Sudden Deaths During Non-Competitive Sporting Activities: How Many Cases are Not Diagnosed and Correctly Coded Due to the Absence of an Autopsy?
The benefits of regular physical activity are well known, although sudden cardiac deaths have been described during competitive and non-competitive sports activities, unforeseen and unexpected. We describe three cases of sudden cardiac death, which occurred in three people under the age of 50 years. In all cases the autopsy revealed the presence of severe cardiomyopathies. We emphasize the importance of autopsy in all cases of unexpected deaths of people under 50 years of age; unfortunately, this is not always practiced in Italy at the moment.
Abbreviations
SCD: Sudden Cardiovascular Death.
Introduction
The benefits of regular physical activity are well known, and we know that elite athletes usually survive longer than the general population. However, we also know the legend of Philippides who, after running the first marathon in history, collapsed and died, showing how even fit people can die with exertion [1, 2, 3].
Important differences have been described in sudden deaths in athletes over the age of 35, which are mainly caused by atherosclerosis, compared to deaths under the age of 35, which are caused by inherited cardiac pathologies, particularly cardiomyopathies and ion channelopathies. The data emerging from the literature reveal that only a minority of cases have suffered from symptoms prior to death that could lead to suspicion of heart disease [4].
In a study that took into consideration 80 cases of sudden unexpected cardiac deaths during occasional amateur sporting activity, it was concluded that the lesions discovered in these cases are the same as those identified in cases of sudden cardiac death in professional athletes [5]. It is always of fundamental importance to carry out forensic autopsies to establish the exact cause of death in order to identify genetically transmissible anomalies, and therefore direct other family members to targeted check-ups.
Traumatic and devastating consequences of sudden sports-related deaths require us to fully understand this phenomenon in the general population [6, 7].
Clinical Report
We describe the sudden death of three people under 50 years of age during amateur sporting activity – all of whom were asymptomatic before death.
Case 1
During body building activities in the gym, a 49-year- old man had a cardiac arrest, and died before he reached the emergency room. A diagnostic autopsy was requested and performed.

Figure 1A: The Heart was Irregular in Shape; In Fact, the Left Ventricle had Increased Dimensions Compared to the Right Ventricle, which Appeared Small and Less Evident than the Left.
Figure 1B: The Myocardium of the Left Ventricle Measured 3.3 Cm Thick; The Myocardium of the Right Ventricle Measured 0.5 Cm Thick; and the Myocardium of the Interventricular Septum Measured 2.5 Cm Thick. The Myocardium Appeared of Increased Consistency when Cut and was a Brown/Reddish Color.

Figure 1C: Heart After Formalin Fixation. The Sections Allow us to See the Myocardium of the Left Ventricle with Thickened and Hypertrophic Walls to the Detriment of the Right Ventricle, with the Left Ventricle Showing an Obliterated Chamber.
Figure 1D: Histologically, the Myocardium Showed Myocardiocytic Hyperplasia/Hypertrophy.
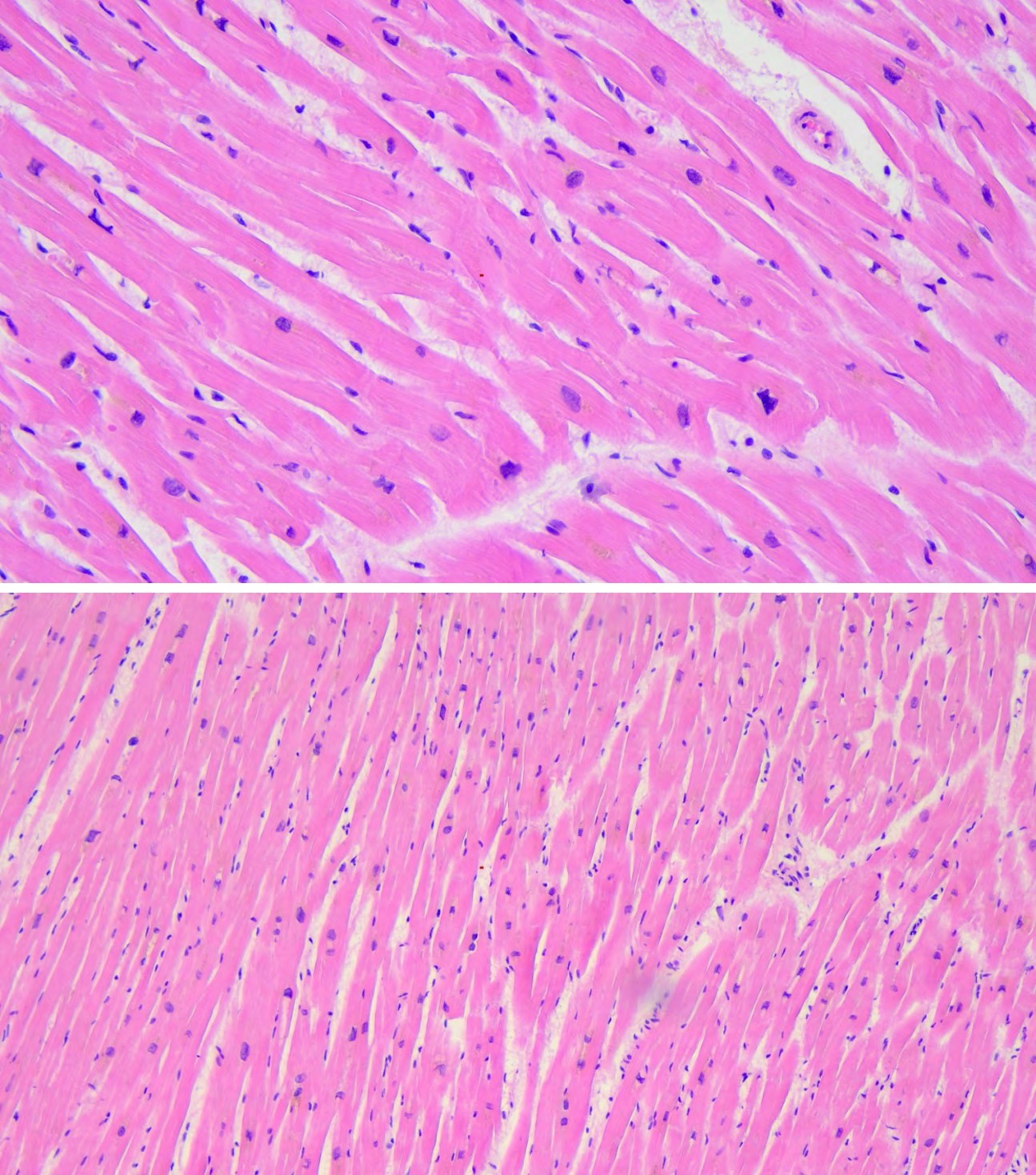
Figure 1E: Histologically, the Myocardium Showed Myocardiocytic Hyperplasia/Hypertrophy.
Figure 1E: Histologically, the Myocardium Showed Myocardiocytic Hyperplasia/Hypertrophy.
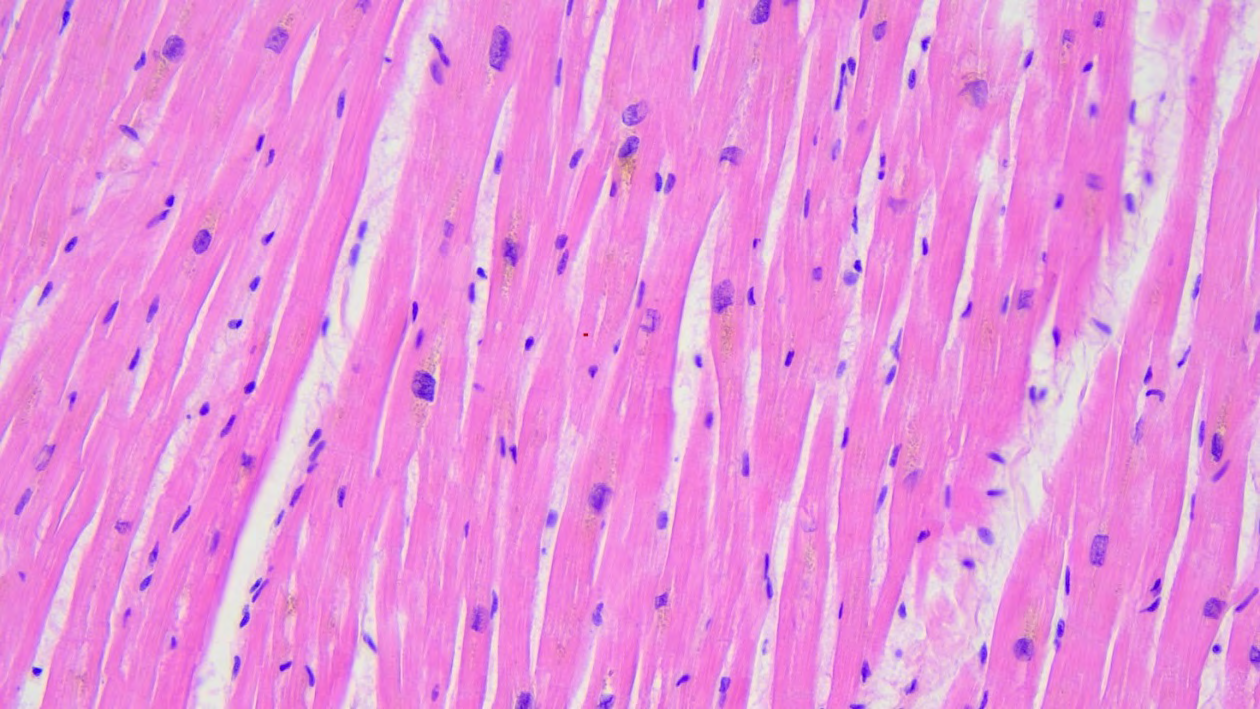
Figure 1F: Histologically, the Myocardium Showed Myocardiocytic Hyperplasia/Hypertrophy.
According to what his family reported, the man was apparently in good health; he skied and practiced various sporting activities.
Autopsy: Male subject (Caucasian), with an appearance consistent with his chronological age (49 years), of tall stature – approximately 180 cm – and of a robust build.
Among the findings of greatest interest, the heart, weighing 466 g, appeared to have an altered conformation due to the left ventricle having increased dimensions and consistency compared to the right ventricle which appeared flaccid and crouched. The myocardium of the left ventricle was 3.3 cm thick; the myocardium of the right ventricle was 0.5 cm thick; and the myocardium of the interventricular septum was 2.5 cm thick. The myocardium appeared of increased consistency when cut, and was a reddish colour.
The endocardium with tricuspid and mitral atrioventricular valves was without alteration; the aortic and pulmonary valves were normal; and aortic stenosis was excluded. The coronary arteries, examined in their entire course, did not present any significant lesions. Histologically, the myocardium showed myocardiocytic hyperplasia/ hypertrophy with focal areas of fibrosis.
Our conclusion was hypertrophic heart disease with substenosis of the aortic inflow from prevalvular myogenic hypertrophy. The morphological findings allowed us to interpret the outcome as a consequence of a major arrhythmic event in hypertrophic heart disease.
Upon our recommendation, the family members decided to go to a reference centre for hypertrophic and dilated cardiomyopathies. Upon initial screening, they were not found to be suffering from cardiac pathologies.
Subsequently, a myocardial sample from the deceased subject was analysed: The analysis of the panel of genes associated with hypertrophic cardiomyopathy highlighted the presence of the variant c.5287G>A p.(Ala1763Thr) in exon 37 of the MYH7 gene (OMIM* 160760) in a condition of heterozygosity.
According to the ACMG 2015 guidelines, specifically adapted for cardiomyopathies related to the MYH7 gene (Kelly MA et al., Genetics in Medicine 2018), the variant can currently be classified as probably pathogenic. The observed genotype could be compatible with the diagnosis of hypertrophic cardiomyopathy (CMH1,OMIM #192600). This variant is noted in ClinVar (Variation ID:177846) as a variant of uncertain significance; however, it is described in the literature in several patients with hypertrophic cardiomyopathy [8, 9, 10], in a patient with dilated cardiomyopathy [11] and in cases of sudden death [12].
Genetic counselling was recommended and this same mutation was identified in the man’s sister and in her son.
Case 2
A 12-year-old girl had a cardiac arrest at school during gymnastics class.
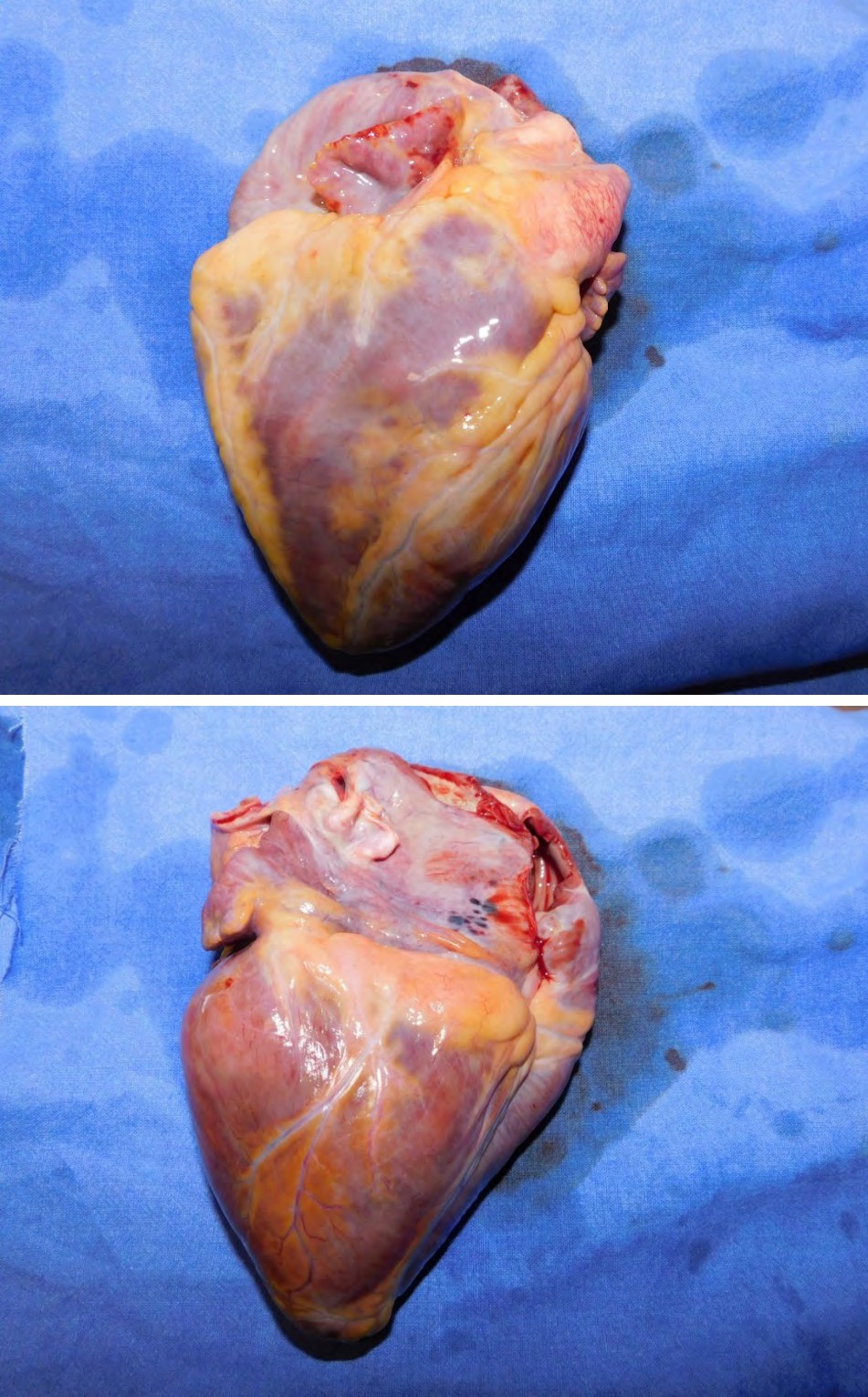
Figure 2A (Front Side): The Heart, as in the Previous Case, had a Left Ventricle of Much Greater Consistency than the Right Ventricle.
Figure 2A (Back Side): The Heart, as in the Previous Case, had a Left Ventricle of Much Greater Consistency than the Right Ventricle.

Figure 2C (Finding at the Autopsy Table): The Myocardium of the Left Ventricle Presented Thickened, Discolored and Hypertrophic Walls to the Detriment of the Right Ventricle.
Figure 2D (Finding After Fixation in Formalin): The Myocardium of the Left Ventricle Presented Thickened, Discolored and Hypertrophic Walls to the Detriment of the Right Ventricle.
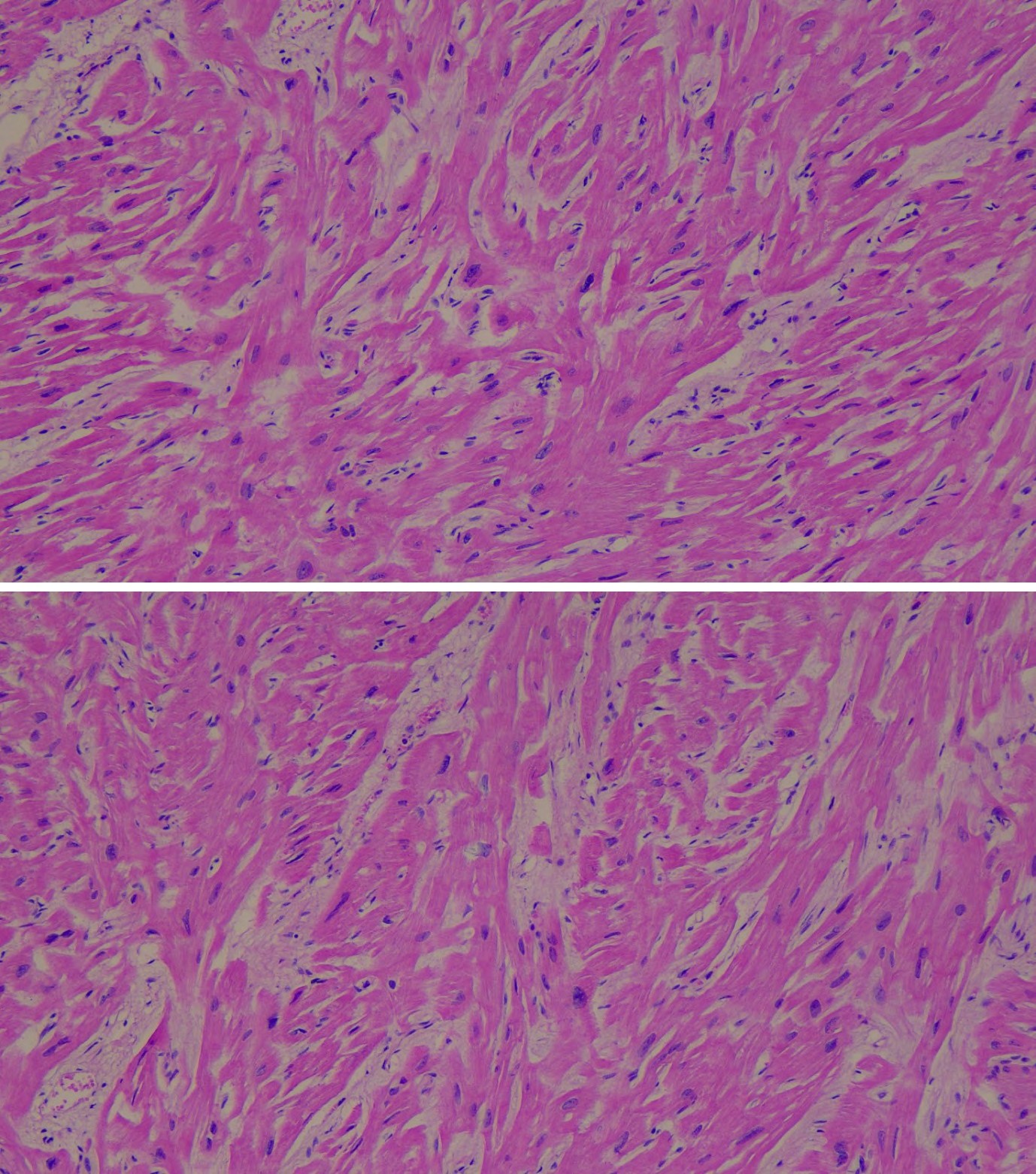
Figure 2E: Interventricular Septum and Left Ventricle Showed Disarrangement of Cardiomyocytes, Extremely Hypertrophic. In Fact, Myocardiocytes Showed Exaggerated Branching (Myocells that Took on Y-Shapes or Formed Vortices Around Vascular Connective Axes).
Figure 2F: Interventricular Septum and Left Ventricle Showed Disarrangement of Cardiomyocytes, Extremely Hypertrophic. In Fact, Myocardiocytes Showed Exaggerated Branching (Myocells that Took on Y-Shapes or Formed Vortices Around Vascular Connective Axes).
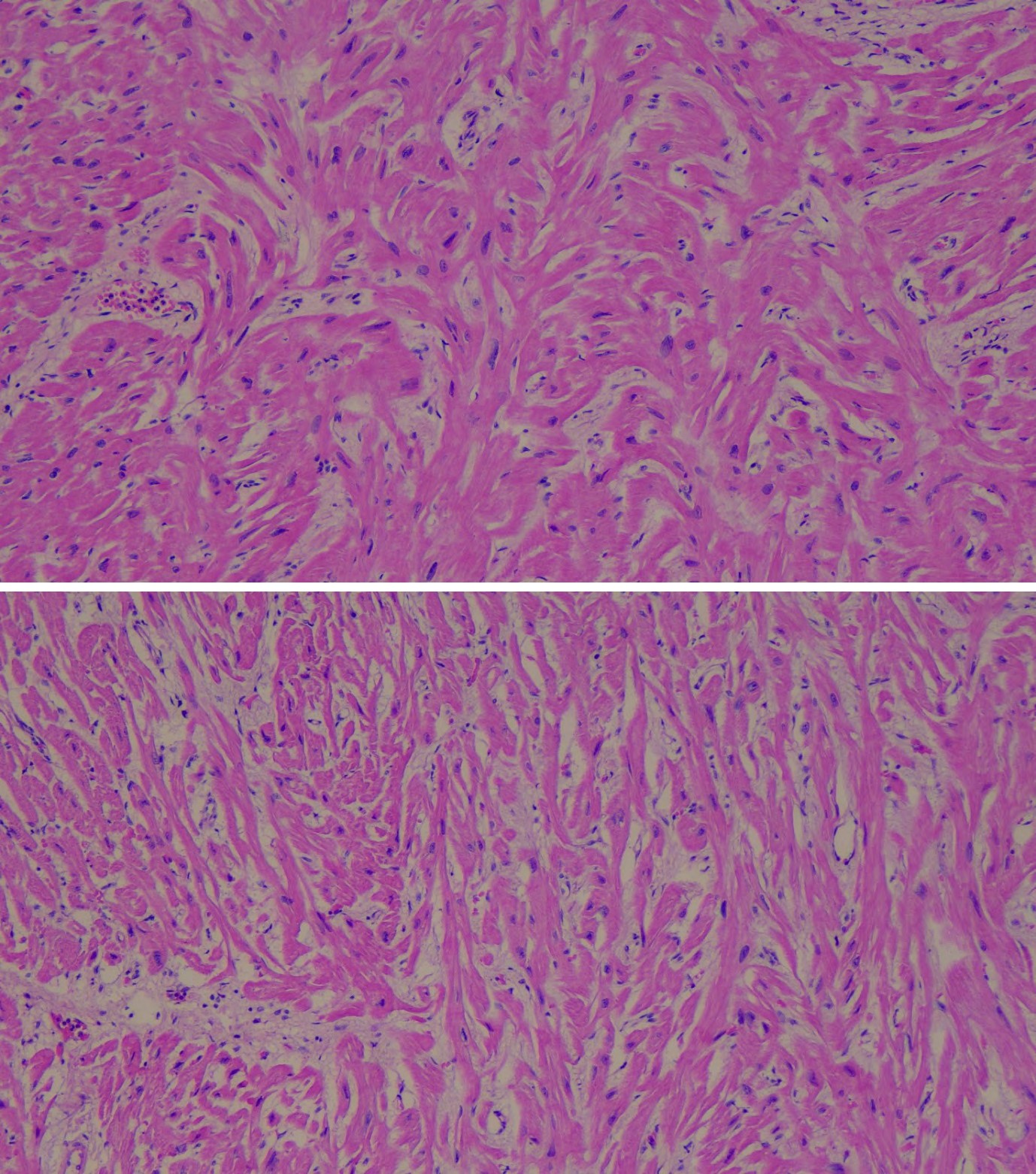
Figure 2G: Interventricular Septum and Left Ventricle Showed Disarrangement of Cardiomyocytes, Extremely Hypertrophic. In Fact, Myocardiocytes Showed Exaggerated Branching (Myocells that Took on Y-Shapes or Formed Vortices Around Vascular Connective Axes).
Figure 2H: Interventricular Septum and Left Ventricle Showed Disarrangement of Cardiomyocytes, Extremely Hypertrophic. In Fact, Myocardiocytes Showed Exaggerated Branching (Myocells that Took on Y-Shapes or Formed Vortices Around Vascular Connective Axes).
She was promptly transferred to the emergency room of the nearest hospital. She had no peripheral pulses, was cyanotic and with eyes in fixed mydriasis. She was resuscitated without success and her death was confirmed. A diagnostic autopsy was requested and performed.
Autopsy: Female subject, Caucasian, with appearance and height consistent with the age of 12 years, who was of slim build.
Among the most interesting findings were: bilateral serohaematic pleural effusion (600 cc on the right and 150 cc on the left); bilateral pleural adhesions more evident on the right, and a serous pericardial effusion of 90 cc. Her heart weighed 237g and measured 11×12×6 cm; the left ventricle, as in the previous case, appeared to be much larger than the right ventricle. The myocardium of the left ventricle had a maximum thickness of 2.3 cm; the myocardium of the right ventricle had a maximum thickness of 1 cm; and the myocardium of the interventricular septum had a maximum thickness of 1.5 cm. The endocardium had tricuspid and mitral atrioventricular valves and normal-shaped aortic and pulmonary valves. The lung weight was increased compared to the normal weight due to bilateral pulmonary oedema. The weight of the heart, lungs and liver was above normal for a female in the 13th year of her life [13]. The average heart weighs 177 compared to 237 in the case in question; the average right lung weighed 346 compared to 505; the average left lung weight 297 compared to 420; and the average liver weight 1050 compared to 1277 (even exceeding the maximum possible expected values). These results suggested a cardiocirculatory overload, but not of recent onset.
Histologically, the interventricular septum and left ventricle showed disarray of cardiomyocytes, which were extremely hypertrophic with myocytes that had exaggerated branching (myocytes that assumed Y-shapes or formed vortices around connective-vascular axes). Overall, the myocardial tissue in all samples taken from the left ventricle and the interventricular septum presented an architectural disarray characterised by the loss of orientation in parallel bundles and the presence of numerous ramifications plus a vortex arrangement of the myocells. There was an increase in interstitial fibrous tissue (also highlighted with Masson’s trichrome histochemical staining).
The death was therefore classified as malignant arrhythmia in congenital heart disease with unrecognised right atrial dilation and disarray of the left ventricular myocardial tissue and interventricular septum. Our diagnostic hypothesis was that of hypertrophic cardiomyopathy. Subsequently, all of the child’s family members underwent cardiac tests at a heart disease referral centre but were found not to suffer from heart disease. However, no molecular testing was performed.
Case 3
A 31-year-old woman had a sudden attack of shortness of breath during Fitwalking activities; the health emergency number was called, but she died before arriving at the hospital. Based on the anamnestic data collected, the woman had never suffered from particular pathologies and was the mother of a 5-year-old child. A diagnostic autopsy was requested and performed.

Figure 3A: Also in this Case, The Left Ventricle was Hypertrophic with Ventricular Cavity Almost Completely Obliterated.
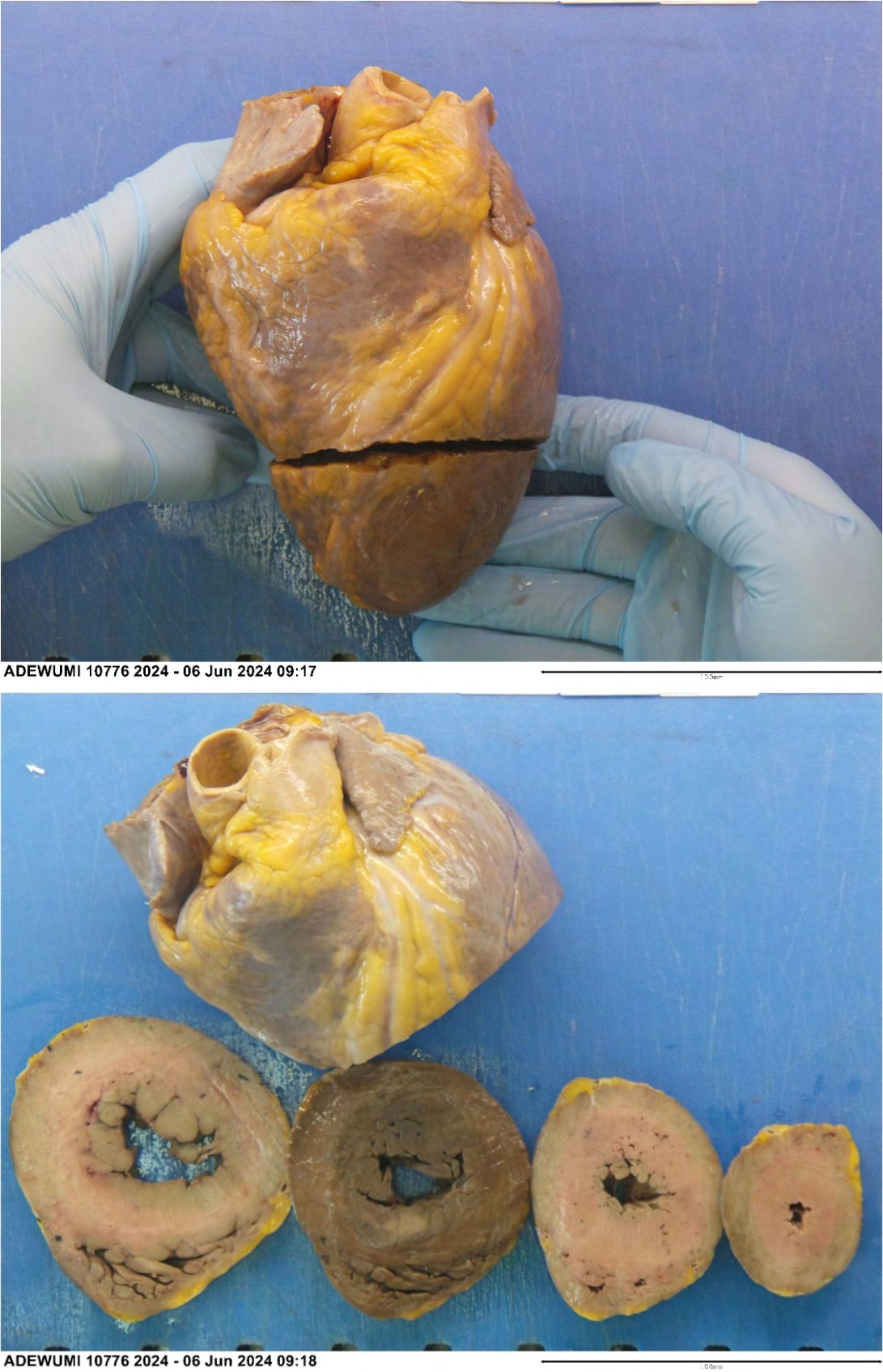
Figure 3B: Also in this Case, The Left Ventricle was Hypertrophic with Ventricular Cavity Almost Completely Obliterated.
Figure 3C: Also in this Case, The Left Ventricle was Hypertrophic with Ventricular Cavity Almost Completely Obliterated.
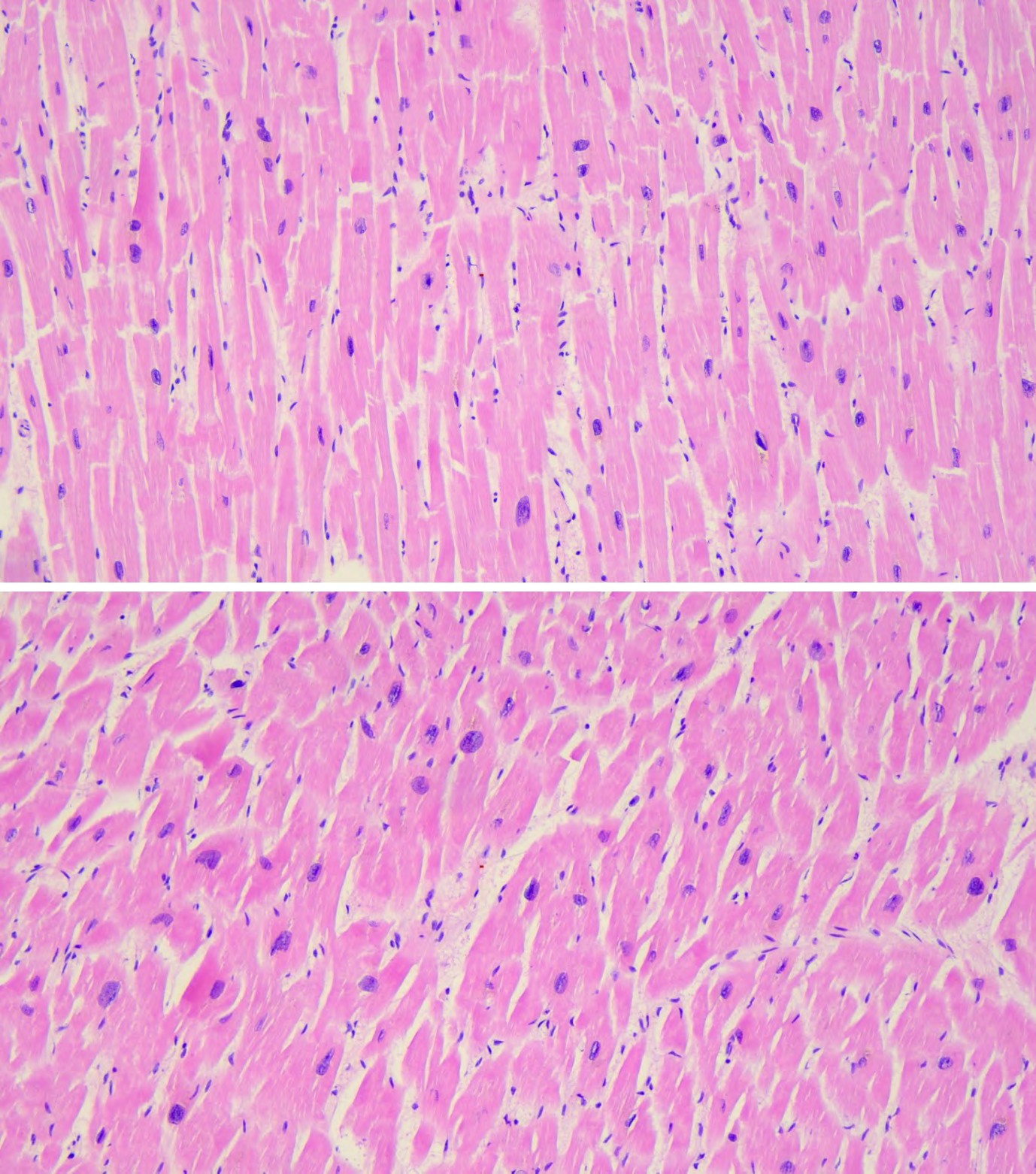
Figure 3D: The Cardiomyocytes, in the Samples Taken from the Left Ventricular Septum and Wall, were Diffusely Hypertrophic.
Figure 3E: The Cardiomyocytes, in the Samples Taken from the Left Ventricular Septum and Wall, were Diffusely Hypertrophic.
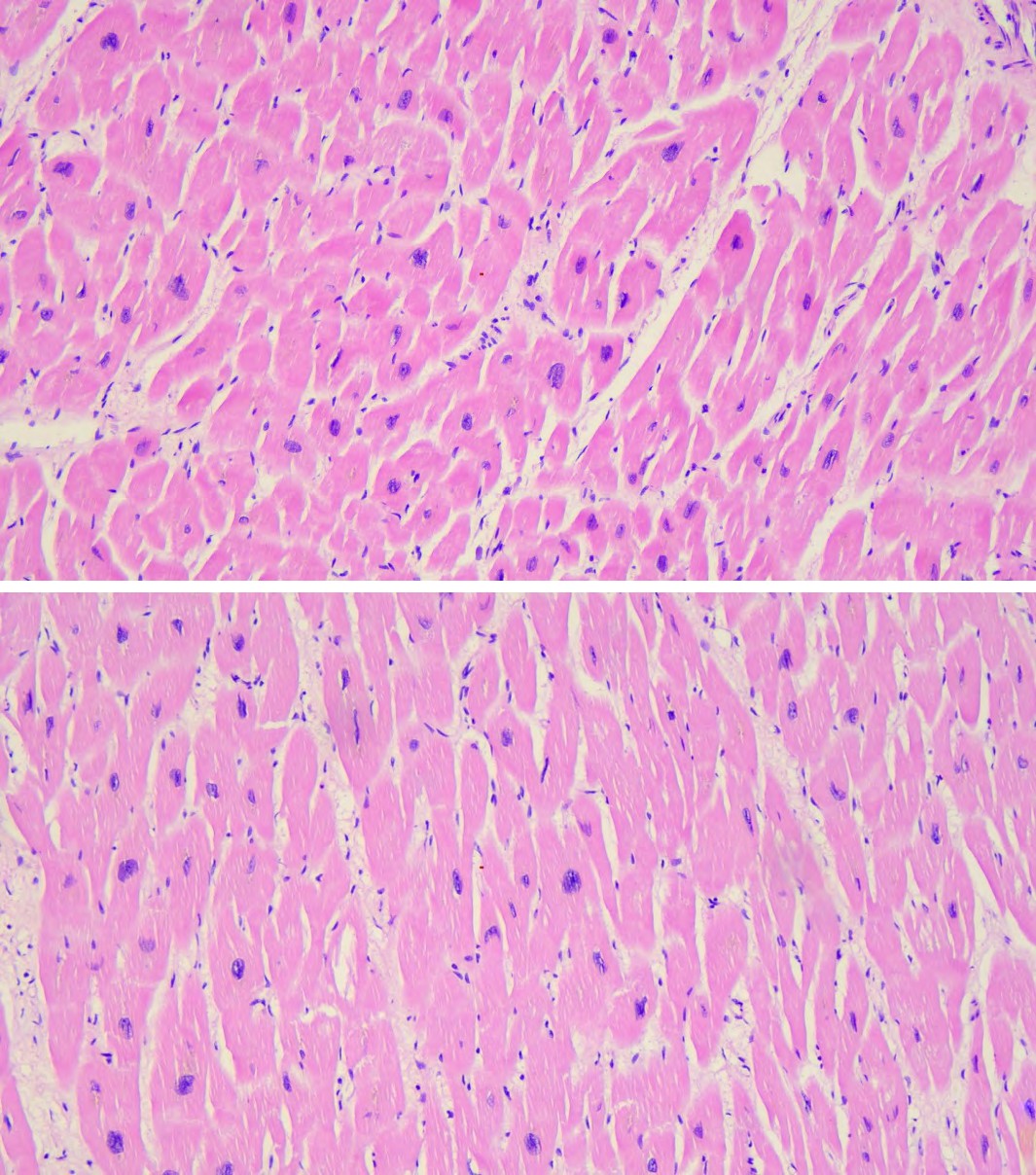
Figure 3F: The Cardiomyocytes, in the Samples Taken from the Left Ventricular Septum and Wall, were Diffusely Hypertrophic.
Figure 3G: The Cardiomyocytes, in the Samples Taken from the Left Ventricular Septum and Wall, were Diffusely Hypertrophic.
Autopsy: A female subject (Nigerian), with an appearance consistent with her chronological age (31 years), of normal stature – approximately 165 cm –with a robust build.
Among the findings of greatest interest was the heart in this case (like the previous two), which weighed 450g, had an altered conformation with a hypertrophic left ventricle in the absence of aortic valve alterations. In fact, the myocardium of the left ventricle was 3 cm thick; the myocardium of the right ventricle was 0.5 cm thick; and the myocardium of the interventricular septum was 2 cm thick. The myocardium appeared fleshy in consistency and reddish in colour. The coronary arteries, examined in their entire course, presented regular calibre and the absence of alterations. Histologically, the myocardium showed myocardiocytic hyperplasia/ hypertrophy. Our conclusion was hypertrophic heart disease.
Also in this case, morphological findings allowed us to interpret the outcome as a consequence of a major arrhythmic event in hypertrophic heart disease. The urine and venous blood of the two adult subjects were tested for amphetamines/methamphetamines/MDMA, ketamine, cannabinoids, cocaine, opiates, benzodiazepines, barbiturates, antidepressants and alcohol; the results were negative for all substances. In the child we considered it useless to conduct this type of examination.
Discussion
A competitive athlete is different from younger and older populations who participate in recreational activities (i.e. a heterogeneous group of adults participating in a running race). The cases under consideration refer to these latter types of athletes, even if engaged in different and non- homogeneous physical activities.
In fact, in the first case, the man was doing body-building activities in the gym; in the second case, the girl was doing sports in the gym at school; in the third case, the woman was doing Fitwalking on a nature trail.
The benefits of physical activity are irrefutable. However, many of these benefits are attributable to moderate exercise, whereas athletes exert efforts well beyond recommended levels of physical activity and consistently push back the frontiers of human endurance [14].
Sudden death in athletes is a rare event, but has been known and studied for a long time. Many studies have focused only on young and competitive athletes; in fewer cases the focus has been on a wider population of amateur athletes [15].
Competitive sports are associated with an increased risk of sudden cardiovascular death (SCD) in adolescents and young adults with clinically silent cardiovascular disease. While coronary atherosclerosis represents the vast majority of SCD in middle-aged/senior athletes, the spectrum of substrates in young athletes is broader and includes hereditary (cardiomyopathies) and congenital structural heart disease (anomalous origin of the coronary arteries) [16].
Screenings were performed on young competitive athletes to assess the risk of sudden death [17].
In some underlying and often silent cardiac pathologies, physical exercise performed with intensity and regularity, the phenomena of pathological cardiac adaptation, physical fitness, lifestyle and the presence of cardiovascular risk factors that are not controlled and often go unobserved by the athletes themselves, are conditions that may counteract the benefit of physical exercise. In contrast and exceptionally, these conditions may trigger a cardiovascular problem that can cause the sudden death of the athlete – a phenomenon with high social and media impact [18, 19, 20].
In the absence of clinical information that can explain the reason for sudden death in people under 50 years of age, an autopsy should always be performed. Correct autopsy diagnosis is an indispensable step in establishing the pathology underlying SCD and is essential in determining which screening procedures the victim’s relatives should undergo; however, data suggest that an autopsy is not always performed [21, 22].
In a study of Danish boys Winkel BG, et al. [23], in two- thirds of all cases of unexpected death, there was no prior medical history that would point to a problem. After autopsy, in 70% of cases, the causes of death were cardiac or unknown.
Another study conducted on adolescents in the UK Finocchiaro G, et al. [24] highlighted how sudden cardiac death can be caused by a spectrum of cardiac conditions. There are cases that occurred during rest (80%) and other cases that occurred during physical exercise. In athletes, sudden death occurs more frequently during exercise than in non-athletes. Coronary artery anomalies and hypertrophic cardiomyopathy are among the most frequent causes. The authors suggest that patients with hypertrophic cardiomyopathy may be particularly vulnerable to exercise- induced arrhythmias.
In a study on sudden cardiac death in young people, which was conducted on autopsies in Sweden [25], the most frequent cause of death was arrhythmic (31% of cases), while hypertrophic heart disease represented 5%. Death occurring during physical activity represented 14% of the cases examined in that study.
In Sweden [25], the legislation stipulates that in cases of this type – sudden deaths especially in young people – the police are always informed, which means that forensic autopsies are often arranged. If this does not happen, it is possible that in this type of case the deceased person will be sent to hospital to undergo a clinical autopsy.
In the UK, when a young person dies suddenly, the coroner is responsible for establishing the cause of death; they will usually use a consultant pathologist to carry out the autopsy in order to establish how and when the death occurred [26]. In selected cases, the coroner will use cardiac pathologists.
In Italy there is a law from 1990 [27], a new law on the matter has been awaited for some years.
Conclusions
Sudden cardiac death is an utterly tragic and unexpected event that can occur in young people and adults even in apparently good health. No death under the age of 50 in apparently healthy subjects should be considered a natural event and therefore deserves an accurate autopsy investigation.
It is always essential to carry out autopsies in cases of sudden death in young subjects, in order to screen all the deceased’s family members to highlight and treat any unknown cardiac pathologies.
It is evident that in many countries it is almost automatic to perform autopsies in cases of this type; however, in Italy, there is no guarantee that in these cases a diagnostic hospital autopsy is always carried out. Also, if there is no indication of a crime, there is no certainty that such a case is subjected to an autopsy. This is extremely serious because essential information is not discovered both from an epidemiological point of view and for the direct relatives of the deceased patient who could be unknowingly suffering from the same heart disease.
In Italy, professional athletes are certainly carefully studied and evaluated from a cardiological point of view, and previously unknown pathologies are occasionally identified and reveal that the athlete is not suitable for competitive sports.
However, for non-competitive activities, medical investigations are much less thorough. In our country, this situation is currently managed through agreements – which are more or less formalised depending on the reality – between the judiciary, hospitals, university forensic medicine institutes, pathologists and freelance professionals.
In such a context, how many cases of sudden death from serious heart disease during non-competitive sports activities or during everyday activities go unnoticed and uncoded?
It is time to seriously discuss and again forcefully reject the unhealthy custom – which already exists in some areas of Italy – of not performing an autopsy and thereby limiting the discovery of the true cause of death.
This study was carried out at the Pathology Unit of the “A. Cardarelli” Regional Hospital of Campobasso, Italy.
Authors’ Contributions
Massimiliano Guerriero performed the three autopsies and prepared the manuscript. The biomedical laboratory technician Raimondo Carnevale helped during the execution of the autopsies. The laboratory technician Domenico Consiglio processed the tissues and prepared all the slides.
Ethics Statement
We obtained written consent from the relatives of the deceased for the use of these cases for teaching and research.
We ensured in the text that no reference was made to the deceaseds’ identities.
The manuscript is in accordance with the rules of the Institutional Ethics Committee.
Conflict of Interest
None.
Financial Support
None.
References
-
Teramoto M, Bungum TJ (2010) Mortality and longevity of elite athletes. J Sci Med Sport 13(4): 410-416.
-
Lemez S, Baker J (2015) Do elite athletes live longer? A systematic review of mortality and longevity in elite athletes. Sports Med Open 1(1): 16.
-
Whang W, Manson JE, Hu FB, Chae CU, Rexrode KM, et al. (2006) Physical exertion, exercise, and sudden cardiac death in women. JAMA 295(12): 1399-1403.
-
de Noronha SV, Sharma S, Papadakis M, Desai S, Whyte G, et al. (2009) Aetiology of sudden cardiac death in athletes in the United Kingdom: a pathological study. Heart 95(17): 1409-1414.
-
Tabib A, Miras A, Taniere P, Loire R (1999) Undetected cardiac lesions cause unexpected sudden cardiac death during occasional sport activity. A report of 80 cases. Eur Heart J 20(12): 900-903.
-
Waldmann V, Bougouin W, Karam N, Albuisson J, Cariou A, et al. (2017) Mort subite de l’adulte : une meilleure compréhension pour une meilleure prévention [Sudden cardiac death: A better understanting for a better prevention]. Ann Cardiol Angeiol (Paris) 66(4): 230-238.
-
Jouven X, Bougouin W, Karam N, Marijon E (2015) Épidémiologie de la mort subite: données du registre francilien Rev Prat 65(7): 916-918.
-
Alfares AA, Kelly MA, McDermott G, Funke BH, Lebo MS, et al. (2015) Results of clinical genetic testing of 2,912 probands with hypertrophic cardiomyopathy: expanded panels offer limited additional sensitivity. Genet Med 17(11): 880-888.
-
(2015) Correction: Corrigendum: Results of clinical genetic testing of 2,912 probands with hypertrophic cardiomyopathy: expanded panels offer limited additional sensitivity Genet Med 17(4): 319.
-
Bos JM, Will ML, Gersh BJ, Kruisselbrink TM, Ommen SR, et al. (2014) Characterization of a phenotype-based genetic test prediction score for unrelated patients with hypertrophic cardiomyopathy. Mayo Clin Proc 89(6): 727-737.
-
Walsh R, Thomson KL, Ware JS, Funke BH, Woodley J, et al. (2017) Reassessment of Mendelian gene pathogenicity using 7,855 cardiomyopathy cases and 60,706 reference samples. Genet Med 19(2): 192-203.
-
Broch K, Andreassen AK, Hopp E, Leren TP, Scott H, et al. (2015) Results of comprehensive diagnostic work-up in ‘idiopathic’ dilated cardiomyopathy. Open Heart 2(1): e000271.
-
Dewar LJ, Alcaide M, Fornika D, D’Amato L, Shafaatalab S, et al. (2017) Investigating the genetic causes of sudden unexpected death in children through targeted next- generation sequencing analysis. Circ Cardiovasc Genet 10(4): e001738.
-
Reid WA (1988) Height and weight in human beings. Autopsy report. J Clin Pathol 41(2): 237.
-
Sharma S, Merghani A, Mont L (2015) Exercise and the heart: the good, the bad, and the ugly. Eur Heart J 36(23): 1445-1453.
-
Dennis M, Elder A, Semsarian C, Orchard J, Brouwer I, et al. (2018) A 10-year review of sudden death during sporting activities. Heart Rhythm 15(10): 1477-1483.
-
Corrado D, Zorzi A (2017) Sudden death in athletes. Int J Cardiol 237: 67-70.
-
Sarto P, Zorzi A, Merlo L, Vessella T, Pegoraro C, et al. (2023) Value of screening for the risk of sudden cardiac death in young competitive athletes. Eur Heart J 44(12): 1084-1092.
-
Cordero A, Masiá MD, Galve E (2014) Physical exercise and health. Rev Esp Cardiol 67(9): 748-753.
-
Boraita A (2002) Sudden death and sport. Is there a feasible way to prevent it in athletes?. Rev Esp Cardiol 55(4): 333-336.
-
Pineda J, Marín F, Cordero A, Giner C, Quiles JA, et al. (2016) Sport, health and sudden death. Int J Cardiol 221: 230-231.
-
Banner J, Basso C, Tolkien Z, Kholova I, Michaud K, et al. (2021) Autopsy examination in sudden cardiac death: a current perspective on behalf of the Association for European Cardiovascular Pathology. Virchows Arch 478(4): 687-693.
-
Winkel BG, Risgaard B, Sadjadieh G, Bundgaard H, Haunsø S, et al. (2014) Sudden cardiac death in children (1-18 years): symptoms and causes of death in a nationwide setting. Eur Heart J 35(13): 868-875.
-
Finocchiaro G, Radaelli D, D’Errico S, Papadakis M, Behr ER, et al. (2023) Sudden cardiac death among adolescents in the United Kingdom. J Am Coll Cardiol 81(11): 1007-1017.
-
Wisten A, Krantz P, Stattin EL (2017) Sudden cardiac death among the young in Sweden from 2000 to 2010: an autopsy-based study. Europace 19(8): 1327-1334.
-
Sheppard MN (2012) Aetiology of sudden cardiac death in sport: a histopathologist’s perspective. Br J Sports Med 46 (S1): i15-21.
-
(1990) (Approval of) New Mortuary Police Regulations. Italian Presidential Decree of 10 August 1990, 285.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review