Management of Sinonasal Melanoma: Case Report
patient aged of 70 years old presented a 6 months history of a right nasal bleeding and blockage. He was diagnosed with mucosal malignant melanoma. Loco regional extension in the CT and MRI showed involvement of the frontal sinus, sphenoidal sinus and suspected involvement of the medial wall of the orbit. He had surgical excision with removal of the tumor. Given the positive margins, adjuvant radiotherapy was indicated. The radiotherapy was delivered with intensity modulated radiation therapy (IMRT) technique in order to overcome anatomical complexity of the region, cover the tumor bed and preserve the organs at risk. Despite advances in techniques, there is still no impact on the overall survival.
and Khalid Hassouni1
Morocco, Tel: +212619948046; E-mail: aiterraissemohamed@gmail.com
Keywords: Melanoma; Sinus; Paranasal; Radiotherapy; IMRT
Introduction
Mucosal malignant melanoma of the nasal cavity and paranasal sinuses is a rare tumor. It is generally managed with an aggressive surgical approach with the intention of complete excision of the tumor followed by adjuvant radiotherapy. The sino-nasal region is difficult to treat and delivering radical doses of radiotherapy is challenging. IMRT radiation technique helps treating this site with a good compromise between efficacy and safety. Prognosis, however, is generally poor even with this aggressive treatment strategy.
The case
This is a 70 years old married man, father of 5 children, works as a salesman, who is treated for type 2 diabetes under insulin therapy. He is a chronic smoker (for 30 years) and had a cholecystectomy 20 years ago. There is no other event in his medical history. The starting of symptoms goes back to 6 months earlier when the patient presented an intermittent bleeding from the right nasal cavity with homolateral nasal blockage. After unsuccessful symptomatic treatment prescribed by a general practitionner, he consulted an ENT (ear - nose- throat) specialist. He proceeded with a nasofibroscopy that showed a tumor of the nasal cavity with posterior extension to the choana. A biopsy was made.
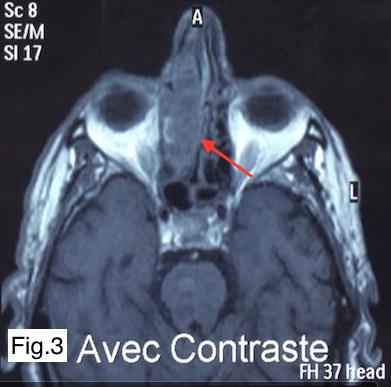
After pathological examination, the biopsy of the tumorturned out to be a poorly differentiated malignant tumor suspected to be a melanoma. The patient was investigated with a CT scan of the paranasal sinuses, which revealed a soft tissue lesion in the right nasal cavity that was extending into the right ethmoid sinus with no regional lymphnodes (Figure 1). The magnetic resonance imaging (MRI) showed that the tumor was very close to the floor of the sphenoid sinus and the right frontal sinus with suspicion of involvement of the floor of the orbit (Figure 2,3). Further staging assessment, which included CT scan of the chest and abdomen, was carried out with no evidence of distant metastasis.
International Journal of Nuclear Medicine & Radioactive Substances


The patient underwent a tumor excision with a right lateral rhinotomy. The surgery removed the maximum tumor bulk from the sino-nasal region with excision of the lacrymo-nasal canal. The histopathology of the surgical specimen was consistent with mucosal malignant achromic melanoma. The margins could not be specified. The lacrymo-nasal canal was not involved by the melanoma.
This case was then discussed in a head and neck tumor board. Considering the extent of the tumor, it was staged as T4aN0M0 as per the 2013 AJCC Staging. Adjuvant radiotherapy was decided.
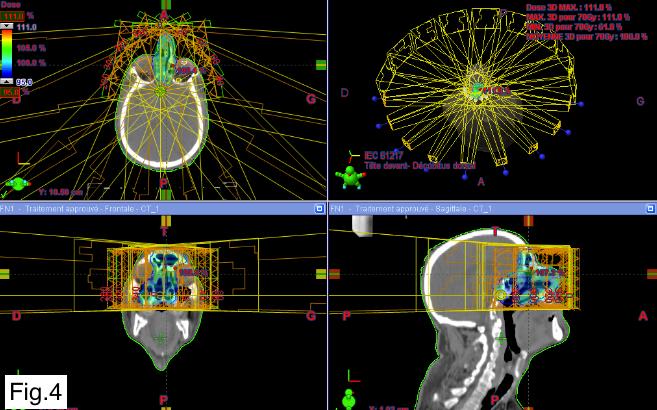
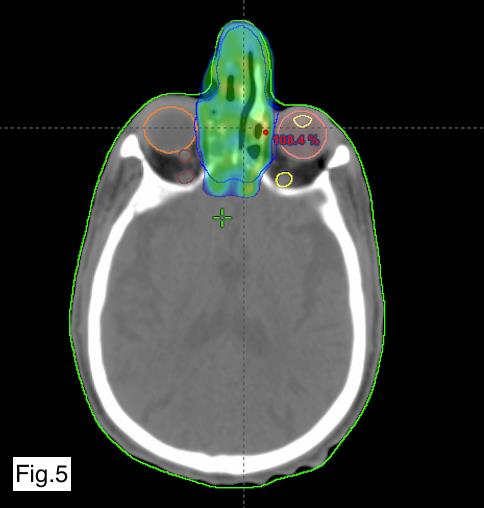
He was planned for a total dose of 66 Gy of RT in 33 fractions, at a daily dose fraction of 2 Gy over 6.5 weeks using the IMRT technique. We were able to keep the tolerance doses of organs at risk such as the optic chiasma, optic nerves, retina, pituitary and parotids within normal limits and at the same time deliver the intended dose of radiation to the tumor site (Figures 4 & Figure 5). The patient received treatment according to plan and the tolerance was good. He was reviewed weekly during the treatment by our team. There were no significant side effects observed except moderate skin reactions on the irradiated skin and occasional right nasal blockage at the end of treatment.
International Journal of Nuclear Medicine & Radioactive Substances
The patient was reviewed after 1 month. Skin reactions almost resolved. The patient was doing well. ACT scan will be performed after 2 months to check on the treatment response.
Discussion
Primary mucosal melanoma of the nasal cavity and paranasal sinuses is a rare tumor [1, 2]. It represents between 4 and 8% of malignant tumors of the nasal cavity and paranasal sinuses [3]. The age at the time of diagnosis is between 60 and 80 years with a mean age between 65 and 70 years [4].
The common symptoms are nasal obstruction and epistaxis [5]. Tumors of the nasal cavity predominantly involve the septum and lateral wall, while tumors of the paranasal sinuses predominantly involve the maxillary sinus followed by the ethmoid, frontal and sphenoidal sinuses [6]. The diagnosis is histological. Imaging assessment includes computed tomography (CT) (for bony structures). Magnetic resonance imaging (MRI) is essential for local and regional staging of the tumor [7]. It defines the tumor extension to the orbit and skull base and also shows brain metastases. Distant staging is based on PET/CT or chest, abdomen and pelvic CT.
The established therapeutic modality is a complete resection of the tumor with clear margins followed by adjuvant radiotherapy [8]. Surgery is indicated as first- line treatment and in the case of local recurrence.
Radiotherapy is classically indicated in the presence of positive surgical margins, local recurrence, and locally advanced tumor. It also used as a palliative treatment.
Radiotherapy increases local and regional control without increasing survival independently of tumor stage [9]. New techniques in radiotherapy, such as intensity- modulated radiation therapy (IMRT) has improved the results on local and regional control with more safety and lower morbidity [10].
Combs et al reported that IMRT showed good results with respect to local control as well as survival, while treatment related toxicities were minimized. After IMRT, local progression-free survival was 71.4% at 1 year and 75% at 3 years [11]. To obtain local control, the radiotherapy doses need to be radical [12].
Modern radiotherapy techniques such as IMRT allow high doses to target volumes, while sparing organs at risk such as the optic chiasma, optic nerves, retina, pituitary, parotids, temporal lobes and auditory structures (including the cochlea and optic structures)[13].
Chemotherapy is classically indicated for palliative treatment or in metastatic patients. Targeted therapy such as s, a BRAF protein kinase inhibitor, is therefore reserved for the treatment of advanced melanoma associated with BRAF mutation [14].
Surviving beyond 5 years will be less expected for the majority of patients with head and neck MMs [15]. Local recurrences have been reported to be ranging from 40% to 79.4%. Distant metastases are also common, with reports ranging from 19.2% to 64.3%. Manolidis, et al. noted a 51.5% rate of distant failure in a pooled analysis from 332 patients [16].
Conclusions
Early diagnosis of mucosal melanoma of the nasal cavity is an essential prognostic factor. First-line treatment is based on wide surgical resection, followed by radiotherapy with modern techniques such as IMRT. Current treatment modalities have not significantly made an impact on the survival .The overall prognosis of these tumors is very poor. Given the rarity of the disease there is a need for multi- centric collaboration that will establish clinical guidelines.
International Journal of Nuclear Medicine & Radioactive Substances
References
-
ChanRC, ChanJYW, Wei WI (2012) Mucosal melanoma of the head and neck: 32-year experience in a tertiary referral hospital. Laryngoscope 122(12): 2749-2753.
-
Marcus DM, Marcus RP, Prabhu RS, Taofeek K Owonikoko, David H Lawson, et al. (2012)Rising incidence of mucosal melanoma of the head and neck in the United States. J Skin Cancer 1-6.
-
Mihajlovic M, Mihajlovic S, Jovanovic P, Stefanovic V (2012) Primary mucosal melanomas: a comprehensive review. Int J Clin Exp Pathol 5(8): 739-753.
-
Patrick RJ, Fenske NA, Messina JL (2007) Primary mucosal melanoma. J Am Acad Der- amatol 56(5): 828-834.
-
Moreno MA, Roberts DB, Kupferman ME, DeMonte F, El-Naggar AK, et al. (2010) Mucosal melanoma of the nose and paranasal sinuses, a contemporary experience from the MD Anderson Cancer Center. Cancer 116(9): 2215-2223.
-
Saint-Blancard P, Kossowski M (2006) Mélanomes des muqueuses nasosinusiennes. Presse Med 35(11): 1660-1663.
-
GilainL, Houette A, Montalban A, Mom T, Saroul N (2014) Mucosal melanoma of the nasal cavity and paranasal sinuses. European Annals of Otorhinolaryngology, Head and Neck diseases 131(6): 365-369.
-
Karim MU, Khan K, Ali N, Ikram M (2015) Sino-nasal mucosal malignant melanoma. BMJ Case Rep.
-
Benlyazid A, Thariat J, Temam S, Malard O, Florescu C, et al. (2010) Postoperative radiotherapy in head and neck mucosa melanoma: a GETTEC study. Arch Otolaryngol Head Neck Surg 136(12): 1219-1225.
-
Khan MK, Khan N, Almasan A, Roger Macklis (2011) Future of radiation therapy for malignant melanoma in an era of newer, more effective biological agents. Oncol Targets Ther 4: 137-148.
-
Combs SE, Konkel S, Thilmann C, Debus J, Schulz Ertner D (2007) Local high-dose radiotherapy and sparing of normal tissue using intensity-modulated radiotherapy (IMRT) for mucosal melanoma of the nasal cavity and paranasal sinuses. Strahlenther Onkol 183(2): 63-68.
-
Gilligan D, Slevin NJ (1991) Radical radiotherapy for 28 cases of mucosal melanoma in the nasal cavity and sinuses. Br J Radiol 64(768):1147-1150.
-
Lohia S, Rajapurkar M, Nguyen SA, Sharma AK, Gillespie MB, et al. (2014) A comparison of outcomes using intensity-modulated radiation therapy and 3- dimensional conformal radiation therapy in treatment of oropharyngeal cancer. JAMA Otolaryngol Head Neck Surg 140(4): 331-337.
-
Flaherty KT, Kim KB, Ribas A, McArthur GA, Sosman JA, et al. (2010) Inhibition of mutated, activated BRAF in metastatic melanoma. N Engl J Med 363(9): 809- 819.
-
Bachar G, Loh KS, O’Sullivan B, Goldstein D, Wood S, et al. (2008) Mucosal melanomas of the head and neck: experience of the Princess Margaret Hospital. Head Neck 30: 1325-1331.
-
Manolidis S, Donald PJ (1997) Malignant mucosal melanoma of the head and neck; review of the literature and report of 14 patients. Cancer 80(8): 1373-1386.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO