beeler S, et al. [15] reported that the GI angle of full-thickness rotator cuff tears was approximately 98.6° greater than 91.0° in patients without rotator cuff tears and that the angle was the largest in patients with arthritis, suggesting that the GI angle may be related to the development of shoulder joint diseases.
MRI can be used not only to diagnose RCT and tear types but also to evaluate fatty infiltration and atrophy of the tendon. Studies have shown that the sensitivity and specificity of MRI in the diagnosis of RCT tears can reach more than 90% [19]. In forensic expertise, MRI is also the main reference basis for determining the relationship of RCTs.
Rotator cuff fatty infiltration (FI) and occupation grade (OG) are common causes of degenerative RCTs [20]. Fuchs B, et al. [21] first used sagittal T1WI images of MR images to classify the degree of fatty infiltration. In addition, the occupation grade (OG) by Thomazeau H, et al. [22], the tangent sign (TS) by Zanetti M, et al. [23], and the grading system of rotator cuff atrophy by Warner JJ, et al. [24] can also be used to quantitatively measure the degree of rotator cuff atrophy. The former two methods are most commonly used at present.
OG refers to the surface area of the supraspinatus muscle over the surface area of the supraspinatus fossa on oblique sagittal T1WI images. The tangent sign refers to the degree to which the line between the superior edge of the scapula and the supraspinatus muscle jumps on the oblique sagittal plane of the MR image (Table 1 and Figure 5). The above study revealed that the more severe the degree of FI and OG was, the more likely the RCT was.
| Types | Extent |
|---|---|
| Fuchs system FI grading | |
| Mild | No fat or little fat |
| Medium | More muscle than fat |
| Severe | Equal amounts of fat and muscle or more fat than muscle |
| Thomazeau system OG grading | |
| Ⅰ | 0.6~1.0 |
| Ⅱ | 0.4~0.6 |
| Ⅲ | <0.4 |
| Warner System TS rating | |
| Ⅰ | Normal |
| Ⅱ | Medium |
| Ⅲ | Heavy |
| Ⅳ | Severe |
Table 1: Fatty Infiltration and Tendon Atrophy.
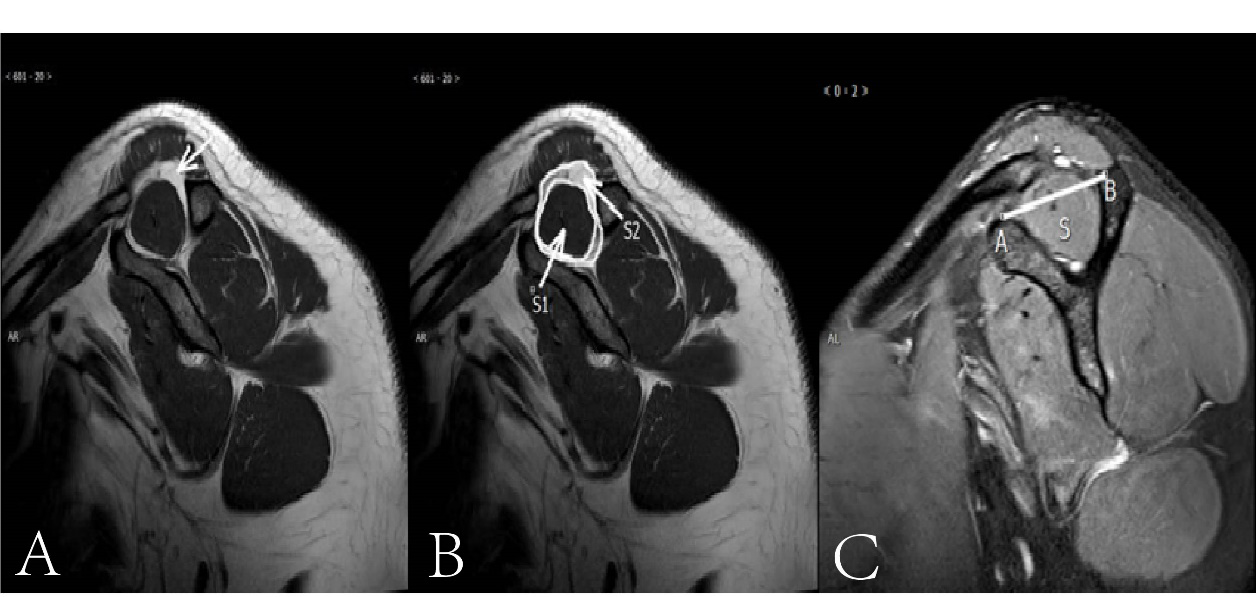
Figure 5: A: Oblique Sagittal T1WI Image, White Signal Represents Adipose Tissue (Arrow) (Fuchs Grade); B: Oblique Sagittal T1WI Image, S1 for Supraspinatus Muscle, S2 for Fat +S1, S1/S2=OG, (Thomazeau Classification); C: Oblique Sagittal Fat Suppression T2WI Image, Line Segment AB is the Connection Between the Superior Edge of the Two Ends of the Scapula, S Represents the Supraspinatus Muscle, S Above AB Is I°, Near AB is Ⅱ°, Slightly Below AB Is Ⅲ°, and A Little Residual S Is Ⅳ° (Warner Classification).
Forensic Clinical Identification
As mentioned above, we need to judge the relationship between acute trauma and one’s own disease, especially in the case of RCTs involving acute trauma without serious shoulder fracture. Accurately judging the degree of participation of each factor is related to the compensation of the victims and the fairness of the judicial trial. According
to forensic practice, when the relationship is judged, the following principles should be followed.
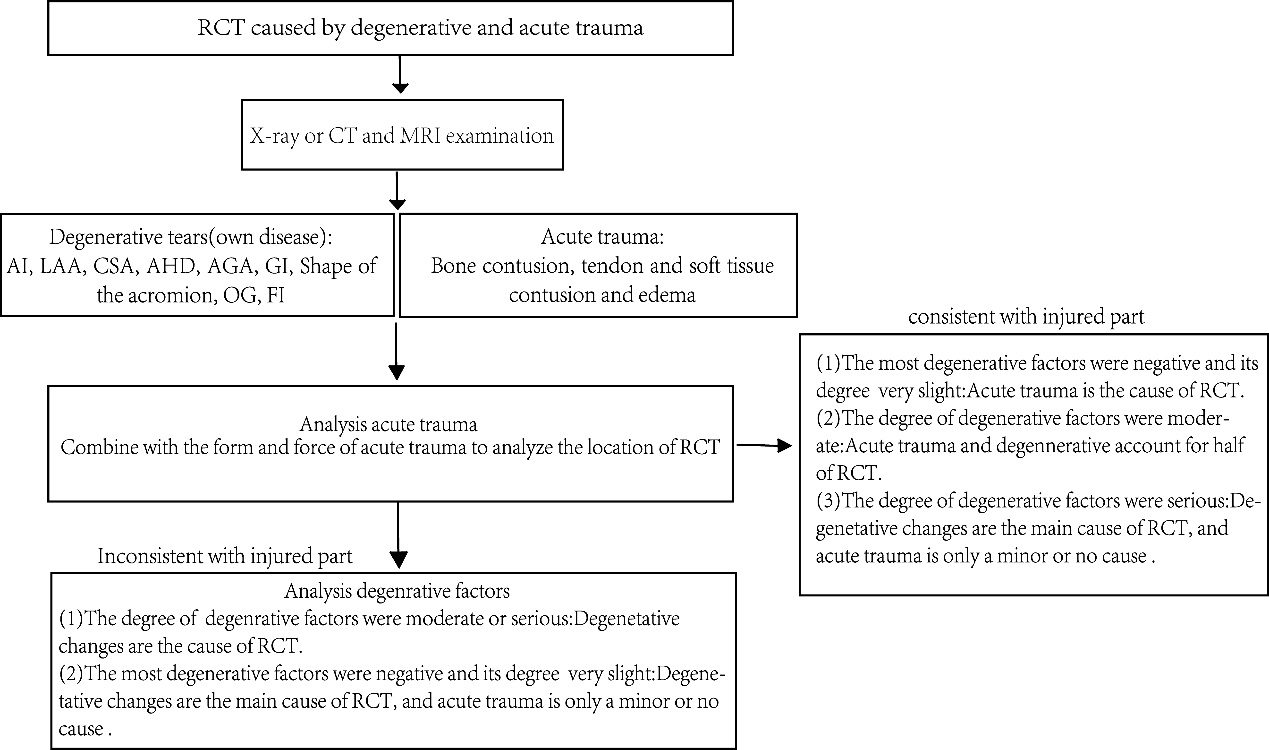
First, the traumatic factor is analyzed. The process and mode of trauma, especially lateral shoulder joint injury, excessive abduction of the upper limbs and shoulder dislocation during tussling and other situations, should be carefully considered. The location of the rotator cuff tear was analyzed according to the form and force of trauma. Among all the inspections, the signs of injury shown by MRI, bone contusion, tendon and soft tissue contusion and edema constitute the most valuable judgment basis. Studies have shown that the greater the force of acute trauma is, the more obvious the sign of accompanying injury on MRI [25]. In addition, compared with lesions alone, RCTs caused by acute trauma generally occur at the direct force site of the rotator cuff. Second, the factors of own disease should be analyzed, especially the cases that lack signs of accompanying injury and trauma, which may lead to RCTs. The relevant indicators of degeneration, CSA, AHD, AGA, FI, OG and other factors were analyzed by X-ray or CT and MRI to determine the degree of disease involvement. Finally, the analysis results of the first and second steps are combined to form a clear appraisal opinion. The opinion should specify what specific factors caused RCT, providing an objective basis for the court’s decision.
Conclusion
The relationship between acute trauma and one’s own disease, which is related to the notarization of court decisions and the conviction of the parties and the compensation of the victims, is accurate. In summary, first, the magnitude and form of acute trauma combined with signs of accompanying injury on MRI were used to analyze whether acute trauma leads to RCT. An analysis of the factors of own disease, especially in patients who lack signs of accompanying injury and acute trauma, may result in RCTs, including AHD, FI, OG and other factors. X- or CT and MRI can be used to determine the degree of disease. Finally, the above two parts form clear appraisal results for court judgment (Figure 6).
References
-
Li X, Xiao Y, Shu H, Sun X, Nie M (2022) Risk Factors and Corresponding Management for Suture Anchor Pullout during Arthroscopic Rotator Cuff Repair. J Clin Med 11(22): 6870.
-
Lawrence RL, Moutzouros V, Bey MJ (2019) Asymptomatic Rotator Cuff Tears. JBJS Rev 7(6): e9.
-
Guevara BG (2023) Editorial Commentary: In Contrast to Chronic, Degenerative Rotator Cuff Tears, the Critical Shoulder Angle in Traumatic Rotator Cuff Tears Can Be Ignored. Arthroscopy 39(2): 232-233.
-
McCrum E (2020) MR Imaging of the Rotator Cuff. Magn Reson Imaging Clin N Am 28(2): 165-179.
-
Codman EA, Akerson IB (1931) The Pathology Associated with Rupture of the Supraspinatus Tendon. Ann Surg 93(1): 348-359.
-
Song A, Cannon D, Kim P, Ayers GD, Gao C, et al. (2022) Risk factors for degenerative, symptomatic rotator cuff tears: a case‒-control study. J Shoulder Elbow Surg 31(4): 806-812.
-
Codman EA (1990) Rupture of the supraspinatus tendon. 1911. Clin Orthop Relat Res (254): 3-26.
-
Milgrom C, Schaffler M, Gilbert S, Van Holsbeeck M (1995) Rotator-cuff changes in asymptomatic adults. The effect of age, hand dominance and gender. J Bone Joint Surg Br 77(2): 296-298.
-
Neer CS 2nd (1972) Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am 54(1): 41-50.
-
Bigliani LU, Ticker JB, Flatow EL, Soslowsky LJ, Mow VC (1991) The relationship of acromial architecture to rotator cuff disease. Clin Sports Med 10(4): 823-838.
-
Pandey V, Vijayan D, Tapashetti S, Agarwal L, Kamath A, et al. (2016) Does scapular morphology affect the integrity of the rotator cuff?. J Shoulder Elbow Surg 25(3): 413- 421.
-
Guo G, Niu S, Li C (2021) Research progress and forensic significance of rotator cuff injury. J Chinese Journal of Forensic Sciences (2): 33-37.
-
Banas MP, Miller RJ, Totterman S (1995) Relationship between the lateral acromion angle and rotator cuff disease. Journal of Shoulder and Elbow Surgery 4(6): 454-461.
-
Mantell MT, Nelson R, Lowe JT, Endrizzi DP, Jawa A (2017) Critical shoulder angle is associated with full-thickness rotator cuff tears in patients with glenohumeral osteoarthritis. J Shoulder Elbow Surg 26(12): e376-e381.
-
Beeler S, Hasler A, Getzmann J, Weigelt L, Meyer DC, et al. (2018) Acromial roof in patients with concentric osteoarthritis and massive rotator cuff tears: multiplanar analysis of 115 computed tomography scans. J Shoulder Elbow Surg 27(10): 1866-1876.
-
Chalmers PN, Salazar D, Steger-May K, Chamberlain AM, Yamaguchi K, et al. (2017) Does the Critical Shoulder Angle Correlate With Rotator Cuff Tear Progression? Clin Orthop Relat Res 475(6):1608-1617.
-
Nové-Josserand L, Edwards TB, O’Connor DP, Walch G (2005) The acromiohumeral and coracohumeral intervals are abnormal in rotator cuff tears with muscular fatty degeneration. Clin Orthop Relat Res (433): 90-96.
-
Vermeulen V, Kozma E, Delsupehe A, Cornillie P, Stock E, et al. (2023) Scapular morphology of great apes and humans: A three-dimensional computed tomography- based comparative study. J Anat 242(2):164-173.
-
Eustace SK, Murphy AN, Hurley DJ, Abul AHA, Kavanagh E (2023) MRI findings in atraumatic shoulder pain- patterns of disease correlated with age and gender. Ir J Med Sci 192(2): 847-852.
-
Giri A, Freeman TH, Kim P, Kuhn JE, Garriga GA, et al. (2022) Obesity and sex influence fatty infiltration of the rotator cuff: the Rotator Cuff Outcomes Workgroup (ROW) and Multicenter OrthopedOrthopaedic Outcomes Network (MOON) cohorts. J Shoulder Elbow Surg 31(4): 726-735.
-
Fuchs B, Weishaupt D, Zanetti M, Hodler J, Gerber C (1999) Fatty degeneration of the muscles of the rotator cuff: assessment by computed tomography versus magnetic resonance imaging. J Shoulder Elbow Surg 8(6): 599-605.
-
Thomazeau H, Boukobza E, Morcet N, Chaperon J, Langlais F (1997) Prediction of rotator cuff repair results by magnetic resonance imaging. Clin Orthop Relat Res 344: 275-283.
-
Zanetti M, Gerber C, Hodler J (1998) Quantitative assessment of the muscles of the rotator cuff with magnetic resonance imaging. Invest Radiol 33(3): 163- 170.
-
Warner JJ, Higgins L, Parsons IM 4th, Dowdy P (2001) Diagnosis and treatment of anterosuperior rotator cuff tears. J Shoulder Elbow Sur 10(1): 37-46.
-
Liu Z, Li Z, Qin M (2023) Comparative Analysis of MRI Findings of Mixed Rotator Cuff Tears and Rotator Cuff Lesions. J Chinese Journal of Forensic Sciences (4): 52- 56.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review